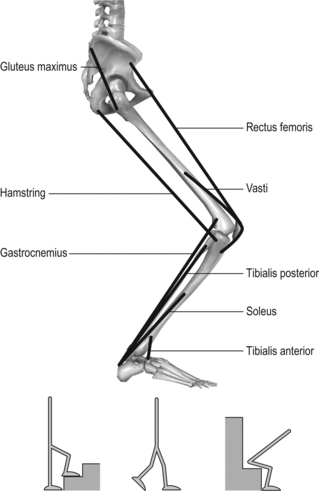
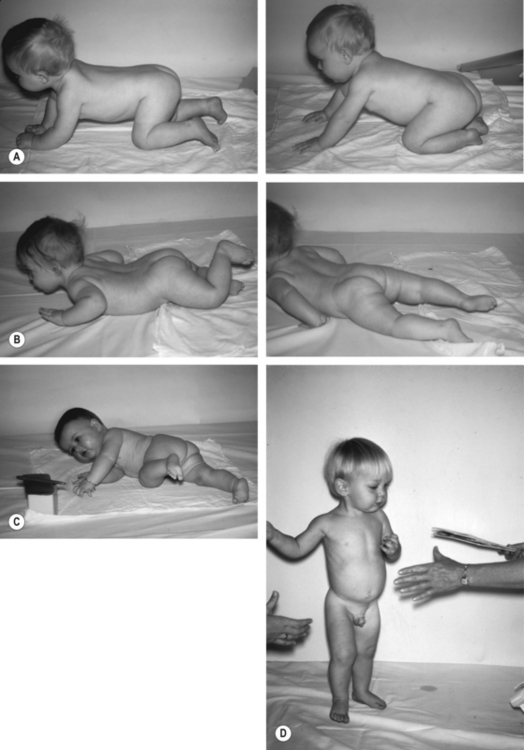
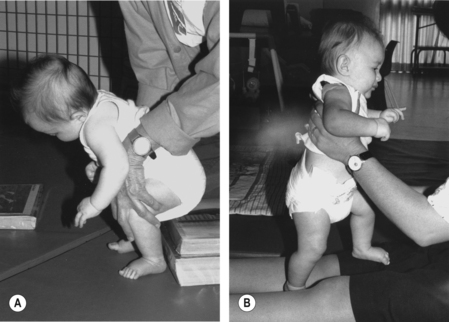
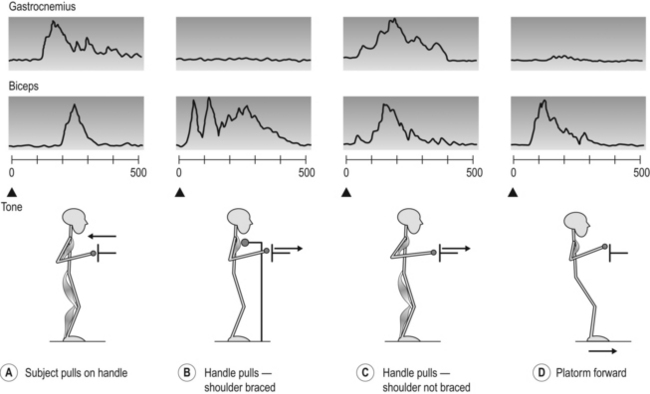
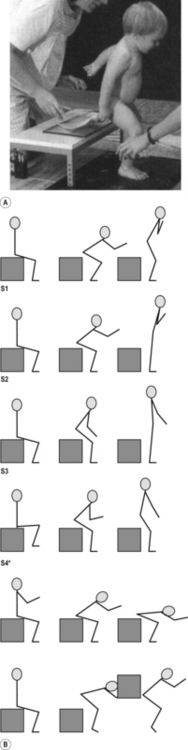
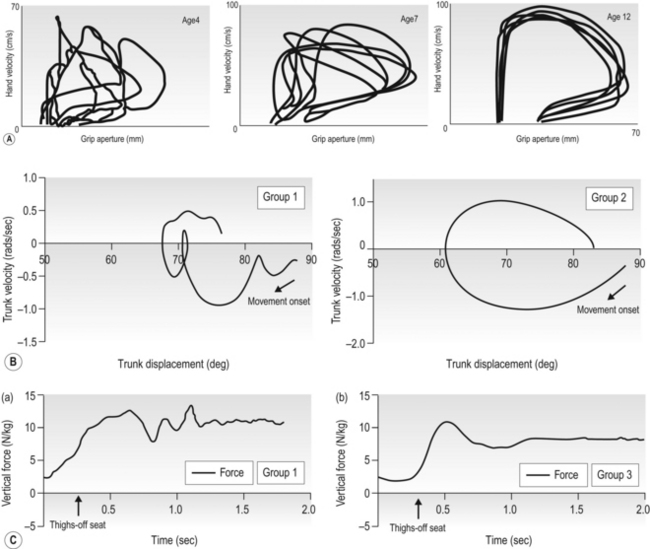
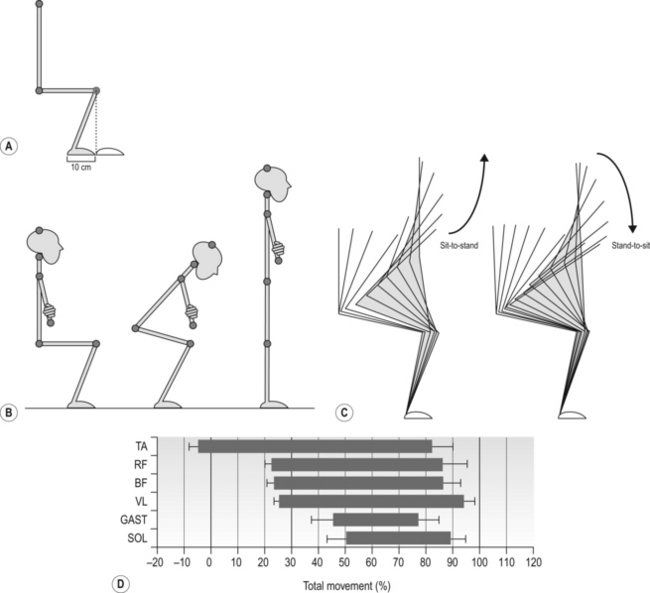
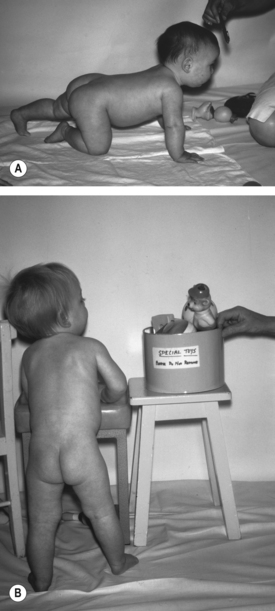
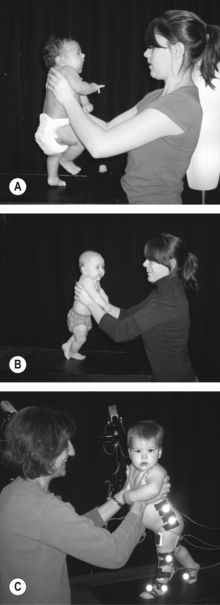
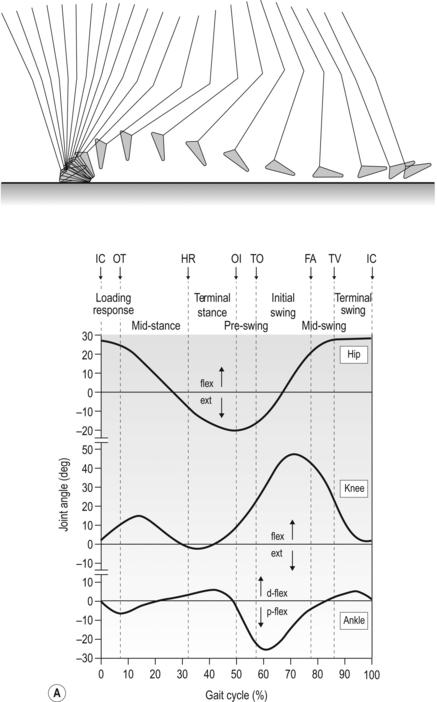
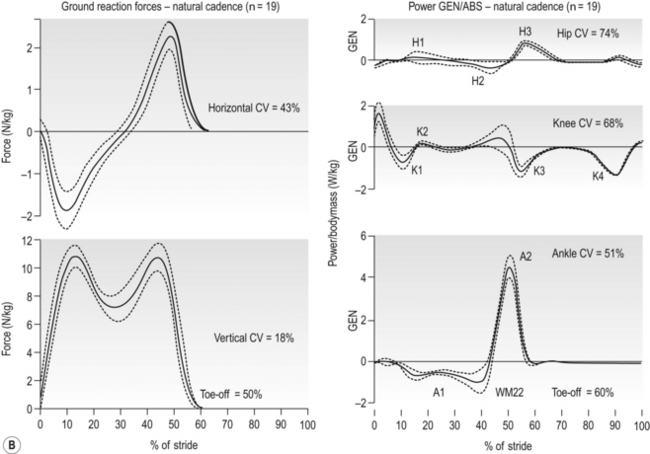
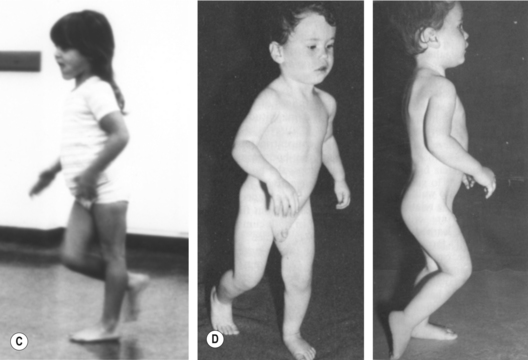
11 Part 1: support, balance, propulsion Development of lower limb motor skills Part 2: guidelines for activity-based intervention in infancy Optimizing support and balance Functional activities for the lower limbs The development of the brain and corticospinal tract in the infant with cerebral palsy (CP) may depend on early and varied use of the limbs. A full-term newborn infant in the early weeks of life begins to adapt to and take advantage of a new and gravitational environment, and over the first weeks begins an exploration of the possibilities available. Much of the first two years is spent learning how to balance the body and develop fundamental skills. A review of the anatomical and biomechanical characteristics of the lower limbs makes it clear that their basic action, underlying most of the actions of daily life, is flexion and extension at hips, knees and ankles (Fig. 11.1). When the feet are on the ground, the lower limbs support the body mass, balance it over the base of support, and propel it in the desired direction (Forssberg, 1982). Figure 11.1 Diagram showing lower limb segments and eight functional muscle groups affecting segmental movement with feet on the support surface. [Reproduced with permission from Kuo and Zajac (1993) A biomechanical analysis of muscle strength as a limiting factor in standing posture. J Biomech 26:137–150, with permission from Elsevier.] Simplifying motor function in this way has enabled the development, over the past three decades, of training and exercise guidelines for adult neurological rehabilitation. These programme consist of task-oriented exercises and activities that are focused on muscle activation, contractility and strength, and on developing co-ordination or motor control of the lower limbs as they flex and extend, support, balance and move the body mass in actions such as standing up and sitting down, squatting to pick up an object on the floor and standing up again, walking up and down stairs and slopes (Carr and Shepherd, 2003, 2010). The focus is on developing skill, learning to control body and limbs to produce effective and efficient movements. The exercise guidelines developed for adult neurorehabilitation, since they are developed out of applied biomechanics, functional anatomy and motor learning processes, are also applicable to infants and children with CP, incorporated into play and activity-related exercises (Damiano, 2006; Shepherd, 1995; Ulrich, 2010). However, infants with CP not only experience the effects of a lesion of the central motor systems but also, as they grow, the secondary effects on the musculoskeletal system of poor muscle contractility, weakness and inactivity. These include changes to muscle morphology and function, and to bone structure. The significance of these secondary effects should not be underestimated. Due to recent technological advances and the resultant research, these secondary effects are predictable and this means they may also be