Medial Epicondyle Fractures and Elbow Dislocations
CASE PRESENTATION
An 11-year-old right hand dominant gymnast presents with left elbow pain, swelling, and limited range of motion after a vaulting injury. There is no history of prior elbow injury or pain, and she denies any distal numbness, tingling, or weakness. Examination reveals swelling over the medial elbow and limited short arc of elbow flexion-extension without crepitus. The hand is well perfused, and distal median, ulnar, and radial nerve function are intact. Radiographs are shown in Figure 29-1.
CLINICAL QUESTIONS
How common are medial epicondyle fractures?
What are the associated injuries seen with medial epicondyle fractures?
What are the surgical indications for the treatment of medial epicondyle fractures?
What are the anticipated results of nonoperative and surgical care for medial epicondylar fractures?
What are the potential complications of medial epicondylar fractures and strategies for their avoidance?
What are the most common patterns of elbow dislocations in children and adolescents?
What are the associated injuries seen with “simple” elbow dislocations?
What are the anticipated results and potential complications of elbow dislocations?
THE FUNDAMENTALS
Medial epicondyle avulsion fractures are common in older children and adolescents, typically arising from sports and high-energy mechanisms of injury. Associated injuries are common, and surgical indications continue to evolve, as our understanding of these injuries—and their potential long-term sequelae—improves.
Elbow dislocations similarly occur in pediatric patients after high-energy injuries and are often associated with obvious or occult osteochondral injuries about the elbow. Timely recognition of associated injuries and adherence to surgical treatment principles are essential to optimize clinical results and avoid complications.
Etiology and Epidemiology
Medial epicondyle fractures are technically avulsion injuries of the medial epicondylar apophysis. While the medial epicondylar apophysis is extra-articular and contributes little to the longitudinal growth of the humerus, it does serve as the origin of the flexor-pronator mass. Avulsion fractures, therefore, typically result from high-energy forces imparted on the flexor-pronator muscles with the elbow under valgus stress. These injuries may occur as a result of sudden, vigorous traumatic events, or from less forceful mechanisms in the patient with underlying apophysitis due to repetitive overuse.
Medial epicondylar avulsion injuries represent the third most common injury pattern in the skeletally immature patient, comprising approximately 10% to 15% of all elbow fractures.1, 2 and 3 Peak incidence occurs in patients between 10 and 12 years of age, slightly older than seen with supracondylar or lateral condylar fractures of the distal humerus.1,4, 5, 6, 7 and 8 Due to the associated high-energy mechanisms of injury, medial epicondylar apophyseal fractures are seen with concomitant elbow dislocations in up to half of cases, and associated elbow fractures (particularly radial neck and head fractures) are also common.1,8
Elbow dislocations are relatively uncommon in skeletally immature patients (Figure 29-2). Again, mechanisms of injury include high-energy falls or sports-related events, explaining in part the predilection for adolescent patients.9,10 Elbow dislocations most commonly occur with extension-valgus stress and result in tears to the ulnar collateral ligament complex, anterior capsule, brachialis muscle, and potentially fractures of the medial epicondyle, coronoid, and/or radial head or neck. Participation in competitive and extreme sports at younger and younger ages is changing the incidence of elbow dislocations and the severity of associated injuries about the elbow.
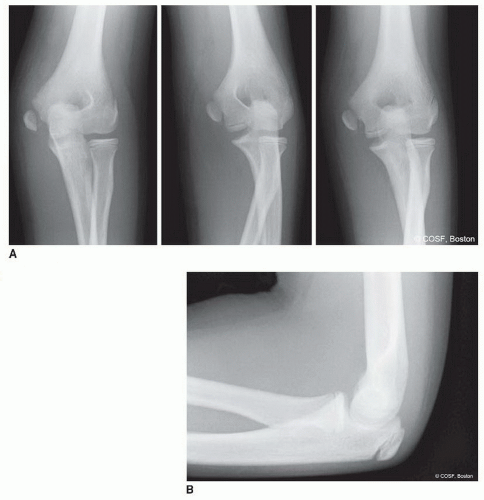 FIGURE 29-1 A, B: AP, oblique radiographs and lateral radiographs of a displaced medial epicondyle fracture. |
Clinical Evaluation
Many of life’s failures are people who did not realize how close to success they were when they gave up.
—Thomas Edison
Patients will typically present with medial elbow pain, swelling, and varying degrees of limited elbow motion after acute fractures. History should be taken regarding hand dominance, functional demands including sports participation, prodromal symptoms consistent with overuse apophysitis, and chronicity of symptoms if present. Physical examination will usually elicit tenderness over the (displaced) medial epicondylar fracture fragment, with or without associated swelling, ecchymosis, and limited elbow flexion-extension. A thorough neurovascular examination is critical to rule out evidence of peripheral neuropathy, particularly involving the ulnar nerve.
In patients with acute elbow dislocations, the clinical presentation is less subtle. Patients will present acutely with pain, obvious deformity, and fixed elbow position after a fall or high-energy injury. Neurovascular examination is important to identify primary nerve palsies due to the injury and establish a baseline against which post-treatment examinations may be compared. Careful assessment of median and ulnar nerve function is critical. Vascular insufficiency is quite uncommon.
