Chapter 15 Lower Limb Orthotic Devices
An orthosis is defined as a device attached or applied to the external surface of the body to improve function, restrict or enforce motion, or support a body segment.38 Lower limb orthoses are indicated to assist gait, reduce pain, decrease weight-bearing, control movement, and minimize progression of a deformity. Lower limb orthoses assist nonambulatory patients with transfer and mobility skills and assist ambulatory patients in becoming safe walkers. Ambulation aids can be used in combination with lower limb orthoses to help patients ambulate more safely. Ambulation aids represent extensions of the upper limb but are discussed in this chapter because of their importance in gait.
Principles of Lower Limb Orthoses
Orthoses should be used for the specific management of selected disorders. As in all fields of medicine, specific treatment should be based on a specific medical diagnosis, with an established goal of treatment.56 Placement of orthotic joints should approximate anatomic joints. Box 15-1 outlines this principle as well as other common lower limb orthotic principles. Most orthoses use a three-point system to ensure proper positioning of the limb within the orthosis.27 For example, a knee that has a tendency to hyperextend, or “back knee,” can be treated with a knee orthosis that applies force posterior to the knee but also applies forces anteriorly along the leg and the thigh. Such an orthosis ensures adequate control of the knee by exerting these forces proximal to, distal to, and at the knee joint.
Shoes
The purpose of wearing shoes is to protect the feet. The normal foot does not require support from shoes. The sole should be pliable so as not to interfere with the normal biomechanics of the foot. A practical way of ensuring that a shoe is of adequate length is to determine whether the index finger can be placed between the tip of the great toe and the toe box.58 The presence of calluses indicates areas of friction from poorly fitting (loose) shoes. The presence of corns indicates areas of friction over bony prominences, most often caused by tight-fitting shoes. Leather shoes are good choices for all types of activity. They are durable, allow ventilation, and mold to the feet with time. A good pair of shoes can often eliminate the need for foot orthoses and should be considered before orthotic prescription.
Shoe Parts
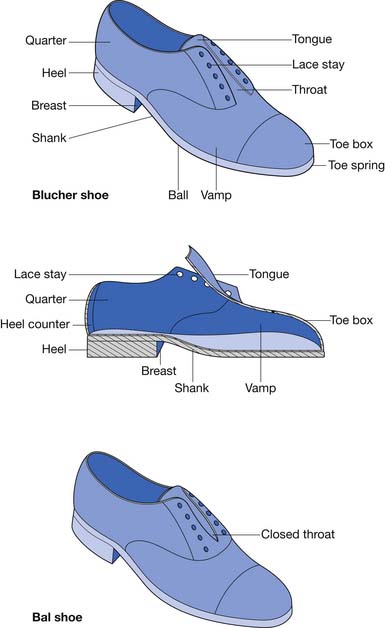
Two types of dress shoes are commonly worn: the Blucher and the Bal (Figure 15-1). The tongue is part of the vamp in the Blucher shoe. The quarters overlap the vamp. A Blucher shoe is recommended for patients requiring an orthosis because there is more room to don and doff the shoe and the orthosis because of the open throat.63 In the Bal shoe style the quarters meet at the throat. The vamp is stitched over the quarters at the throat, thereby limiting the ability of the shoe to open and accommodate an orthosis.
Foot Orthoses
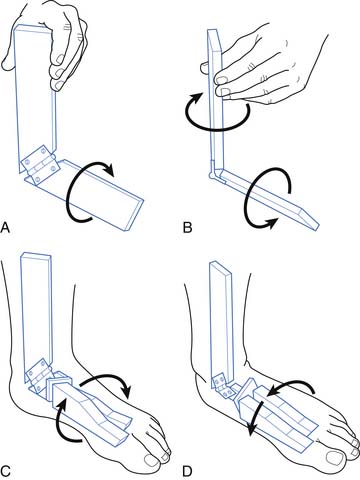
Foot orthoses range from arch supports found at a local pharmacy or athletic store to customized orthoses fabricated by an orthotist. The effectiveness of an orthosis depends on proper diagnosis of the foot condition, the appropriate selection of orthotic material, and proper molding. Foot orthoses affect the ground reactive forces acting on the joints of the lower limb. They also have an effect on rotational components of gait (Figure 15-2).
Mild conditions can be treated with over-the-counter orthoses. More severe problems and chronic medical conditions require customized orthoses.61 These are available in three types. A soft type is most commonly used in over-the-counter orthoses. Orthotists usually provide semirigid orthoses, which provide more support than the soft type but are still shock absorbing. A rigid orthosis is indicated only for a problem that requires aggressive bracing to control a deformity.
