Intraoperative Patient Positioning and Fluoroscopy for Fracture Surgery: A Suggested Guide To Obtaining The Quality Images
William Rossy
Optimal patient position and placement of the image intensifier aids the surgeon in obtaining accurate, real-time radiographs during surgery. When radiographic images are easily accessible, total operating room (OR) time is decreased and more accurate assessment of reduction and implant placement can be achieved. Regardless of operative site, the position of the patient and image intensifier should allow maximum access to the operative field, minimize surgical site obstruction, and allow for easy duplication of necessary intraoperative biplanar imaging.
UPPER EXTREMITY
Fractures about the Shoulder (Proximal Humerus/Clavicle)
Proximal Humerus
Patient placed in modified beach chair position
A bump can be placed underneath the medial border of the scapula to turn the patient slightly to the contralateral side.
The head is secured in a position in neutral rotation and flexion and the patient’s airway tube is secured, facing the noninjured side.
Image intensifier is most easily brought into field from above the patient in order to obtain necessary anteroposterior (AP) and axillary views of surgical site (Fig. 53.1).
Clavicle
Patient placed in modified beach chair position
Head secured in position with airway tube facing noninjured side
The image intensifier is brought from the contralateral side of patient to allow optimal visualization of the medial aspect of the clavicle and sternoclavicular joint (Fig. 53.2).
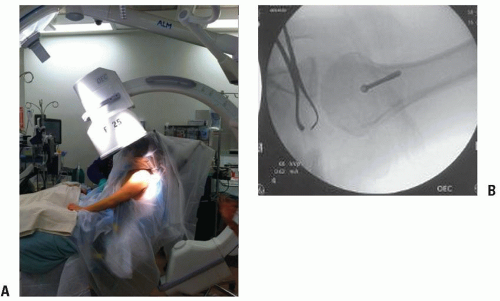 FIGURE 53.1 (A) Image intensifier brought in from above patient with bump beneath scapula improving the AP and axillary views. (B) Image demonstrating the axillary view that is easily obtained with this positioning. |
Fractures of the Humeral Shaft and Fractures about the Elbow
Fixation of humeral shaft fractures and fractures about the elbow can both be accomplished with the patient either supine or lateral. The specific position utilized is based partly on surgeon preference and partly
on fracture pattern, as fracture pattern may make one surgical approach preferable over another.
on fracture pattern, as fracture pattern may make one surgical approach preferable over another.
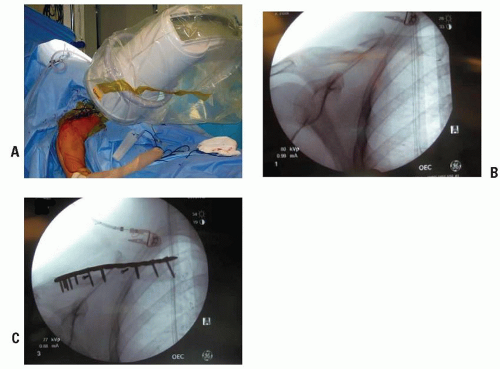 FIGURE 53.2 (A) Image intensifier brought in from contralateral side of injury enabling view of medial aspect of clavicle. (B) AP preoperative confirmed. (C) AP following fixation. |
Posterior Approach (Humeral Shaft, Distal Humerus, Olecranon)
Patient positioned in lateral decubitus position stabilized with a beanbag. The affected extremity can be hung over an armrest for added support and to facilitate reduction.
Axillary roll should be placed beneath the contralateral arm to minimize brachial plexus traction injury.
Image intensifier is again brought in from the ipsilateral side and can easily obtain desired AP and lateral views.
Can be reliably used for humeral shaft fractures or fractures about the elbow (Fig. 53.3)
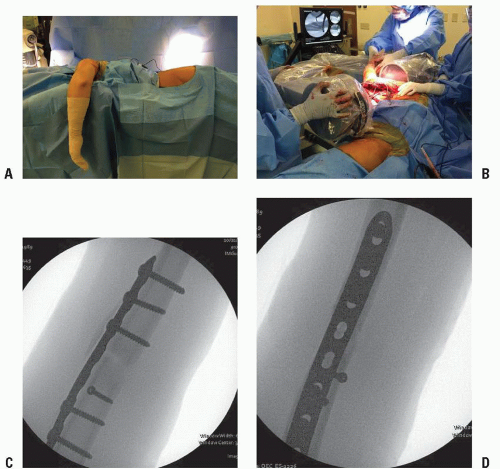 FIGURE 53.3 (A) The patient’s extremity is positioned over a beanbag with the arm stabilized by a beanbag and hanging over a radiolucent arm post. (B) The image intensifier is brought in from the ipsilateral side. (C,D) Intraoperative films demonstrate AP and lateral views of fracture site after internal fixation performed. |
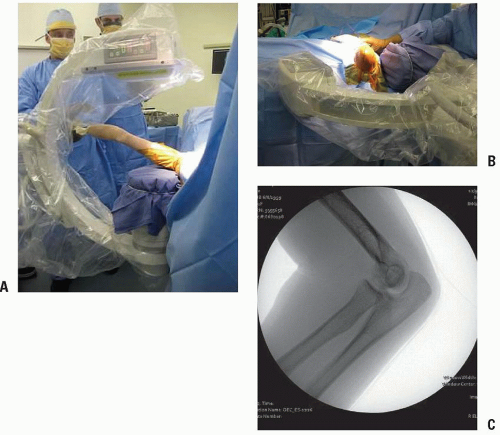 FIGURE 53.4 (A) With the patient translated to the edge of the bed, the operative arm can be easily manipulated to obtain the desired AP and (B) lateral views of the injured extremity. (C) Intraoperative lateral radiograph of elbow obtained. |
Direct Lateral and Anterolateral Approaches (Humeral Shaft, Distal Humerus, Radial Head, Proximal Radius, Proximal Ulna)
Patient is positioned supine on radiolucent table. If desired, a hand table can be used.
Patient translated to edge of bed so affected extremity can be freely manipulated to obtain necessary views of humeral shaft, distal humerus, or elbow.
Image intensifier is brought in from ipsilateral side of patient to allow machine to be brought in or taken away as necessary (Fig. 53.4).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


