Chapter 42 Knee Pain of Neural Origin
INTRODUCTION
Nerves related to the knee include not only those that go in the skin about the surface of the knee joint but also mixed (motor and sensory) nerves that pass the knee on the way to their targets distal to this joint. In addition to these well-known nerves are those that innervate the knee joint. Each of these nerves is at risk of injury whenever (1) there is blunt force directed at the knee, (2) there is a stretch/traction injury to the musculoskeletal system of the knee joint, (3) there is an inversion sprain to the ankle, and (4) open or arthroscopic knee surgery has been performed. Whereas it is intuitively clear that a joint is innervated, the exact pathways of this innervation are curiously omitted from the classic and even the newer anatomy texts. For the human knee, the innervation pattern was not found to be described until 1994 during the author’s search for an etiology of knee pain unrelated to musculoskeletal dysfunction.25 The approach to knee pain described in this chapter follows closely that developed for wrist pain,8,16,20 which preceded the author’s interest in knee pain and led to a subsequent similar approach to those for shoulder pain1,3 and ankle pain.6,13,29
Nerves are at risk of injury from
Approach: knee pain that exists after musculoskeletal treatment is of neural origin.
PERIPHERAL NERVE ANATOMY RELATED TO THE KNEE
Innervation of the Human Knee Joint
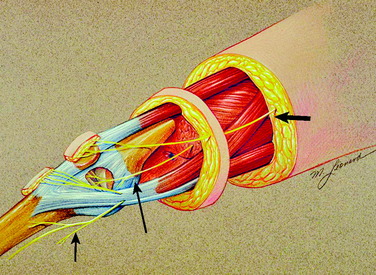
The innervation of the human knee joint is remarkably constant.25 On the medial aspect (Fig. 42-1), the femoral nerve branch that innervates the vastus medialis continues past its motor point and exits deep and distal to the vastus medialis. At this point, it lies deep to the medial retinaculum and becomes related to the medial recurrent geniculate artery and vein. This structure is termed the medial retinacular nerve. These structures, nerve and vessels, continue directly adjacent to the vastus medialis and superficial to the synovium to enter the ligamentous structures of the medial aspect of the knee. These fibers also continue toward the midline of the knee to innervate the undersurface of the patella (see Fig. 42-1).
On the lateral aspect of the knee (Fig. 42-2), a branch of the sciatic nerve leaves the popliteal fossa, travels laterally and anteriorly, emerges deep to the biceps tendon, and enters the space beneath the lateral retinaculum. In this location, the nerve is adjacent to the superior lateral geniculate artery and vein. This structure is termed the lateral retinacular nerve. These structures, the nerve and vessels, are immediately distal to the vastus lateralis and superficial to the synovium. The nerve enters the ligamentous structures of the lateral aspect of the knee (which have not yet been further defined histologically) and travels to the midline to innervate the undersurface of the patella.
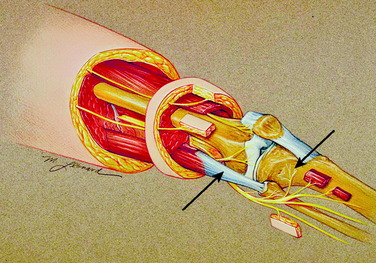
Anteriorly, another source of innervation is derived from the femoral nerve innervation of the vastus intermedius. This nerve continues on the surface of the periosteum to innervate the tissues around the prepatellar bursa. Finally, posteriorly, branches from the sciatic nerve enter the posterior knee joint capsule to provide innervation (see Fig. 42-2).
Innervation of the Proximal Tibiofibular Joint
Although many patients complain of “knee pain,” they may be pointing or referring to the region distal and lateral to the knee, which is the articulation between the fibular head and the tibia. This joint space is likely to be injured from fractures of the fibula or lateral tibial plateau or from high tibial osteotomy or a Maquet operative procedure. This space is innervated by the common peroneal nerve (see Fig. 42-2). As the common peroneal nerve travels from the popliteal fossa to the fibular head, it gives off a small (~1 mm in diameter) nerve that may enter this space posterior to the fibular head. The common peroneal nerve gives off a second branch to this space immediately as it curves anterior to the fibular head, at the junction with the fibular neck. This branch is also approximately 1 mm in diameter. The next branch of the common peroneal nerve goes to the tibialis anterior, which is a critical motor branch. In the operating room, the only way to identify the branch to the joint is to stimulate it electrically. No motor function will be elicited when the branch to the joint is stimulated. This is a critical step. This small branch often looks like epineurium.
