Talus
EPIDEMIOLOGY
These are second in frequency among all tarsal fractures.
The incidence of fractures of the talus ranges from 0.1% to 0.85% of all fractures and 5% to 7% of foot injuries.
Approximately 14% to 26% of talar neck fractures have associated fracture of the medial malleolus.
Lateral process of the talus fractures are frequently seen in snowboarding injuries and account for 15% of all ankle injuries.
Fractures of the talar head are rare with an incidence of 3% to 5% of all fractures of the talus.
ANATOMY
The body of the talus is covered superiorly by the articular surface through which a person’s body weight is transmitted. The anterior aspect is wider than the posterior aspect, which confers intrinsic stability to the ankle (Fig. 40.1).
Medially and laterally, the articular cartilage extends plantar to articulate with the medial and lateral malleoli, respectively. The inferior surface of the body forms the articulation with the posterior facet of the calcaneus.
The neck of the talus is roughened by ligamentous attachments and vascular foramina. It deviates medially 15 to 25 degrees and is the most vulnerable to fracture.
The talar head has continuous articular facets for the navicular anteriorly, the spring ligament inferiorly, the sustentaculum tali posteroinferiorly, and the deltoid ligament medially.
There are two bony processes. The lateral process is wedge shaped and articulates with the posterior calcaneal facet inferomedially and the lateral malleolus superolaterally. The posterior process has a medial and lateral tubercle separated by a groove for the flexor hallucis longus tendon.
An os trigonum is present in up to 50% of normal feet. It arises from a separate ossification center just posterior to the lateral tubercle of the posterior talar process.
Sixty percent of the talus is covered by articular cartilage. No muscles originate from or insert onto the talus. The vascular supply is dependent on fascial structures to reach the talus; therefore, capsular disruptions may result in osteonecrosis.
The vascular supply to the talus consists of:
Arteries to the sinus tarsi (peroneal and dorsalis pedis arteries)
An artery of the tarsal canal (posterior tibial artery)
The deltoid artery (posterior tibial artery), which supplies the medial body
Capsular and ligamentous vessels and intraosseous anastomoses
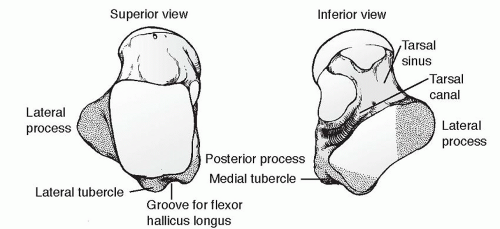 FIGURE 40.1 Superior and inferior views of the talus (stippling indicates the posterior and lateral processes). (From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and Green’s Fractures in Adults. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2006.) |
MECHANISM OF INJURY
Most commonly associated with a motor vehicle accident or a fall from a height with a component of hyperdorsiflexion of the ankle. The talar neck fractures as it impacts the anterior margin of the tibia.
“Aviator’s astragalus”: This historical term refers to the rudder bar of a crashing airplane impacting the plantar aspect of the foot, resulting in a talar neck fracture.
CLINICAL EVALUATION
Patients typically present with ankle pain.
Range of foot and ankle motion is typically painful and may elicit crepitus.
Diffuse swelling of the hindfoot may be present, with tenderness to palpation of the talus and subtalar joint.
Associated fractures of the foot and ankle are commonly seen with fractures of the talar neck and body.
RADIOGRAPHIC EVALUATION
Anteroposterior (AP), mortise, and lateral radiographs of the ankle, as well as AP, lateral, and oblique views of the foot are obtained.
Canale view: This provides an optimum view of the talar neck. Taken with the ankle in maximum equinus, the foot is placed on a cassette, pronated 15 degrees, and the radiographic source is directed cephalad 15 degrees from the vertical (Fig. 40.2). This view was described for evaluation of posttraumatic deformity and is difficult to obtain in the acute setting.
Computed tomography (CT) is helpful to characterize fracture pattern and displacement further and to assess articular involvement.
Technetium bone scans or magnetic resonance imaging (MRI) may be useful in evaluating possible occult talar fractures.
CLASSIFICATION
Anatomic
Lateral process fractures
Posterior process fractures
Talar head fractures
Talar body fractures
Talar neck fractures
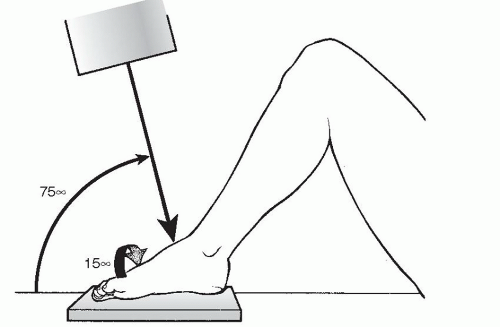 FIGURE 40.2 Canale and Kelly view of the foot. The correct position of the foot for x-ray evaluation is shown. (From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and Green’s Fractures in Adults. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2006.) |
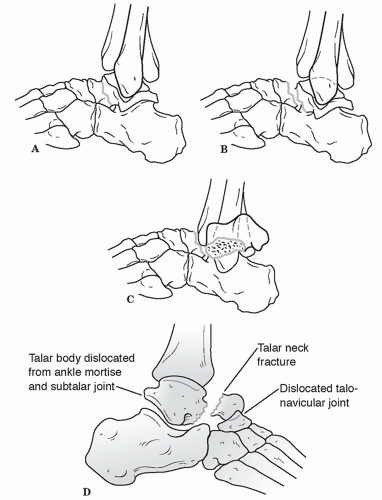 FIGURE 40.3 The three patterns of talar neck fractures as described by Hawkins. Note that type I fractures are nondisplaced. (A) Type I talar neck fractures with no displacement. (B) Type II talar neck fractures with displacement and subluxation of subtalar joint. (C) Type III talar neck fracture with displacement and dislocation of both ankle and subtalar joints. (D) Type IV talar neck fracture with dislocations of ankle, subtalar, and talonavicular joints. (From Bucholz RW, Heckman JD, eds. Rockwood and Green’s Fractures in Adults. 5th ed. Baltimore: Lippincott Williams & Wilkins; 2002.) |
Hawkins Classification of Talar Neck Fractures (Fig. 40.3)
Type I:




Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