Radiographic evaluation will confirm the diagnosis. Standard anteroposterior (AP) and lateral radiographs will identify the medial epicondylar avulsion fracture and characterize displacement. Oblique radiographs, including the external rotation oblique, will assist in radiographic assessment of fracture displacement as it brings the normally posteromedial medial epicondyle into profile. It is important to recognize that the flexor-pronator mass acts to displace the medial epicondylar apophysis distally and often anteriorly, not laterally, and therefore the magnitude of fracture displacement cannot be quantified on AP radiographs. Indeed, recent information suggests that plain radiographs do not allow for accurate measurement of displacement, and that intra- and interobserver reliability of medial epicondylar fracture displacement is low.11,12
 FIGURE 29-2 AP and lateral radiographs of a posterolateral elbow dislocation in a 9-year-old female gymnast. |
Medial epicondylar fracture fragments can be entrapped in the elbow joint. The trochlear ossification is usually irregular, often fragmented. The medial epicondyle is ovoid and regular. At times, the entrapped medial epicondyle can be mistaken for a trochlea and the diagnosis of an entrapped medial epicondyle missed. Look for the medial epicondyle in or near its anatomic posteromedial location. If it is not there, look for it in the joint. If necessary, compare elbow films of the affected and unaffected side. An entrapped medial epicondyle is a diagnosis not to be missed.
In cases of displaced medial epicondylar apophyseal fractures, joint stability may be assessed using gravity valgus stress views (Figure 29-3). This radiographic technique involves placing the patient in the supine position with the shoulder abducted 90 degrees, elbow extended, and the forearm maximally supinated (the thumb points to the ground). An AP view of the elbow is taken, and the medial joint space is assessed. Medial joint widening of >3 mm is suggestive of valgus instability.
Plain radiographs, including obliques, will also clearly diagnose simple and complex elbow dislocations and characterize the direction of displacement. Elbow dislocations in general are described anatomically according to the position of the forearm in relationship with the distal humerus (e.g., posterolateral, posteromedial, anterior, medial, lateral). “Simple” dislocations denote pure joint dislocations, whereas “complex” dislocations are used to describe joint instability with associated bony or chondral fractures.
Advanced three-dimensional imaging is rarely required in acute cases of medial epicondylar fractures but may provide important additional information in cases of chronic injuries or elbow dislocations with suspected chondral or osteochondral shear fractures (Figure 29-4). Imaging with magnetic resonance imaging (MRI) is particularly useful in these latter situations, especially when nonoperative management is being considered.
Surgical Indications
There are only two options regarding commitment. You’re either in or out. There’s no such thing as a life in-between.
—Pat Riley
The indications for surgical treatment of medial epicondylar avulsion fractures are controversial and continue to evolve. Historically, almost all displaced fractures of the medial epicondyle were treated nonoperatively with reportedly acceptable results. Farsetti et al.13 previously reported on 42 children and adolescents with displaced medial epicondyle fractures followed to an average age of 45 years. Patients treated nonoperatively had similarly good long-term results as those treated with open reduction internal fixation (ORIF). Based upon this information, the authors and others suggest that displaced medial epicondylar fractures may be successfully treated nonoperatively.14 This and other similar reports have established the dogma by some that medial epicondylar avulsion fractures are nonsurgical injuries.
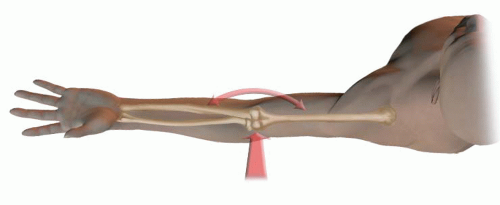 FIGURE 29-3 Schematic representation of the valgus gravity stress radiograph. With the patient supine, the shoulder abducted 90 degrees, elbow extended, and the forearm maximally supinated (the thumb points to the ground). An AP view of the elbow is taken by directing the beam parallel to the ground, and the medial joint space is assessed. |
 FIGURE 29-4 Complex elbow dislocation with chondral shear fracture. A: AP and lateral radiographs demonstrate a mildly angulated radial neck fracture and subluxation and incongruity of the ulnohumeral joint. B: Sagittal MRI images depicting an intra-articular loose body (small arrow) from a chondral shear injury to the trochlea (arrowhead) with a dislocated ulnohumeral articulation. |
It is clear that patients with medial epicondyle fracture dislocations in whom the fracture fragment is incarcerated within the elbow joint should be treated with expeditious ORIF. Relative indications include displaced fractures with associated ulnar neuritis/neuropathy or fractures affecting the dominant limb in throwing or overhead athletes. We tend to be surgically aggressive for displaced medial epicondyle fractures, given the safety and efficacy of acute surgical treatment and the functional limitations and surgical challenges of symptomatic nonunions or malunions.15, 16 and 17 We prefer anatomic alignment of the fracture, rigid fixation with elbow joint stability restored, and early motion rehabilitation to avoid a flexion contracture.