Common Peroneal Nerve
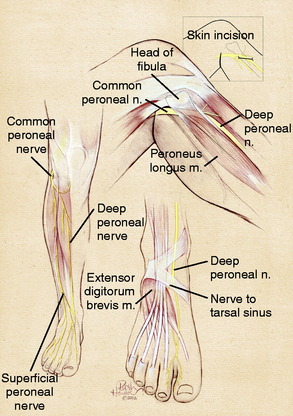
The common peroneal nerve is the lateral branch of the sciatic nerve. It can most often be identified as a distinct branch even to the sciatic notch. Therefore, in the thigh, there is clearly a common peroneal nerve even though it may be referred to as the sciatic nerve. In the distal thigh, the common peroneal nerve courses laterally, approaches the fibular head, and continues anteriorly to cross the fibular neck and enter the leg. As the common peroneal nerve approaches the fibular neck, it clearly divides into the superficial and the deep peroneal nerve, increasing in size as increased epineurium is required to ensheath these two branches (Fig. 42-3). The critical anatomic sites that can cause compression have long been appreciated to occur as the common peroneal nerve crosses the fibular neck, requiring division of the fascia of the peroneus longus fascia.35 With increasing experience, it has become evident that three other anatomic factors must be considered. A fibrous band exists beneath the peroneus longus in 20% of cadavers, but this band is present (and ranges from 5–15 mm in width) in 80% of patients requiring neurolysis.14 The surgeon must identify the common peroneal nerve by elevating it from the fibular neck, determine whether fibrous thickening in the lateral gastrocnemius muscle fascia is present, and finally, be certain that the overall entrance into the anterior and lateral compartments is sufficiently large.
Deep Peroneal Nerve
The deep peroneal nerve arises over the fibular neck as a discrete fascicle. It can be dissected proximally by microtechnique if necessary. Immediately after crossing the fibular neck, it gives off tiny branches to the tibialis anterior and the toe extensor muscles. In so doing, the deep peroneal nerve effectively tethers the common peroneal and its distal branches from having too much excursion. This predisposes the common peroneal nerve and its branches in this region to stretch/traction injuries. The entrapment site for the deep peroneal nerve is at the ankle, the “anterior tarsal tunnel,” which is a rare site for compression unless there has been a direct injury in this location. A more common site for compression is over the dorsum of the foot where the tendon of the extensor hallucis brevis represents the anatomic structure causing the compression. A portion of the tendon of the extensor hallucis brevis is excised in the region of the deep peroneal nerve5 (see Fig. 42-3).
Superficial Peroneal Nerve
The superficial peroneal nerve arises over the fibular neck from the common peroneal nerve. It can be dissected more proximally by microdissection if required. The motor innervation to the foot everters arises within the first 1 to 2 cm distal to the neck of the fibula. The known site of entrapment for this nerve is the region where it transitions from deep to the fascia into the subcutaneous tissues in the distal third of the leg. The typical division into its dorsomedial and dorsolateral branches occurs just proximal to the ankle in approximately 75% of patients (see Fig. 42-3). In the author’s experience, it is now clear that in at least 25% of cadavers and patients coming to surgery, this division can occur in the proximal third of the leg.2,39 This creates the situation in which the superficial peroneal nerve may be found in both the anterior and, its most usually described location, the lateral compartment. Indeed, the superficial peroneal nerve may be present in just the anterior compartment or within the septum between the two compartments.40 The anatomic variability means that any surgical approach to this nerve must open both the anterior and the lateral compartments.
