22. Liver and pancreatic infections



Hepatitis
The classic clinical triad of jaundice, dark urine and pale stools (Fig. 3. 22.1) accompanying fever is often missing, particularly in children, who are more often asymptomatic. The vast majority of cases have a viral aetiology, with hepatitis A, B and C being the commonest causes.

Entamoeba histolytica and parasitic infections are common causes of hepatitis in tropical climates.
Diagnosis and management
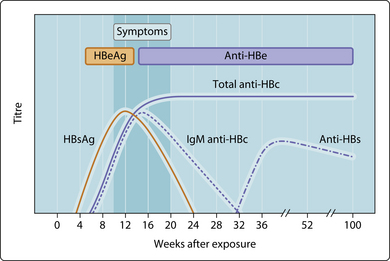
Diagnosis of viral (and leptospiral) infection is serological, by detection of either antigen or specific antibody. The detection of hepatitis B surface antigen (HBsAg) confirms the diagnosis of hepatitis B virus, and the presence of hepatitis B ‘e’ antigen (HBeAg) indicates a high infectious risk (Fig. 3.22.2). Other markers are determined in specific cases. Jaundice in carriers, in whom HBsAg persists for 6 months or more, is most likely to have another cause, which should be sought. Hepatitis A virus infection is diagnosed by specific IgM. Serological assays for the diagnosis of hepatitis C do not offer early diagnosis, as they are based on the detection of specific IgG, which may take several weeks to develop; diagnosis is, therefore, retrospective unless an earlier method such as gene amplification in the polymerase chain reaction is used.
< div class='tao-gold-member'>

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