To make a custom foot orthosis, the subtalar joint should be placed in a neutral position before casting. This position minimizes abnormalities related to foot and ankle rotation, such as hyperpronation, and it is also the position in which the foot functions best.41 The subtalar neutral position is used to treat conditions associated with hyperpronation including pes planus, patellofemoral pain.9,48 The foot is then covered with a parting agent such as stockinette or a clear plastic wrap. The foot is then wrapped in either plaster of Paris strips or fiberglass tape and allowed to harden. Fiberglass casting is also used for difficult orthotic cases where the fiberglass casting itself can be used as a temporary orthosis to determine whether the mold properly controls the deformity. This negative mold is then removed to allow a positive mold to be made from the negative mold. The positive mold can be modified to increase the effectiveness of the orthosis. The custom orthosis is obtained by heating and form-fitting (often by use of a vacuum) the plastic to the positive mold.
Common Foot Conditions
Pes Planus (Flat Foot)
Symptomatic relief of pain is obtained by controlling excess pronation of the foot. Pronation of the foot can be defined as a rotation of the foot in the longitudinal axis resulting in a lowering of the medial aspect of the foot. Foot pronation is a component of eversion. Eversion involves pronation at the subtalar joint, dorsiflexion at the ankle joint, and abduction of the forefoot at the tarsometatarsal joints. The key to controlling excess pronation is controlling the calcaneus to keep the subtalar joint in a neutral position.
Pes planus can be due to abnormalities such as excessive internal torsion of the tibia (which results in pronation of the foot) or malalignment of the calcaneus. It is the interaction between the tibia and the foot at the subtalar joint that allows pathology outside the foot to cause inrolling of the foot (see Figure 15-2).
The reduction of pronation is accomplished by maintaining the calcaneus and the subtalar joint in correct alignment. The subtalar joint should be in a neutral position during the custom molding process. The subtalar joint neutral position prevents rotational deformities associated with excessive pronation or supination from occurring (see Figure 15-2, C and D). Elevation of the anteromedial calcaneus exerts an upward thrust against the sustentaculum tali to help prevent inrolling.6 The orthosis should extend beyond the metatarsal heads to provide better leverage for control of the deformity. A custom-made foot orthosis designed to prevent hyperpronation is also referred to as a UCBL orthosis (or UCB), denoting the University of California Biomechanics Laboratory, where original work regarding this type of orthosis was performed in the 1940s. There are two common mistakes noted in custom foot orthoses. First, some are not made by orthotists, who represent the profession best capable of making a proper foot orthosis. Second, some custom foot orthoses do not cup the calcaneus but rather merely serve as a platform to stand on. The orthosis must extend proximally enough on the calcaneus to cup and control the subtalar joint during gait.
Some cases of pes planus are due to ligamentous laxity within the foot. For these cases a medial longitudinal arch support can be helpful for alleviating pain. Initial use of an arch that is too high can cause discomfort. The height of the arch can be increased as necessary as the foot develops a tolerance for the inlay. A Thomas heel extension (term for increased medial length to heel) can also offer medial support, particularly for heavier individuals. A most practical piece of advice for runners who have hyperpronation or pes planus is to purchase a pair of running shoes with a firm medial heel counter as well as shoes with a wide last at the shank (see Figure 15-1). Each of these applications helps prevent pronation at the subtalar joint.
Pes Cavus (High-Arched Foot)
A typical complication of pes cavus is excess pressure along the heel and metatarsal head areas, which can lead to pain. This can be prevented by making the height of the longitudinal support just high enough to fill in the space between the shank of the shoe and the arch of the foot to distribute weight more effectively. Weight should also be evenly distributed over the metatarsal heads. The lift is extended just to the metatarsal head area to help distribute and alleviate pressure over the metatarsal weight-bearing area. The high point of the arch is located at the talonavicular joint because there is no tendency to pronate as in pes planus. If the tibia is externally rotated (see Figure 15-2), this can give the appearance of an elevated arch as the foot supinates and the lateral aspect of the foot assumes additional weight-bearing responsibility. In these cases a foot orthosis is custom molded with the subtalar joint in a neutral position to prevent excess supination from occurring.
