Meniscal Repair with Meniscal Fixators
Peter R. Kurzweil
The fixation of meniscal tears has undergone a revolution since the introduction of fixators into arthroscopic surgery a decade ago. The simplicity and ease of insertion of these devices led to their popularity for the repair of torn menisci. The only alternative was the traditional suture technique, which required additional incisions, prolonged operative time, and the risk of neurovascular injury.
The first fixators on the market were somewhat rigid devices made of a variety of bioabsorbable materials, with varying resorption times. They are supplied in varying lengths, with the appropriate size chosen depending on the location of the tear. They were designed with barbs, heads, or screw threads to engage meniscal tissue, and therefore are not well suited for the most peripheral tears or capsular detachments. Compression at the tear site is often difficult to achieve and nearly impossible to adjust after insertion. Among the most popular first-generation fixators are the Arrow, the Hornet, the Clearfix Screw, and the Dart.
With increasing reports of unsatisfactory long-term results and the inability to repair peripheral tears to the capsule, a second generation of meniscal fixators was developed to more closely mimic suture repairs. The two suture-based implants currently available are the Fast-Fix (Smith & Nephew, Endoscopy Division, Andover, MA) and the RAPIDLOC (Mitek Surgical Products, Westwood, MA) (Fig. 9-1 A,B). Both of these implants consist of two small polymer T-bar anchors connected by a pre-tied, locking, sliding knot, which has eliminated the need for arthroscopic knot tying. Both Fast-Fix anchors and one of the RAPIDLOC anchors are designed to be deployed across the capsule, then rotate to engage the capsule when the connecting suture is pulled, analogous to EndoButton (Smith & Nephew, Andover, MA) fixation. Since the suture length between the two anchors adjusts during implantation to allow compression of the tear, these fixators come in only one size. The only variability is the angle of the needle delivery system. But, like other fixators, the anchors deployed across the capsule cannot be removed arthroscopically once inserted.
The Fast-Fix Delivery Needle is supplied with three angles: 0, +22, and −22 degrees (Fig. 9-1D). The −22-degree needle allows suture placement on the undersurface of the meniscus. The device requires that each anchor be deployed across the capsule, and at least one also pass through the tear. This allows for a vertical or horizontal suture orientation. The Rapid-Loc comes with needle tips of 0, 12, and 27 degrees (Fig. 9-1C). It is designed to be placed on the superior surface of the meniscus. Its insertion requires only one pass of the “backstop” anchor across the tear and through the capsule. Both fixators come with anchors and sutures that are permanent or bioabsorbable. The choice depends on surgeon preference. I prefer permanent material, as is my choice when doing the traditional inside-out or outside-in suture repair techniques.
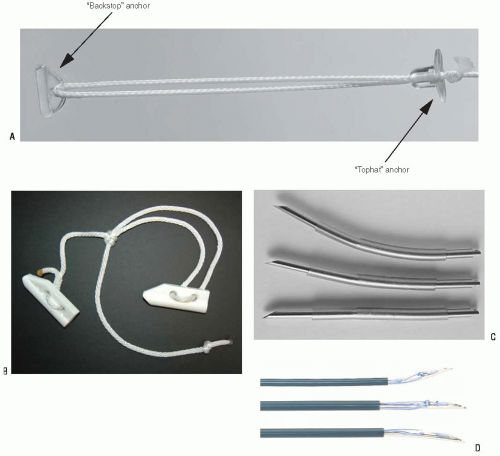 FIGURE 9-1 A: The Rapid-Loc is made of two anchors called the “top-hat” and “backstop,” which are connected by a pre-tied, sliding suture of No. 2 nonabsorbable Ethibond (Ethicon, Somerville, NJ). Note that it is also available with absorbable components using a PDS “top-hat” and Panacryl suture. B: The Fast-Fix is made of two 5-mm anchors also connected by a pre-tied, sliding No. 0 suture of nonabsorbable, braided polyester. C: The angles for the insertion needles for the Rapid-Loc are 0, 12, and 27 degrees. D: The Fast-Fix is supplied with three insertion angles of 0, +22, and −22 degrees. |
INDICATIONS/CONTRAINDICATIONS
The indication for meniscal repair should remain the same regardless of technique. Fixators are not ideal to use for every tear location and orientation. My preference is to use outside-in suture repairs for anterior third tears, and once started, I will often stretch this to the anterior two thirds of the meniscus. Fixators are most ideal for the posterior third, where the traditional inside-out technique would have required a posterior incision to protect neurovascular structures. For tears entirely in the posterior half of the meniscus, I will generally use suture-based fixators only. However, there is no reason to commit to just one method of fixation. I frequently use hybrid fixation, with outside-in sutures anteriorly and fixators posteriorly. Cost is an issue, and these second-generation fixators are far more expensive than using sutures.
In my experience, unstable bucket-handle tears, which are found displaced in the notch, have sometimes failed when fixators alone were used. Although these failures were seen with first-generation fixators, this led me to favor the traditional suture repair techniques for this scenario. Recently, I have been more confident with hybrid repairs using suture-based fixators and outside-in sutures for these displaced bucket-handle tears.
Tear orientation is also important. Ideally, fixators (and sutures) should be inserted into the meniscus so that they are perpendicular to the tear, making vertically oriented tears ideal. Horizontal cleavage tears and radial tears are less suited for fixators, and sutures are preferred if a repair is indicated. Some surgeons are attempting to use the Fast-Fix in these situations.
SURGERY
Patient Positioning
We prefer to have the patient supine on the operating room table, allowing the knees to rest in extension. A tourniquet is applied to the proximal thigh but is not routinely inflated. A lateral thigh post clamped to the table allows application of a valgus stress to the knee, opening the medial compartment for visualization. For viewing the lateral compartment, the leg is placed in the figure-4 position. We have also found that general anesthesia affords a little extra room in the compartments, since valgus or varus stressing to open the knee is sometimes too painful with only local anesthesia.
Meniscal Preparation
Related posts:
 Medial Patellofemoral Ligament Reconstruction and Repair
Patellectomy
Medial and Lateral Meniscus Transplantation: Arthroscopic-Assisted Techniques and Clinical Outcomes
Double-Bundle Posterior Cruciate Ligament Reconstruction
Arthroscopic Chondroplasty and/or Debridement
Synovectomy for Pigmented Villonodular Synovitis
Medial Patellofemoral Ligament Reconstruction and Repair
Patellectomy
Medial and Lateral Meniscus Transplantation: Arthroscopic-Assisted Techniques and Clinical Outcomes
Double-Bundle Posterior Cruciate Ligament Reconstruction
Arthroscopic Chondroplasty and/or Debridement
Synovectomy for Pigmented Villonodular Synovitis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


