Metatarsal and Calcaneal Osteotomies for Cavus Foot
Paul G. Peters
Gregory P. Guyton
Pes cavus is defined as an abnormally high arch that fails to correct with weightbearing. The deformity may be initiated through plantarflexion of the first ray with secondary changes in the hindfoot (forefoot cavus), or it may be initiated through an increased calcaneal pitch with secondary changes in the forefoot (hindfoot cavus). Regardless of whether the cavus alignment begins in the hindfoot or forefoot, eventually all components of the deformity become fixed. The relatively inverted position of the calcaneus in a cavus foot prevents the talar head from dropping during the weight-acceptance phase of gait. The resulting rigid foot is less able to pronate and absorb the mechanical loads applied during walking. Plantar pressures are concentrated on the heel and metatarsal heads.
Although many cases are idiopathic in origin, other common etiologies in skeletally mature individuals are Charcot-Marie-Tooth (CMT) disease, poliomyelitis, and trauma (1,2). Deformities identified in the pediatric population may be associated with clubfoot or other neurologic lesions including Friedreich ataxia, hereditary cerebellar ataxias, Roussy-Levy syndrome, spinal muscular atrophy, syringomyelia, diastematomyelia, spinal dysraphism, and cerebral palsy. Each pes cavus foot is different, and surgical procedures are selectively implemented to address the specific deformity present in each case (3, 4 and 5).
INDICATIONS AND CONTRAINDICATIONS
Because of the multiple potential etiologies of the deformity, each cavus foot must be evaluated individually. A careful understanding of the underlying disease process is critical to treatment. The four aspects of the deformity that must be addressed are the hindfoot, forefoot, toe deformities, and the soft tissue component.
In forefoot cavus, plantarflexion of the first metatarsal creates a forefoot valgus, which the hindfoot then compensates by falling passively into varus. In most cases, particularly CMT, this is due to the persistent function of the peroneus longus to plantarflex the first ray, while the anterior tibialis becomes weak (6). Radiographic involvement of the metatarsals is best evaluated on a weightbearing lateral x-ray examining the talo-first metatarsal angle, with normal being 0° and anything greater than 4° being abnormal (7).
The degree of residual mobility of the hindfoot is critical to determining treatment. The Coleman block test can be performed to evaluate the flexibility of the hindfoot. Standing alignment of the hindfoot is evaluated with a wooden block of appropriate thickness placed under the lateral column of the foot. The first ray is then allowed to rest on the floor. If the hindfoot remains flexible, it will correct to a neutral or valgus position (8).
 FIGURE 21.1 Lateral radiograph showing a hindfoot cavus deformity. |
Most cases of forefoot cavus involve at least a partially fixed plantarflexion deformity of the first ray by the time of surgical intervention. A dorsiflexion osteotomy of the first ray is indicated to elevate the medial column and eliminate this underlying cause of the global deformity.
In some relatively rare circumstances, a transfer of the peroneus longus to the peroneus brevis alone will eliminate the overpull of the longus and may be sufficient if the deformity remains very supple. Most cases, however, require an osteotomy either with or without concurrent tendon transfer. A calcaneal osteotomy is required if the hindfoot cannot correct to neutral or beyond with the Coleman block test.
Hindfoot cavus is usually easily identified on a lateral radiograph by an increased calcaneal pitch (Fig. 21.1). The long axis of the calcaneus is assessed relative to the plane of the floor, and an angle of over 30° is indicative of the deformity (7). Isolated hindfoot deformity is rare, especially with the decreased prevalence of polio, and most cases are idiopathic in modern practice.
Calcaneal osteotomies are typically used for correction as long as a reasonable amount of subtalar motion remains (9,10,11). As is also the case in forefoot cavus, extremely rigid deformities may require a triple arthrodesis.
Claw toes are commonly present in cavus deformities (12). Typically, the long flexors and extensors retain function, while the intrinsic musculature of the foot is weakened, resulting in metatarsophalangeal (MTP) joint extension and interphalangeal (IP) joint flexion at the lesser toes. Standard claw toe correction techniques are typically used and are beyond the scope of this chapter.
Clawing of the hallux may represent a special case, however. In some etiologies, particularly CMT and polio, function of the extensor hallucis longus (EHL) may be preserved in the presence of a weak anterior tibialis. This results in the use of the EHL as an accessory dorsiflexor to lift the foot during gait. A severe claw toe results and secondarily depresses the first metatarsal head, which in turn further exacerbates the forefoot cavus. Correction is achieved by fusing the IP joint of the hallux and transferring the EHL tendon directly to the first ray or midfoot, the Jones procedure.
In all circumstances of prolonged cavovarus foot positioning, contracture in the plantar fascia occurs, and the tension must be released to gain appropriate correction and foot alignment. Isolated release of the plantar fascia for deformity correction is not indicated. Sliding calcaneal osteotomies do alter the position of the plantar fascia origin and may be sufficient in some cases, but plantar fascia release as a component of the global deformity correction can be a useful adjunctive procedure.
Contraindications to motion-sparing cavus foot corrections include severe rigid deformities or arthritic change, both of which must be managed with triple arthrodesis. Isolated arthritis along the medial column, particularly in the first tarsometatarsal (TMT), may be addressed with a dorsiflexion-producing fusion of the joint rather than a metaphyseal osteotomy.