Forefoot Pain (Metatarsalgia)
Relief of pain in the forefoot is accomplished by distributing the weight-bearing forces to an area proximal to the metatarsal heads. This can be done by either internal or external modification. A metatarsal pad (also referred to as a “cookie”) can be placed inside the shoe just proximal to the second, third, and fourth metatarsal heads. It should also be just proximal to the lateral aspect of the first metatarsal head and medial to the fifth metatarsal head (Figure 15-3). A metatarsal bar is recommended for cases in which the foot is too sensitive to tolerate a pad inside the shoe. The metatarsal bar is typically ¼-inch thick and tapers distally. The distal edge should be proximal to the metatarsal heads. It is often applied to a leather or neoprene sole.35 The metatarsal bar can also be used for forefoot pain associated with pes cavus. A rocker bottom (Figure 15-4) can also be used for metatarsalgia to decrease the force on the metatarsal pad region at push off.


Prevention of forefoot pain should also be emphasized to patients. Patients should avoid shoes with high heels or pointed toes, which place excess stress on the metatarsal heads.4
Heel Pain
The painful area can be alleviated by using an orthosis to help distribute weight. Rubber heel pads can be applied inside the shoe to offer relief in cases of minor discomfort. A calcaneal bar is recommended for cases in which the foot is too sensitive to tolerate a pad inside the shoe and the heel pain is associated with a chronic condition. The calcaneal bar is placed distal to the painful area to prevent the calcaneus from assuming full weight-bearing status. The same can be accomplished with a shoe that has a spring for the heel set on the anterior calcaneus (see Figure 15-4, A). The application of a rocker bottom shoe can also be used to help initiate heel strike anterior and the ground reaction force anterior to the painful calcaneus (see Figure 15-4, B). Both of these shoe types are now commercially available.
A common cause of heel pain along the anteromedial calcaneus is plantar fasciitis. Pain occurs at the attachment site of the fascia along the medial aspect of the heel.39 Point tenderness is located over the anteromedial calcaneus. It is common in people who hyperpronate their feet, thereby placing excess stress on the medial longitudinal arch. A custom-made orthosis with the subtalar joint in a neutral position (such as that described for pes planus) helps prevent excessive inrolling from occurring and reduces the stress placed along the proximal arch. A custom-made UCB orthosis is indicated for cases in which conservative treatment has failed. From an orthotic standpoint, conservative treatment should include the use of a pair of shoes with a firm medial heel counter and a wide shank (see Figure 15-1).
An additional orthotic intervention for plantar fasciitis is the application of a plantar fascia night splint, which is a prefabricated AFO placed in a few degrees of dorsiflexion.16,42 This helps provide the plantar fascia and plantar flexors a therapeutic stretch during sleep hours, assuring the patient several hours of passive stretching daily. Such a device is recommended for as long as is necessary until the patient is asymptomatic (Figure 15-5).

Heel spurs are frequently mistaken as the source of heel pain. Heel spurs related to plantar fasciitis are the result of mechanical stress acting through the plantar fascia onto its origin at the calcaneus and are not the source of the pain.34 Inferior heel spurs are related to advancing age and are not painful in nature.
Osteoarthritis of the Knee
Although osteoarthritis of the knee is not a foot condition, it is mentioned here because pain related to it can be alleviated with foot orthoses. Foot orthoses alter the ground reaction forces affecting the more proximal joints, such as the knee, and this relationship should be considered when prescribing a foot orthosis. Lateral heel wedges can be used for conservative treatment of osteoarthritis when medial compartment narrowing is present. The heel wedges used are ¼-inch thick along the lateral border and taper medially. Relief was obtained with heel wedges in 74 of 121 knees from 85 patients in one study.15 Relief of pain was most frequently obtained in patients with mild osteoarthritis, but it was also documented in some patients with complete obliteration of the medial joint space. Wedge use widened the gait pattern. This orthosis has not been studied in patients with medial meniscus injuries, but it might afford some pain relief with medial compartment unloading.
Pediatric Shoes
It is a common misconception that all flat feet need to be treated in children. Flat feet are usual in infants, common in children, and occur occasionally in adults.50 Flat feet improve over time, in part because of the loss of subcutaneous fat and the reduction of laxity of the joints that occur with growth50 and the maturation of the gait pattern. Intensive treatment with corrective shoes or inserts for a 3-year period did not alter the natural history of flat feet in 129 children who were 1 to 6 years of age.58 One cannot make the asymptomatic person feel any better. Frequent shoe size change is necessary in the first few years of life.59
Ankle-Foot Orthoses
AFOs are the most commonly prescribed lower limb orthoses. They were formerly known decades ago as short leg braces. Metal or plastic AFOs can be used effectively to control ankle motion. Metal AFOs are relatively contraindicated in children because the weight of the brace can cause external tibial rotation. Plastic AFOs are now most common in all age-groups.