preventable. The alignment of the limbs, muscle morphology, bone structure and shape are dependent on how the infant learns to move, specifically on the stresses provided by the musculature of the limb. If for example, the hip flexors lose their extensibility and develop contracture the alignment of the lower limb is altered. Figure 11.11C, D illustrates the resultant pattern of movement as the small child with hemiplegic or diplegic CP walks. The crouch gait of children with diplegia is described by Arnold and Delp (2005). Developments in technology are enabling detailed examination of bone structure in children with diplegia, outlining the altered features of long bones (Carriero et al., 2009), and the altered morphology of muscles (see Chapters 6 and 7). The shape (form or topology) of functional movements (see Fig. 11.8) is dependent on co-operative action from major abductor/adductor and rotator muscles in addition to flexion and extension. The strength and control of basic lower limb movements depends also on muscles within the trunk that, although they do not themselves move the limbs, contribute to lower limb movements by stabilizing the muscle attachments on the pelvis and lumbar spine. Early weight-bearing and lower limb flexion/extension activities provide the stresses critical for stimulating bone growth and density, for development and growth of muscle, and the experiences that will foster the learning processes that underpin motor development. Targeted training of the lower limbs in infants with CP appears to have been neglected in the literature in comparison to the upper limbs. Chen and colleagues (2002) suggested that this might have resulted from a view that although infants are making purposeful reaching movements with the upper limbs within the early months, the lower limbs appear to be moving spontaneously in random kicking actions until required to perform purposeful weight-bearing activities. This neglect may also be due to the long-held view that upper limb actions are ‘fine motor skills’ while those of the lower limb, including balancing and locomotion, are ‘gross motor skills’. These terms have become meaningless as neuroscience and biomechanics teach us about the complexity and flexibility of motor control mechanisms, particularly those complex and finely tuned balance adjustments that occur as a critical part of our most critical everyday actions. Effective performance of standing up and sitting down, walking, reaching out for a variety of objects and manipulating them to achieve desired goals in different environments is critical to independent living. Most of our goal-directed motor behaviour is carried out when we are upright, in sitting or standing, and infants need the opportunity to focus on developing a functional linkage between upper and lower limbs (and including the vertebral joints) in the context of these two positions most critical for independence. Emphasis on sitting and standing enables the infant to develop the necessary orienting behaviours and balance mechanisms that enable them to explore and attend to their environment, communicate with others, and to develop the ability to formulate and carry out their goals. In the upright position infants, driven by their need for visual focus, also learn to control their head position. This is necessary for the development of visual acuity, visuomotor control and ability to pay attention, as well as eye contact for communication