In all cases of cavus foot, surgery is strictly contraindicated if there is suspicion of a progressive underlying neurologic lesion. The underlying disease pattern must be understood along with the associated potential for recurrence. Focal neurologic lesions may be signaled by rapidly progressive deformity, marked asymmetry between sides, and long-tract signs.
PREOPERATIVE PLANNING
The location of the pain and impairment should be determined, such as pain from overloading the lateral foot, fifth metatarsal head, fifth metatarsal base, frequent ankle sprains, lateral ankle ligament instability from varus malposition, and claw toes. Detailed physical examination standing and walking should be performed. The etiology of the cavus foot should be determined and if necessary, a neurology consultation and electromyography performed. Sometimes the cause of the cavus foot cannot be determined. Alignment of the hindfoot should be quantitated with a standing tibiocalcaneal angle measurement, as well as range of motion of the hindfoot and ankle, pain with joint motion, presence of callosities, ankle ligament stability, and manual muscle strength testing. Heel cord tightness with the knee flexed and extended should be documented as well as the Coleman block
test. Weightbearing radiographs of the foot and ankle are important to assess alignment, degenerative arthritis, joint instability, bony anomalies, and stress fractures. The level of the cavus deformity should be ascertained. Nonsurgical management involves foot orthoses and braces. Patients need to understand what surgery can accomplish, and that their condition may change over time even after a successful operation. Operative treatment may include correction of muscle imbalance with tendon transfers, soft tissue lengthening, osteotomies of the metatarsals and calcaneus, and arthrodesis.
test. Weightbearing radiographs of the foot and ankle are important to assess alignment, degenerative arthritis, joint instability, bony anomalies, and stress fractures. The level of the cavus deformity should be ascertained. Nonsurgical management involves foot orthoses and braces. Patients need to understand what surgery can accomplish, and that their condition may change over time even after a successful operation. Operative treatment may include correction of muscle imbalance with tendon transfers, soft tissue lengthening, osteotomies of the metatarsals and calcaneus, and arthrodesis.
 FIGURE 21.2 A longitudinal incision, 4 to 6 cm long, is made over the first MTC joint. |
SURGICAL TECHNIQUE
Technique 1: Dorsiflexion Osteotomy of the First Metatarsal
The patient is placed in a supine position. A proximal thigh tourniquet is used. A 4-cm dorsal incision is placed over the first metatarsocuneiform (MTC) joint extending from the distal half of the medial cuneiform to the distal third of the first metatarsal (Fig. 21.2).
The dorsal medial cutaneous nerve to the first toe is and protected if encountered. The EHL tendon is identified and mobilized. It is then retracted medial or lateral with a Weitlander retractor. Localization of the first MTC joint is performed to delineate the osteotomy site, which is 15 mm distal to the joint or at the metaphyseal-diaphyseal flare (Fig. 21.3).
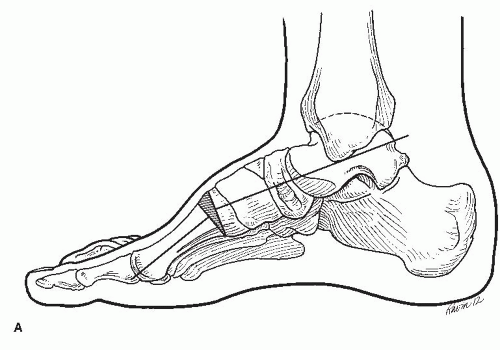
FIGURE 21.3 A: Placement of osteotomy in a cavus foot.
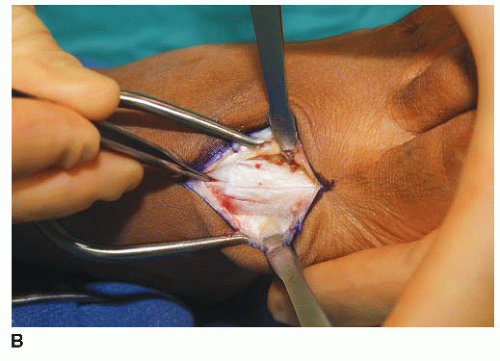
FIGURE 21.3 (Continued) B: The incision is deepened, and the medial dorsal cutaneous nerve is identified and protected. The extensor tendon is retracted laterally. The MTC joint is at the proximal extent of the incision.
The first cut is made with a microsagittal saw parallel to the TMT joint, hinging on the intact plantar cortex in greenstick fashion. A small K-wire can be used to template the osteotomy using a C-arm to provide localization and to ensure a parallel placement (Fig. 21.4A and B).
A second, converging cut is then made, aiming at the anticipated apex of the osteotomy (Fig. 21.4C).Related posts:
 Hallux Metatarsophalangeal Interposition Arthroplasty (Modified Keller Procedure)
Hallux Metatarsophalangeal Interposition Arthroplasty (Modified Keller Procedure)
 Realignment of Lesser Toe Deformities
Realignment of Lesser Toe Deformities
 Tarsometatarsal Arthrodesis
Tarsometatarsal Arthrodesis
 Peroneal Tendon Repair and Reconstruction
Peroneal Tendon Repair and Reconstruction
 Tibiofibular Syndesmosis Reduction and Fixation
Tibiofibular Syndesmosis Reduction and Fixation
 Autologous Osteochondral Transfer for Talar Defects: Mosaicplasty
Autologous Osteochondral Transfer for Talar Defects: Mosaicplasty

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