AFOs should provide mediolateral stability as a safety feature.17 Although much emphasis with AFOs is placed on controlling the amount of dorsiflexion and plantar flexion, movements at the subtalar joint also significantly influence the biomechanics of gait. Inversion includes supination at the subtalar joint, adduction at the tarsometatarsal joints, and plantar flexion at the ankle joint, which results in the foot being in an equinovarus position. Eversion includes pronation at the subtalar joint, abduction of the forefoot at the tarsometatarsal joints, and dorsiflexion at the ankle joint, resulting in the foot being in a valgus position. Rotation at the subtalar joint is also accompanied by rotation of the tibia (see Figure 15-2).
AFOs can also stabilize the knee during gait.23 They are prescribed for conditions affecting knee stability, such as genu recurvatum. An AFO should be considered for conditions affecting the knee, particularly when a concurrent problem exists at the ankle or subtalar joints. A proper AFO prescription considers the biomechanical influence of the orthosis at the foot, ankle, and knee in all planes of movement. It is very important to remember that plantar flexion creates a knee extension moment and dorsiflexion creates a knee flexion moment.
Metal Ankle-Foot Orthoses
Recent research has offered support that metal AFOs provide better stabilization of the ankle during the gait cycle.8
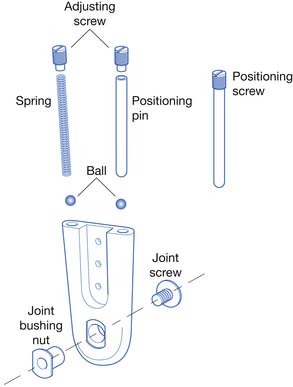
The metal AFO consists of a proximal calf band, two uprights, ankle joints, and an attachment to the shoe to anchor the AFO (Figure 15-6). The posterior metal portion of the calf band should be 1.5 to 3 inches wide to adequately distribute pressure.11 The calf band should be 1 inch below the fibular neck to prevent a compressive common peroneal nerve palsy. A leather strap with Velcro is used to close the calf band, because it provides ease of closure for patients with only one functional upper limb.

Ankle joint motion is controlled by pins or springs inserted into channels (Figures 15-7 through 15-10). The pins are adjusted with a screwdriver to set the desired amount of plantar flexion and dorsiflexion. The spring is also adjusted with a screwdriver to provide the proper amount of tension necessary to aid motion at the ankle joint (used to assist dorsiflexion). Longer channels help prevent the spring mechanism from ″bottoming out” and provide for more precise control of ankle motion.


FIGURE 15-8 Double-action stirrup (left) and dorsiflexion assist stirrup (right), used with the ankle joints shown in Figures 15-7 and 15-6, respectively.
(Courtesy USMC, Pasadena, CA.)

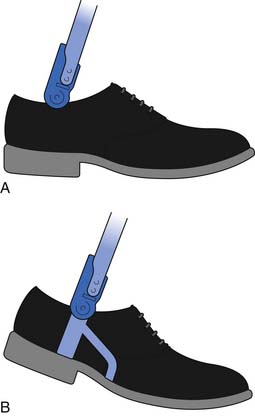
A solid stirrup is a U-shaped metal piece permanently attached to the shoe. Its two ends are bent upward to articulate with the medial and lateral ankle joints (see Figure 15-7). The proximal stirrup attachment sites are shaped to enforce the desired movements at the ankle joint (see Figure 15-8). The sole plate can be extended beyond the metatarsal head area for conditions requiring a longer lever arm for better control of plantar flexion (e.g., plantar spasticity).
A split stirrup can be used instead of a solid stirrup (see Figures 15-6 and 15-9). The split stirrup has a sole plate with two flat channels for insertion of the uprights. The two uprights are now called calipers, as they can open and close distally to allow donning and doffing of the AFO. A split stirrup allows removal of the uprights from the shoes so that the AFO can be worn with other shoes (see Figure 15-6). Other pairs of shoes should also have the sole plate with channels for calipers incorporated into the heel area. The split stirrup is not as stable as the solid stirrup, and the metal uprights can pop out, which is the main reason a split stirrup is infrequently used.
Ankle Stops and Assists
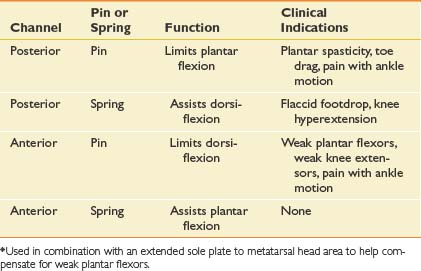
The ankle joint can be positioned so that it is in a neutral, dorsiflexed, or plantar-flexed position, depending on the gait disturbance. It can be set to permit a partial range of motion or to eliminate a certain motion. An understanding of the effect on the placement of pins and screws into the two channels of an ankle joint (see Figure 15-10) facilitates the proper orthotic prescription for the patient. This section reviews the common uses of the posterior stop (via pin), anterior stop (via pin), and the posterior dorsiflexion assist (via spring) of the orthotic metal ankle joint (Table 15-1). A spring in the anterior channel has not been demonstrated to be of clinical value.