with others, all of which function together with independent head movement (Chapman, 2002). It is now recognized that the varied actions practiced by infants as they grow and learn, as they become stronger and develop more control, depend to a large extent on their opportunities, in particular their curiosity, drive and determination, their environment, and the effects of cultural influences within the family on child-rearing practices. Given the opportunity, and encouraged and assisted by parents and siblings, infants practice intensively, exploring the possibilities of crawling, creeping, standing and walking; they push and pull up from prone and supine, squat and stand up on a parent’s lap, kneel on one or both legs, cruise sideways along the furniture (Figs 11.2 and 11.3). The more the infant is allowed to explore and experiment with movement, the more he/she learns. Figure 11.2 (A) On hands and knees rocking forward and backward, testing the possibilities, learning to shift weight. (B) In prone, practicing extension of head and spine; progressing along the floor by pulling with arms and pushing with legs. (C) Mastery of rolling over involving the whole body working as one unit. (D) Just prior to the first independent steps in a forward direction. Figure 11.3 Two task-specific exercises to stimulate extensor muscle activation, increase extensor muscle strength, and preserve muscle extensibility. (A) Assisted sit-stand-sit: some assistance ensures knees are forward (i.e., ankles sufficiently dorsiflexed) with some downward pressure so the infant gets the idea of pushing down through the feet. (B) Step up and down on someone’s lap. The infant is steadied to prevent a fall but she raises and lowers her body mass herself. This chapter is focused on the details of intervention: on methods of encouraging and driving the infant’s own actions, and on setting up an interesting and challenging environment that enables the infant to practice using the lower limbs to support and balance the body mass. Guidance and constraint are provided when necessary. The infant is encouraged and assisted to be active and to explore, to practice a variety of movements that increase activation, contractility and strength of muscles, as well as preserve muscle extensibility (Fig. 11.2). Whatever the action to be learned, the infant needs to support the body through the lower limbs, balance it throughout the action, and, with many actions including walking and standing up, propel the body in the desired direction. The aims of intervention are to increase mobility, train functional actions (promote skill learning), and to activate and exercise muscles (for increased contractility, strength, extensibility, intersegmental co-ordination). The aims of prevention are to minimize changes to muscle morphology that may negatively impact functional performance, and to monitor during functional training, and if necessary correct, lower limb alignment that may negatively impact bone (and joint) alignment. Support of upper body over lower limbs In standing, support is brought about by the generation of the extensor muscle activity necessary to maintain segmental alignment in the presence of gravitational forces working to collapse the limbs. Many mono- and bi-articular muscles that span hip, knee and ankle joints work co-operatively across the three joints to maintain support and to balance the body mass over the thighs and feet (in sitting), feet (in