Proximal Tibial Nerve
Although the tibial nerve (like the common peroneal nerve) arises at the sciatic notch as the medial component of the sciatic nerve, and is often clearly a distinct nerve in the thigh, the only well-described site for tibial nerve compression was at the medial ankle in the tarsal tunnel.31 It is now evident that the tibial nerve can be compressed in a site more proximal than the tarsal tunnel, and this site (just distal to the knee) is best described as the proximal tibial nerve to distinguish it from the tarsal tunnel region. Tibial nerve compression in the popliteal fossa has been described related to the presence of compartment syndrome or space-occupying masses, such as a popliteal artery or a Baker cyst.26,34 Although anatomy texts clearly depict a fibrous arch or soleal sling from which the soleus muscle arises, only recently has there been an anatomic study describing the relationship of this sling to the proximal tibial nerve.41 This sling lies at a mean distance of 9.3 cm (range, 7–13 cm) from the middle of the popliteal fossa and causes a visible narrowing of the tibial nerve over a length of 1.5 cm in 55% of the cadavers, with a severe constriction being found in 2% of the specimens. With injury to the knee, especially one associated with postoperative bleeding into the popliteal fossa, tibial nerve compression at this proximal site must be considered as a source of symptoms of numbness in the plantar aspect of the foot, with proximal referral to the knee region.
Lateral Femoral Cutaneous Nerve
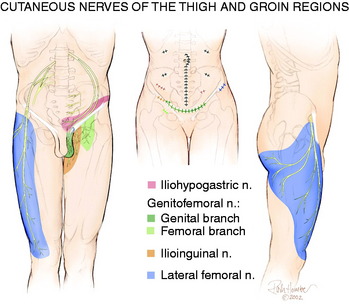
The lateral femoral cutaneous nerve has a great deal of anatomic variability related both to its location at the anterior superior iliac crest2 and to its innervated skin territory. If the location is within the inguinal ligament instead of inferior to it, the lateral femoral cutaneous nerve is at risk for compression or stretch/traction injury during falls, while wearing tight belts, during a seatbelt injury, or during manipulation of the knee with the patient on the operating room table. From Figure 42-4, it can be appreciated that compression of the lateral femoral cutaneous nerve can produce symptoms that include numbness or pain about the lateral aspect of the knee.37 This nerve, or the femoral nerve itself, can be injured during regional anesthesia given for knee surgery.22
Saphenous Nerve
The saphenous nerve is a branch of the femoral nerve that arises from the femoral nerve in the proximal thigh. Its cutaneous branches to the skin below the knee are well described and lie in a position to be injured directly from either a medial ankle arthroscopy portal or the midline incisions used for many surgical approaches to the knee. These branches can be directly injured by blunt trauma as well. Less well recognized is the nerve to the skin overlying the patellar itself. This is a branch of the femoral nerve, which may include sensory contribution from the obturator nerve joining within Hunter’s canal. The medial cutaneous nerve of the thigh (see Fig. 42-1) approaches from the medial aspect of the knee compared with the vertical approach taken by the anterior femoral cutaneous nerves.1 Even less well appreciated is that the saphenous nerve can be compressed in the distal thigh within Hunter’s canal. This is called adductor canal syndrome, which is rare in the absence of direct trauma to this region. Entrapment of the saphenous nerve in this location can present as medial knee pain.36
CLINICAL EVALUATION OF KNEE PAIN OF NEURAL ORIGIN
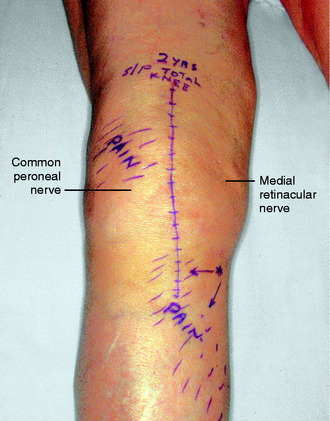
The physical examination is directed to identifying one or more sources of neural origin of the pain. First, the clinician should try to distinguish whether any skin territories are dysesthetic or painful when touched lightly. If so, these areas should be outlined. The most common distribution is that of the infrapatellar branch of the saphenous nerve; the second most common is the skin over the patella itself. These areas might be numb, indicating loss of sensation (Fig. 42-5). Once the pattern is identified, examine proximally along the course of the given nerve, observing for a trigger spot, which is either a true end-bulb neuroma or an in-continuity nerve lesion. The hypothesis is made that this nerve or these nerves are the source of the cutaneous pain; a diagnostic nerve block will be required to confirm this hypothesis.