Occasionally patients will present for first consultation to the pediatric hand and upper extremity surgeon after closed reduction of an elbow fracture dislocation by a referring caregiver. The previous care can cloud the decision-making process. If the elbow joint is unstable and/or the fracture is still displaced, we tend to proceed with ORIF to provide stability for early range of motion and avoid late complications. Clearly chronically entrapped medial epicondylar fracture fragments require extraction and ORIF no matter how late those patients present for evaluation and care.
In cases of elbow dislocations, it is clear that acute simple elbow dislocations should be treated with prompt closed reduction, either under conscious sedation or under general anesthesia. Surgical indications include complex elbow dislocations with associated nerve injury or entrapment, associated osteochondral fractures, or joint instability precluding appropriate postinjury rehabilitation. Surgical repair of the collateral ligaments and/or muscles is not necessary following successful closed reductions of simple dislocations.18, 19 and 20
SURGICAL PROCEDURES
• Closed Treatment of Medial Epicondyle Fractures and Elbow Dislocations
As cited above, nonoperative treatment is appropriate for nondisplaced or minimally displaced medial epicondylar fractures without ulnar neuropathy in patients without high functional demands of the affected elbow (e.g., baseball pitchers, gymnasts, cheerleaders) (Figure 29-5). Nonoperative care consists of a brief period of splint or cast immobilization (no longer than 2 weeks), followed by hinged elbow brace protection and advancement of elbow range of motion in brace until 6 weeks postinjury. Physical therapy may be initiated at 6 weeks, if needed, to regain the remaining elbow motion and strength. Sports participation is limited until elbow motion and strength normalizes, usually at 2 to 3 months.
One error in nonoperative treatment of medial epicondylar fractures lies in excessive immobilization. The amount of soft tissue and capsular injury cannot be accurately assessed on initial clinical evaluation or radiographs. Stiffness is a risk, even with seemingly innocuous fractures. If nonoperative treatment is chosen—and therefore no intent to achieve anatomic fracture reduction—early protected range-of-motion exercises are critical to avoid functionally limiting stiffness.
The other problem with nonoperative treatment of displaced fractures is symptomatic nonunions or malunions. If the medial epicondylar fragment heals in a displaced distal and anterior position, it will limit motion (especially extension) and function. Some nonunions cause symptomatic valgus instability, especially in gymnasts and throwing athletes.
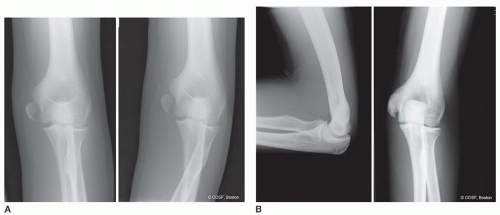 FIGURE 29-5 Nonoperative treatment of a displaced medial epicondyle fracture involving the nondominant limb of a 14-year-old male. A: Initial AP and lateral radiographs demonstrate a displaced medial epicondyle apophyseal avulsion. B: Follow-up radiographs 3 months postinjury demonstrate evidence of bony union with exostosis. At times this can lead to ulnar nerve compression. |
Closed reduction of simple elbow dislocations follows principles similar to adults. Conscious sedation or general anesthesia is preferred to mitigate the effects of muscle spasm, avoid excessive force, which imparts risk of producing iatrogenic osteochondral shear fractures, and provide maximum patient comfort. In general, for the most common posterior dislocations, closed reduction maneuvers may be divided into “pull” or “push” techniques.21, 22, 23, 24, 25, 26, 27, 28 and 29 With the brachium stabilized and the patient either in the supine or in the prone position, the elbow is flexed and forearm supinated to unlock the radial head and reduce tension on the biceps. Longitudinal traction is then provided distally along the axis of the humerus, with simultaneous anteriorly directed force. Hyperextension is avoided, as it further tensions the anterior capsule and flexor muscles and may lead to iatrogenic shear fractures of the radial head, coronoid process, trochlea, or capitellum. Reduction with extension also increases the risk of entrapment of the median nerve in the joint. Alternatively, distally directed pressure may be applied to the prominent olecranon process and radial head with the elbow flexed and forearm supinated to “push” the forearm back into position. Following reduction, careful radiographic evaluation is performed to confirm a congruent joint reduction and rule out associated fractures, which may not be apparent on initial injury films. The stable arc of motion is assessed and the limb immobilized in a long-arm bivalved cast or posterior splint with the forearm in pronation. The postreduction immobilization needs to be quite bulky
as elbow dislocations will have considerable soft tissue swelling in the first week postinjury.
as elbow dislocations will have considerable soft tissue swelling in the first week postinjury.
▪ ORIF of Medial Epicondylar Fractures
An ORIF of displaced medial epicondylar apophyseal fracture fragments is performed under general anesthesia and tourniquet control (Figure 29-6). In cases of fracture dislocations with the fracture fragment incarcerated in the elbow joint, initial attempts at closed manipulation may be performed under general anesthesia before proceeding to open repair.30,




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