standing) or knees (in kneeling). The co-operative extensor muscle force throughout each limb as we flex and extend hips, knees and ankles in standing and when standing up is illustrated by the ‘support moment of force’, an algebraic summation of the moments of force acting over the three joints, demonstrated in biomechanical studies of walking (Winter, 1987) and sit-to-stand (Shepherd and Gentile, 1994). Any reduction of extensor force at one joint can be made up for by increased moments of force at the other two joints. Muscles within the trunk that rotate, flex and extend the vertebral joints provide flexibility and stability to the movements of the upper and lower limbs. The ability to balance the body mass over the lower limbs enables us to move about under different conditions and for a variety of different goals. Movements that balance us and prevent a fall include adduction/abduction and rotation movements at the hips, and movements within the spine, as well as the basic flexion/extension of the hips, knees and ankles, and small movements at the joints of the feet. These movements control the body mass as it moves about over the base of support, ensuring the body’s centre of mass (CoM) stays within the base of support. Ongoing neuromotor interactions between our intent (pick up an object from the floor) and information from tactile, pressure and motion sensors (including plantar load receptors in soles of feet, and muscle and tendon receptors), and from vision, anticipate upcoming destabilizations, ensure ongoing musculoskeletal responsiveness throughout the action or a quick enough response to an unexpected perturbation to prevent a fall. The need for motor control is magnified when the base of support is small and when the body’s centre of gravity (CoG) is far from the support base, as in walking and standing on one leg. The mechanical problem of remaining balanced in the presence of the destabilizing forces that occur as we move is a particular challenge to the corticospinal system. Anticipatory and ongoing adjustments, and responses to unexpected perturbations, ensure the body is aligned and balanced over the base of support, stabilizing parts of the body while other parts move, and preventing a fall (Ghez, 1991). Even simple actions such a raising an arm in standing, or taking a deep breath, require initial (anticipatory/preparatory) and ongoing muscle activations. The muscle activations and joint movements (called ‘postural adjustments’) that balance us as we move about are flexible and vary specifically according to task and context (Belenkii et al., 1967; Cordo and Nashner, 1982; Eng et al., 1992; Smart et al., 2004) (Fig. 11.4). When bearing weight through the lower limbs and learning to stand up and sit down, reach for an object in standing or in sitting, squat to pick up an object, and to walk, balance is always a major focus of the neuromotor system. Once they can stand independently, although with frequent falls, infants practice balancing in standing and taking steps. They often prefer independence when walking, and will take a few steps unaided rather than hold a parent’s hand. Figure 11.4 An example of the task- and context-specificity of muscle activity. An arm muscle (biceps brachii) and a leg muscle (gastrocnemius) were monitored during different tasks. (A) The subject pulls on the handle. (B) The subject leans against a chest support, unexpected movement of the handle. (C) As in (B), but subject