Plantar Stop (Posterior Stop)
The plantar stop is used to control plantar spasticity or help incrementally stretch plantar contractures. The plantar stop is most commonly set at 90 degrees. A pin is inserted into the posterior channel of an ankle joint, such as that in Figure 15-10, to limit plantar flexion. An AFO with a plantar stop at 90 degrees produces a flexion moment at the knee during heel strike. Because the dorsiflexors cannot eccentrically activate to permit the foot to make contact with the ground, the ground reactive force remains posterior to the knee after heel strike, which creates a flexion moment at the knee (and possibly an unstable gait via buckling). The proximal portion of the AFO also has an effect on knee stability. The posterior portion of the proximal AFO exerts a forward push on the proximal leg to increase the knee flexion moment after heel strike (Figure 15-11). The opposite occurs at toe-off, with an extension moment created at the knee. This concept has been used to develop what has been referred to as a plastic ground reaction AFO, with a solid proximal anterior tibial closing that provides a greater influence on the knee. This device will be discussed in more detail later. The greater the plantar flexion resistance, the greater the flexion moment at the knee at heel strike, and the greater the need for active hip extensors to prevent the body from collapsing forward on a buckling knee.
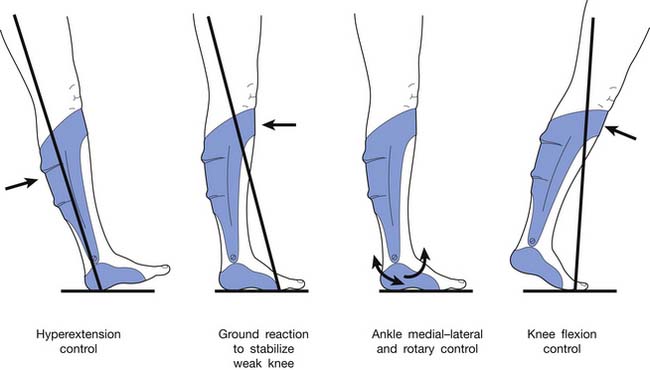
The posterior stop should be set at the minimal amount of plantar flexion required to clear the foot during swing-through.18 Remember, plantar flexion creates a knee extension moment at the knee from midstance to toe-off. This provides a more stable knee during gait than when the ankle plantar stops are set in any degree of dorsiflexion.
A balanced decision should be made between providing resistance to plantar flexion to clear the foot during the swing phase of gait and the amount of instability at the knee during the stance phase of gait. No AFO is effective in reducing the amount of knee flexion to “normal” levels during the stance phase of gait.20
Dorsiflexion Stop (Anterior Stop)
An anterior stop is used to substitute for the function of the gastrocnemius-soleus complex (Figure 15-12). It is used in conditions with weak calf muscles or weak quadriceps (because of its effect on the knee). Weak calf musculature allows the ankle to enter dorsiflexion, and dorsiflexion creates a knee flexion moment after heel strike. The anterior stop set at 5 degrees of dorsiflexion best substitutes for gastrocnemius-soleus function.18,20 Three muscle groups help stabilize the knee during the gait cycle: the quadriceps, hamstrings, and gastrocnemius-soleus complex. All three of these muscle groups cross the knee joint and should be clinically evaluated and considered when prescribing a lower limb orthosis.
The earlier the dorsiflexion stop occurs during the stance phase, the greater the extension moment at the knee. This is useful in clinical situations where quadriceps weakness is also present. If the extension moment at the knee is too great for too long, genu recurvatum (“back knee”) can occur. A balance should be obtained such that the extension at the knee is sufficient to stabilize the knee in extension yet prevent genu recurvatum. If too much dorsiflexion is permitted by the anterior stop, there will be too much knee flexion during gait from midstance to toe-off.
Dorsiflexion Assist (Posterior Spring)
The posterior spring (see Figure 15-6) serves two purposes. It substitutes for concentric contraction of dorsiflexors to prevent flaccid foot drop after toe-off. It also substitutes (inadequately) for the eccentric activation of the dorsiflexors after heel strike.
A summary of some of the common indications for the various channel components is found in Table 15-1.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


