CHAPTER 11 Methods of analysing gait
Introduction
Gross abnormalities, such as a patient with a marked limp or a child who is a toe walker, are relatively easy to visually identify. Minor variations from the ‘normal’ are harder to spot and describe in a meaningful way. This is not surprising given that it only takes 650 ms to complete one full gait cycle and the human eye cannot perceive events that occur in less than 83 ms (Gage & Ounpuu 1989). Practitioners are, therefore, increasingly looking towards methods of investigating gait in a systematic way that provides accurate, reproducible and quantitative data.
How can gait by analysed?
Clinically based gait analysis methods include observation and simple quantitative methods that can provide useful data. Observation of a patient’s gait can be assisted by the use of video and treadmills. Simple quantitative measures can be made with techniques using paper, pen, tape measure and stop watch. Clinically based methods are simple to use, provide repeatable data, and are relatively easy and quick to interpret. They are also relatively low tech.
Observation of gait
Observational or visual gait analysis is the analysis of a subject’s gait without the use of any equipment, and is one of the more useful and widely used clinical tools available to practitioners. The analysis of gait in this way is subjective and needs a substantial understanding of normal gait (Kirtley 2006, Perry 1992, Whittle 2001).
Observational gait analysis involves watching a person walk up and down an area that allows sufficient space for up to 10 steps, usually a corridor in the clinical setting. Any relevant deviations from the assumed normal are noted. Observational gait analysis is best done by systematically concentrating on one body part at a time, then another, and usually one limb at a time. However, this skill takes time to develop, with novices more erratic in their observation of body regions (Ford 2001) (Fig. 11.1).
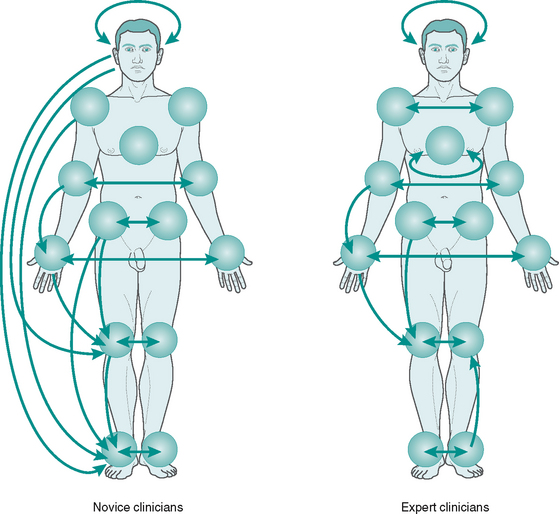
Figure 11.1 State transition diagrams demonstrating visual transitions and fixations with a probability higher than 0.2 in novice and expert clinicians. Expert clinicians made a greater number of transitions to adjacent body regions (e.g. feet to knees). Novice clinicians made a large number of transitions between body regions that were anatomically distant (Ford 2001).
With experience many gait deviations can be observed. The difficulty of observing one body part at a time is that multiple movements in multiple segments are occurring concurrently. Checklists, such as the one provided in Box 11.1, are usually helpful to work through, especially when learning. Traditionally, the approach is to observe the limb as it moves through the different periods of the stance phase – heel contact, mid-stance and propulsion. Another approach (Pathokinesiology Service 1993) is to divide gait into weight acceptance (initial contact and loading response), single limb support (period when body progresses over single limb), and swing limb advancement (time when one limb is unloaded and the other limb is loaded) and note variations from normal during these phases.
Box 11.1 Practical observational gait analysis
• Observe for amounts and timing of events
• Concentrate on one aspect at a time
• Bisection of calcaneus and posterior aspect of leg is often helpful
• A mark on the medial side of the navicular is also helpful
• Be aware that many individuals may consciously or subconsciously alter gait while being observed
• At least an 8–10 m walkway is desirable and provision for watching clients from behind/in front (frontal plane) as well as from the side (sagittal plane)
• Patient should be wearing shorts (have different sizes available in your clinic)
• Observe with and without shoes, and with and without orthoses
Frontal plane observations
There is no permanent record from observational gait analysis – no opportunity to review the data at a later date. The analysis is very dependent on the skill and experience of the observer. All the data are subjective and qualitative. When one observes an individual standing on both feet, it is impossible to predict whether the load (distribution of force) under both feet is equal. This highlights the fundamental drawback of observation of gait: you cannot observe forces and the eye can be easily deceived. Reliability studies on observational gait analysis show that it is somewhat unreliable (Brunnekreef et al 2005, Krebs et al 1985, Saleh & Murdoch 1985). Despite these limitations, observational gait analysis provides a good overall impression of gait and requires no equipment. Experienced observers use observational gait analysis to make critical judgements, assist in diagnosis and determine the outcomes of interventions such as foot orthoses.