is free standing. (D) Unexpected forward movement of the platform. [Adapted with permission from Nashner LM (1983) Analysis of movement control in man using the movable platform. In: Desmedt JE (Ed.), Motor Control Mechanisms in Health & Disease. Raven Press, New York.] Moving the body mass requires the generation and timing of muscle forces to accelerate the body in the desired direction: forward and upward to stand up from a seat and from a squat, more vigorously in jumping vertically and walking fast. Leg extensor muscles increase in strength and ability to generate a powerful contraction as infants practice squatting to standing and sitting to standing (Liao et al., 2007). Calf muscles and hip extensors propel the body mass forward during stance phase in walking. Walking faster requires more powerful muscle contractions to propel the body forward at the end of stance. Infants learn to increase propulsion when they can place their heel down at the end of swing phase and push-off at the end of stance phase. When they start to run a few steps, they demonstrate some difficulty in the control of momentum and may over-run and fall. Figure 11.5 shows the lack of control over horizontal momentum in young children when they stand up from a seat—even when standing up is independent, the child may take a few steps forward instead of standing still (Cahill et al., 1999). Figure 11.5 (A) The infant can stand up independently but takes a step forward to regain balance. He has not mastered the action as, on this attempt, he has not controlled the forward momentum of his body produced in the first phase of the action. (B) Stick figure diagrams taken from videotape of six children with CP aged between 4 and 6 years as they stand up from a height-adjusted stool. Note that although the starting position was standardized, the performance varies with each infant. The diagrams show that several infants had difficulty in achieving an erect standing position and maintaining balance. [(A) From Cahill et al. (1999) Intersegmental co-ordination in sit-to-stand: an age cross-sectional study. Physiother Res Internat 4:12–27, with permission from John Wiley and Sons. (B) From McDonald C 1994 A biomechanical analysis of the sit-to-stand movement in children with diplegic cerebral palsy, BAppSc(Hon) thesis, The University of Sydney.] In the following section, keep in mind that lower limb skills almost all require the ability to support the body mass, balance it and move it from one place to another. This section is a brief account of motor development as it relates to the lower limb. More detailed information is provided in references cited and elsewhere (e.g., Bradley and Westcott, 2006; Piek, 2006; Sutherland, 1997). Our current understanding of motor development is now influenced by experimental findings from biomechanical and electromyographical (EMG) studies. For example, as reaching with the upper limb becomes more efficient and effective, a phase plane plot can demonstrate the gradual changes occurring in joint co-ordination (Fig. 11.6A). A comparative study of the lower limbs as skill develops in sit-to-stand in different age groups is likely to show similar changes occurring over time, reflecting increasing co-ordination of limb segments as the action becomes more skilled (Fig. 11.6B). Studies of kinetics and kinematics illustrate the development of balance control in infants and young children (Roncesvalles et al., 2001), although