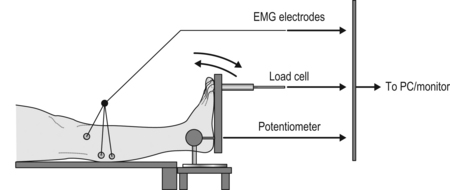
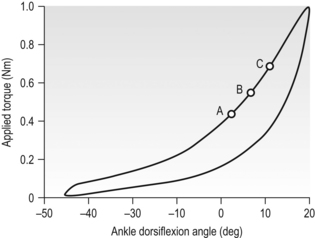
Annotation B Study 1: Non-reflex stiffness in children with CP Study 2: Distinguishing between reflex and non-reflex stiffness in children with CP in a clinical scale Study 3: Non-reflex stiffness can influence the motor performance of children with CP Study 4: Effect of botulinum injections on non-reflex stiffness in children with CP Suggestions for future studies Progressive plantarflexor muscle dysfunction is common, particularly in children with hemiplegia or diplegia and may result from changes in muscle activation, myotendinous length and stiffness (Becher et al., 1998). When a non-contracting (resting) muscle is stretched in a child with cerebral palsy (CP), any force opposing the movement is due to tension originating through the passive mechanical properties of the muscle, as well as any abnormal muscle activation evoked in spastic muscle. This resistance, however, is commonly recognized as primarily a manifestation of enhanced stretch reflex activity (Mirbagheri et al., 2000) that is often presented as the primary opponent to movement. Researchers frequently group passive myotendinous stiffness under a general label of spasticity/contracture and may not treat it as a separate impairment. For a number of years the abnormal muscle activation evoked in muscle was considered to be the main contributor to the resistance to movement. However, work by Dietz and Berger (1983) was the first to suggest that muscle stiffness during locomotion in patients with spasticity was due more to changed passive mechanical properties of the muscle than to heightened stretch reflexes in both adults and children with spastic cerebral palsy. All studies were approved through both the Hospital Ethics Committee of The Children’s Hospital at Westmead, Sydney, Australia and the Human Research Ethics Committee of the University of Sydney. Participants were recruited through the Child Assessment Centre in The Children’s Hospital at Westmead and through open advertisement for typically developing children. All participants were aged between 4 and 10 years. Participants were consecutively selected based on inclusion and exclusion criteria, and their willingness to participate. Full details of the participants, including inclusion and exclusion criteria, demographic detail and clinical status are given for each study in the relevant publication. A specially constructed ankle measurement device, similar to that described by Moseley et al. (2001) was used for this aspect of the studies (Fig. B.1). It consisted of a footplate hinged to a support bracket for the lower leg, with a rotary potentiometer (Model 157, RS Australia, Sydney) aligned with the lateral malleolus. The footplate and axis of rotation were adjustable to match the dimensions of the child. A 450 N load cell (XTRAN S1W, Applied Measurement Australia Pty, Oakleigh) was attached perpendicular to the footplate to measure resistance to movement. A handle was attached to allow manual oscillation of the footplate. Figure B.1 Schematic of ankle measurement device and experimental procedure. EMG electrodes detect muscle activity in medial gastrocnemius, soleus and tibialis anterior. Applied torque is calculated from the product of the force measured through the load cell and the perpendicular distance to the axis of rotation (potentiometer). The lower leg is clear of the support surface. High inter-rater and intra-rater reliability has previously been demonstrated for the measurement of passive torque and ankle displacement using similar techniques (intraclass correlation coefficient (ICC)>0.86) (Chesworth and Vandervoort, 1988) and the procedure has been shown to be highly responsive to change in soft tissue stiffness characteristics (Sinkjaer et al., 1988). Each child lay supine with the foot placed in the ankle apparatus and positioned, by visual approximation, such that the point midway between the lateral and medial malleolus in the sagittal plane was aligned with the axis of rotation of the device. The participant’s foot was secured to the footplate with Velcro® straps, the knee was placed in an extended position, and light pressure was applied by the researcher’s hand above the knee over the thigh to ensure that knee position was maintained. The calf was free of contact and clear of all surfaces and structures. In the children with CP, the affected or more affected leg was tested; in typically developing children, the leg tested was randomly selected. The researcher rotated the foot passively in a sinusoidal pattern around the ankle from full plantarflexion to full available dorsiflexion (determined visually by loss of heel contact). All children were instructed to keep their legs relaxed and to avoid assisting or resisting the motion during the sinusoidal rotation. Electromyographic (EMG) activity