Treadmill
One of the most debated areas of gait analysis is the length of walkway required to achieve ‘normal’ walking patterns: 4–6 m is considered the minimum, but 8–10 m is more appropriate. Some practitioners use treadmills rather than an overground walkway. This is for several reasons: to view running, allow use of video systems or due to a lack of clinical space. If a treadmill is used, one must ensure that the participant has every opportunity to adapt to treadmill walking before the analysis. This usually requires at least 15 minutes of walking on the treadmill. The more exposure to treadmills, the shorter the time recorded to acclimatise and perform consistently (Tollafield 1990). Clearly, older clients, children and clients with medical conditions are likely to tire more quickly. No matter how sophisticated the system is, participants must feel relaxed and comfortable when being observed. Most authorities now accept that in order to achieve this objective, clients should be allowed to walk at their own cadence rather than being artificially constrained by walking in time to a metronome or some other timing device.
For visual observation, treadmills facilitate closer inspection of the gait as well as easy observation of gait in the sagittal plane. In addition, treadmills are relatively inexpensive. There are subtle kinematic and kinetic differences between overground and treadmill gait (Riley et al 2006), however the principal consideration is that people should feel comfortable when using the treadmill.
Video
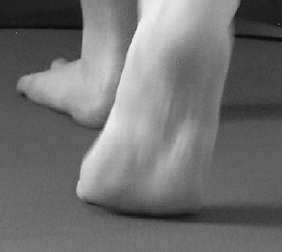
Video recording of gait for subsequent analysis (overground or on a treadmill) offers a different perspective than visual gait analysis. Observational gait analysis is limited by the high speed at which motions occur. It has been observed that events that happen faster than 83 ms (1/12 second) cannot be perceived by the human eye (Gage & Ounpuu 1989), so the use of slow-motion video and freeze-frame can enhance observational gait analysis. For example, some of the motions at the first metatarsophalangeal joint can be observed (Fig. 11.2). With good pause and slow-motion facilities the more subtle features of gait that would otherwise be missed can be observed. This will depend on the frequency of sampling: below 30 Hz may be insufficient, 50 Hz is an ideal for slow walking and 100 Hz will generally be required for running. If these sampling rates are not used, too much movement happens between each sampling frame to be useful for interpretation. Unfortunately, the standard frame rate for consumer-level video cameras is 25 Hz (PAL) and 30 Hz (NTSC). This means that the frame rate for such cameras makes it difficult to see fast-moving parts of the gait cycle: particularly around heel contact and heel and toe off. Some video software systems interpolate video (mathematically create a new video frame between two existing frames) to get around the low frame rate problem, with varying levels of success.
If two cameras and a video mixer are used, it is possible to view gait in two body planes simultaneously on the same split screen eliminating the problem of cross-plane interpretation. Most new digital video cameras allow for video to be downloaded, viewed and archived on a computer. Videos of persons walking with and without footwear and interventions (e.g. taping or foot orthoses) can be easily compared. Some systems (e.g. Dartfish, Contemplas, Silicon Coach) allow the drawing and calculation of angles between segments, the generation of gait analysis reports and the linking of the recorded gait into the patient’s computerised records. Such systems also make it easy to show clients their own gait after it has been recorded, which can be a powerful tool to explain abnormalities in their gait for educational purposes (Fig. 11.3).
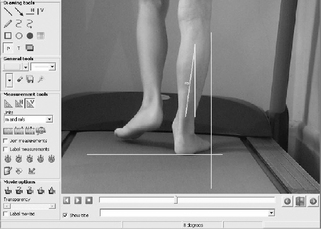
 Screen shot of a typical analysis software for two-dimensional digital video recording of gait.
Screen shot of a typical analysis software for two-dimensional digital video recording of gait.



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


