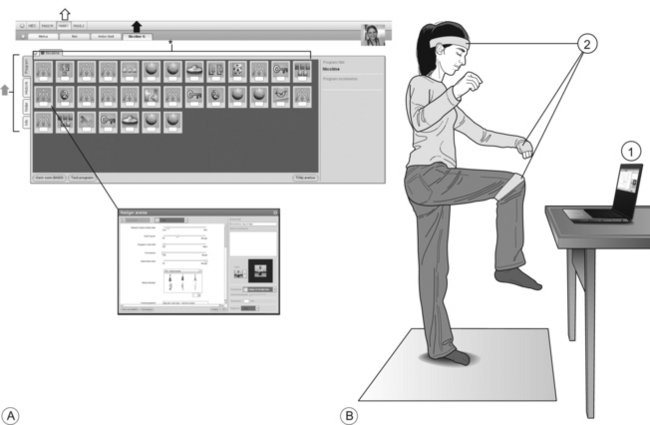
15 The necessity of early diagnosis and intensive long-lasting training of children with cerebral palsy (CP) has been argued elsewhere in this book and is in my opinion not disputable. However, nothing comes for free and both early diagnosis and early treatment cost money. Health welfare expenditures are rising throughout the world with every new advance in diagnosis and treatment forcing doctors and politicians to make unpleasant decisions about what to diagnose and what to treat unless we find ways of making cheaper diagnoses and cheaper treatments. And we have to face the reality: What really costs money is manpower. It is the human resources that we have to put into early diagnosis and early treatment that are the real limiting factors. We may argue that children with cerebral palsy should be diagnosed some years earlier and receive more intensive treatment for many more years than what is the case now, but unless we minimize the human resources (doctors, therapists) required, we will be met by administrators, insurance companies and politicians who fail to find the money, and all the good ideas that we have may never see the light of day. In my opinion, there is therefore no doubt that we will need to find ways of using technology to supplement some of the human resources involved in diagnosis and treatment. I believe that there is a huge potential that has not been exploited sufficiently in the past, but which becomes more and more difficult to ignore with the increasing economic pressure from increasing health care expenditures, on the one hand, to the explosion of computer, internet and smartphone technologies that offer themselves as intelligent (and cheap) solutions, on the other. There is in my mind no doubt that we will see an explosion in intelligent interactive technologies for diagnosis and treatment within the next five to ten years, not only in the field of neurology but also throughout health care. In this chapter I will highlight a few of the possibilities which have already been tested or are about to be tested and which are directly relevant in relation to ensuring efficient and relatively low cost early diagnosis and treatment of children with cerebral palsy. CP is sufficiently rare, even in very premature infants, to make a specific diagnosis necessary before initiating any treatment. Imaging techniques such as serial cranial ultrasound and magnetic resonance imaging certainly provide efficient means of screening for brain damage in premature children (DeVries et al., 2011; Milligan, 2010), but are not feasible or affordable for the larger group of infants born at term, although it is in this group the largest number of infants with CP is found (Krägeloh-Mann and Cans, 2009). There is also only a limited relation between observations from brain imaging and the clinical abnormalities in individual infants with a large number of false-positive (early lesions compensated by later plastic changes) and false-negative (especially the multiple smaller lesions caused by oxygen deficits) findings (Bax et al., 2006; Korzeniewski et al., 2008). Although the relatively rare severe brain lesions are usually noticed early after birth, the much more frequent smaller lesions that produce less apparent cognitive, sensory or motor deficits are often not detected until the child is several years old. This means months and years without proper treatment. What can we do to improve this? One way may be to implement early diagnosis based on the general movement assessment system introduced by Prechtl and co-workers (Einspieler et al., 1997; Prechtl et al., 1993) (see Chapter 8). Several studies have demonstrated that this assessment has a very high predictive value and may be applied to infants as young as three months (Cioni et al., 1997; Einspieler et al., 1997; Guzzetta et al., 2003; Hadders-Algra, 2004). However, one practical problem is that the assessment requires a trained and experienced clinician or therapist who needs to observe the child for a relatively long time either in real life or on a video recording under standardized circumstances. This has prevented the system from being introduced on a larger scale for screening of infants. A solution to this problem may be to use computer algorithms that are now very powerful to analyse video recordings of the children and detect possible abnormalities in their movement pattern. This would help to minimize the time that clinicians or therapists would need to spend on healthy infants and instead focus their attention on infants who have been identified by the computer algorithm as having diminished or abnormal movement. This would also guarantee a certain level of quality and reproducibility in the diagnosis. Such automatized computer diagnostic systems have already been developed and tested (Adde et al., 2009, 2010; Karch et al., 2010, 2012). The systems do show promise but there are still technical challenges that need to be overcome. One is that optimal tracking of movements requires 3D motion analysis that until recently had been expensive and complex to work with in practice, especially due to the necessity of placing markers on the infant and calibration of the system. With the recent development in interactive gaming technologies (Kinect from Microsoft and similar), 3D cameras and motion analysis software that do not require markers have become very cheap. This opens up the possibility of a large-scale automatized screening system with video recordings that can be obtained in the home of the infant and transferred to a