of the soleus, medial gastrocnemius and tibialis anterior muscles was recorded simultaneously with ankle rotation, using a telemetric 16-channel EMG unit (Telemyo 2400 R G2 system, Noraxon, Arizona) with a sampling rate of 3000 Hz. We used disposable, self-adhesive Ag/AgCl bipolar surface electrodes (Kendall Medi-Trace Mini 130 Foam ECG Electrodes, Neurotronics, Randwick, NSW), placing pairs of electrodes parallel with the muscle fibre direction with minimal inter-electrode distance. Before electrode placement, we cleaned the skin with isopropyl alcohol. The location of electrodes was based on contemporary recommendations (Hermens et al., 2000). EMG acquisition enabled monitoring of muscle activity during the test. Torque values were extracted from the data at predetermined dorsiflexion angles (0°, 5° and 10°; Fig. B.2, points A, B and C, respectively). These provided an indication of the torque necessary to displace the ankle to comparable positions for each group tested. Stiffness was computed as the slope of the line between 0° and 5° of dorsiflexion. Hysteresis, expressing the energy absorbed by the muscle–tendon unit during the loading/unloading cycle, was calculated as the area enclosed between the loading and unloading curves of applied torque against ankle angle. This study revealed that the plantarflexors of the children with CP were much less mechanically compliant than an age-matched group of typically developing children (Alhusaini et al., 2010a). Torques at predetermined joint angles, ankle stiffness (slope of curve) and hysteresis were almost three times as great in the children with CP compared with the typically developing group (p<0.001). These findings are important, particularly as we know that non-reflex stiffness in children with CP has not been described or quantified, nor have the effects been recognized of adaptive changes such as decreased muscle extensibility on motor development (Lambertz et al., 2003). This knowledge, therefore, has the potential to improve clinical practice by furthering what is known about the changes in the muscle’s intrinsic properties and broadening physiotherapists’ understanding about the effects of such changes in these children. The attempt was made to expose the calf muscle to conditions similar to those found during normal gait by using a sinusoidal movement that was similar in angular velocity and range of motion to that encountered during the stance phase of walking (Ada et al., 1998; Becher et al., 1998), while also avoiding stimulation of reflex hyperactivity in the calf muscles. Although this criterion was not always easy to achieve, and the responses of the children did vary in their ability to relax, it was possible to produce at least one complete cycle in each test during which EMG activity was silent. This situation, therefore, fulfilled the requirement for measurement of the passive myotendinous characteristics. Torque–angle curves at velocities up to 70 degrees/second show the characteristic shape of tissue stretch only (van der Salm et al., 2005). In a study of adults exhibiting spastic hypertonia, it was reported that, even at stretch velocities of 120 degrees/second, only four of 15 people demonstrated reflex responses in the triceps surae (Rabita et al., 2005). The sinusoidal movement speeds used in the experiments were felt to be adequate to measure the passive myotendinous stiffness parameters while not eliciting simultaneous reflex activity. Although the oscillation frequency was significantly different between groups, the children with CP, who were more likely to respond with hyper-reflexia, were stretched at the slightly lower rate, consistent with the subjective need to maintain a relaxed, passive movement.
Findings from a series of studies of passive mechanical properties of muscle in young children with cerebral palsy
Methodology
Study 1: Non-reflex stiffness in children with CP
Related posts:
 Re-thinking the brain: new insights into early experience and brain development
Effects of motor activity on brain and muscle development in cerebral palsy
Functional effects of neural impairments and subsequent adaptations
Treadmill training in early infancy: sensory and motor effects
Very early upper limb interventions for infants with asymmetric brain lesions
Training lower limb performance in early infancy: Support, balance and propulsion
Re-thinking the brain: new insights into early experience and brain development
Effects of motor activity on brain and muscle development in cerebral palsy
Functional effects of neural impairments and subsequent adaptations
Treadmill training in early infancy: sensory and motor effects
Very early upper limb interventions for infants with asymmetric brain lesions
Training lower limb performance in early infancy: Support, balance and propulsion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