Critical Points CLINICAL EVALUATION OF KNEE PAIN OF NEURAL ORIGIN
The physical examination is then directed to the joint afferents. Palpation is done deeply to the spot located just distal to the vastus medialis muscle, through the medial retinaculum to elicit pain from the medial retinacular nerve. Palpation is next done deeply to the area located just distal to the vastus lateralis muscle, through the lateral retinaculum, to elicit pain from the lateral retinacular nerve (Fig. 42-5). The hypothesis is made that the knee joint pain is due to an injury to one or both of the joint afferents; a diagnostic nerve block will be required to confirm this hypothesis. The medial cutaneous nerve to the thigh and the medial retinacular nerve can be blocked at the same area. Ten minutes after the nerve blocks, the patient is instructed to walk in the hallway, climb and descend a few steps, and even to kneel on a padded chair (Fig. 42-6). A reduction of 5 points on a visual analog scale; for example, from 10 to 5, where 10 represents the worst pain, is confirmation that sufficient relief of pain has occurred to permit surgery for partial knee denervation and resection of cutaneous neuromas.




FIGURE 42-6 Demonstration of the use of local anesthesia to block the suspected joint and cutaneous afferents in the patient with knee pain. A mixture of 0.5% bupivacaine (Marcaine) and 1% lidocaine (Xylocaine), each without epinephrine (upper left), is used to conduct the local block at the two sites indicated in Figure 42-5 to block the joint afferents most likely to be the source of joint pain. Additional blocks would also be done of cutaneous afferents. After the block, the patient should be able to climb stairs and kneel without the previous pain (as shown). There should be a reduction of at least 5 on the 10-point Likert scale in order for this block to be considered successful enough to recommend a partial knee denervation. If there is significant residual pain after the block, additional nerves causing this pain should be identified.
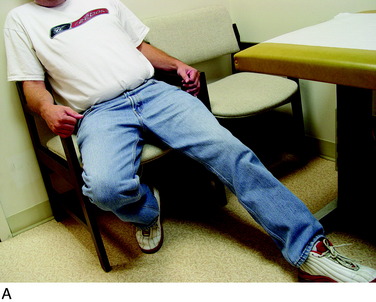
Finally, the groin should be examined to search for a Tinel sign over the lateral femoral cutaneous nerve. The patient will be noted to sit with the lower extremity extended at the hip joint (Fig. 42-7). The midthigh should be examined to search for a Tinel sign over Hunter’s adductor canal. This is most effectively done with the patient supine, and the effected leg externally rotated at the hip, leaving the knee bent. This stretches the adductor muscle group over the saphenous nerve. Then, gentle palpation over the canal produces a distal radiating painful response (Fig. 42-8).
< div class='tao-gold-member'>

Related posts:
 Human Movement and Anterior Cruciate Ligament Function: Anterior Cruciate Ligament Deficiency and Gait Mechanics
Human Movement and Anterior Cruciate Ligament Function: Anterior Cruciate Ligament Deficiency and Gait Mechanics
 Differences in Neuromuscular Characteristics between Male and Female Athletes
Differences in Neuromuscular Characteristics between Male and Female Athletes
 Rehabilitation after Articular Cartilage Procedures
Rehabilitation after Articular Cartilage Procedures
 Lateral, Posterior, and Cruciate Knee Anatomy
Lateral, Posterior, and Cruciate Knee Anatomy
 Meniscus Transplantation: Diagnosis, Operative Techniques, and Clinical Outcomes
Meniscus Transplantation: Diagnosis, Operative Techniques, and Clinical Outcomes
 Posterior Cruciate Ligament: Diagnosis, Operative Techniques, and Clinical Outcomes
Posterior Cruciate Ligament: Diagnosis, Operative Techniques, and Clinical Outcomes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