central health care unit, through the internet, where a diagnosis can be facilitated by automatized computer algorithms. The race has already started for making this come true. One of the challenges to initiation of early treatment in CP is to ensure sufficiently intensive training for a sufficiently long time. The amount of training that can be offered through individual therapeutic sessions as part of public health systems is insufficient to drive neuroplastic changes (Lang et al., 2009) and significant functional improvements will therefore have to rely on intensive high-quality training conducted by the families in their own home (Katz-Leurer et al., 2009; Lang et al., 2009) and guided by a well-trained clinical movement scientist and therapist. But how do we ensure sufficient high quality in the training if it is conducted without the supervision of an appropriately trained therapist? How do we ensure that training is made progressively challenging as the infant matures and masters new skills? And, probably most important, how do we ensure that the child and the families remain motivated and continue training as intensively and for as long time as required? One of the answers to these questions may be to develop interactive technologies for supervised training at home (Bilde et al., 2011; Napolitano et al., 2003; van den Berg et al., 2006). One such system (Move it to improve it; MiTii) has been developed at the Helene Elsass Center in Copenhagen, Denmark, and is now being tested in randomized controlled studies in Denmark and Australia. A feasibility and proof of principle study on a sample of nine children in the age group 6–12 years was recently published (Bilde et al., 2011). The training system is based on individualized interactive computer training modules delivered through the internet directly to the child’s home (Fig. 15.1) (Bilde et al., 2011). Figure 15.1 The MiTii training system. (A) Illustration made from screenshots of MiTii. The individual settings are made and progressively modified in the editing window. The first step in editing is to choose the group of patients (open arrow). The next step is to select the individual client details (solid black arrow). Each individual training programme is made up of a sequence of exercises. The different exercises are represented by icons that can be moved around freely to accomplish the optimal individual sequence. The full programme covers from 30–45 minutes (asterisk). In subjacent layers the editing screens offer possibilities for visual feedback from the patients in training, showing intensity and training time from the previous day, week, month or the total training course. This feedback information is obtained automatically on line. A basic case record system is provided to store personal patient information (grey arrow). A double click on each of the icons opens up a new window (seen here as the overlay on the screen). where the range of parameters for each individual exercise—speed, number of repetitions, placing of target and pick-up area on screen, seize of objects, time to react, etc.—can be set. A special database makes it easy to change the graphics for the exercise, e.g., pictures from the patient’s own daily life can be uploaded to the database. Changes in the graphic environments are normally performed once a week as it provides excellent motivation. If needed, a video can be uploaded with the exercise giving the therapist a possibility to show, in advance, what the patient is asked to do. The video will automatically play in advance of the exercise. Other parameters to be modified include disturbances, i.e., graphic animations that challenge the attention of the person in training, and time bombs that bring pressure to finishing the exercise in a predetermined space of time. (B) MiTii at work in a home environment. The hardware necessary comprises a computer (1) with a webcam and an internet connection. Elastic bands (2) are placed around the head, on the wrists, the knees, the elbows or wherever the therapists find it to meet the requirements. The colour of the elastic band is what controls MiTii. Thus, the therapists may decide which part of the body they want to act as interface to the webcam. These settings can be changed from game to game within the daily programme or over time as the training develops. [Reprinted with kind permission of the Helene Elsass Center.]
Interactive technologies for diagnosis and treatment in infants with cerebral palsy
Early diagnosis: a role for technology?
Early treatment: a role for interactive technologies?
Related posts:
 Re-thinking the brain: new insights into early experience and brain development
Effects of motor activity on brain and muscle development in cerebral palsy
Functional effects of neural impairments and subsequent adaptations
Treadmill training in early infancy: sensory and motor effects
Very early upper limb interventions for infants with asymmetric brain lesions
Training lower limb performance in early infancy: Support, balance and propulsion
Re-thinking the brain: new insights into early experience and brain development
Effects of motor activity on brain and muscle development in cerebral palsy
Functional effects of neural impairments and subsequent adaptations
Treadmill training in early infancy: sensory and motor effects
Very early upper limb interventions for infants with asymmetric brain lesions
Training lower limb performance in early infancy: Support, balance and propulsion
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Musculoskeletal Key
Fastest Musculoskeletal Insight Engine