investigation is typically confined to the infant’s response to unexpected support surface movement. Several biomechanical studies have reported the changes as gait matures around 5 years of age (Fossberg, 1985; Sutherland, 1997, 2001, 2002; Sutherland et al., 1980; Whitall et al., 1985), and the data show the stages through which an infant passes en route to skilled performance. Many of the changes taking place are similar to those found in adults as they learn a novel skill: for example, improved balance, smooth co-ordination, increased speed, decreased energy expenditure, increased effectiveness. Sutherland (1997) has noted that ‘we must understand the natural history of immature walking in order to define and interpret pathological gait in young children’ (p. 163). Figure 11.6 (A) Kinematic profiles of prehension at the age of 4, 7 and 12 years. Linear velocity of the hand was plotted against grip aperture in three children, one from each age group, as they reached to pick up an object. Six trials are superimposed for each subject. By the age of 12 years, reaching and opening the hand to grasp is well co-ordinated and the movement of the hand through space is smooth with no deviations. (B) A velocity–displacement phase plane plot of trunk (i.e., hip) flexion/extension in standing up in an infant from the youngest group (Group 1) shows typical deviations (interruptions and reversals) indicating lack of ability to co-ordinate a smooth transition from hip flexion to hip extension around thighs-off. Compare this to the plot of an older child in Group 2. (C) A representative trial of standing up showing vertical ground reaction forces produced by a child from Group 1 and another from Group 3. The older children (Group 3) showed the distinctive peak around thighs-off similar to adult performance (i.e., skilled), while the younger showed many fluctuations with no distinctive peak. [(A) From Kuhtz-Buschbeck JP et al. (1998) Development of prehension movements in children: a kinematic study Exp Brain Res 122:424–432, with permission from Springer Science+Business Media.] [(B,C) From Cahill et al. (1999) Intersegmental co-ordination in sit-to-stand: an age cross-sectional study. Physiother Res Internat 4:12–27, with permission from John Wiley and Sons.] The basic motor pattern of lower limb movement referred to earlier is seen in utero, where infants practice flexion and extension of lower limbs, kicking and pushing their feet against the uterine wall (Milani-Comparetti, 1980). After birth they retain this ability to flex and extend their legs. The most obvious active movement of lower limbs in the first months in infancy is kicking in various forms. However, when held in standing, full-term newborn infants can also support the body mass through the feet, flex and extend the lower limbs, and take steps, although the way they do this seems to depend on opportunities provided. Most infants can take a few steps on a treadmill if supported (see Fig. 11.10). Early stepping used to be considered a reflexive movement that would disappear, to be followed later by ‘true’ walking. However, Zelazo et al. (1983) found that, with practice and experience of walking, infants retained their ability to take steps and their walking improved. Thelen and Cooke (1987) suggested that this ability to walk after a period of ‘practice’ was due to increased lower limb strength. Evidence also comes from cross-cultural child-rearing studies that advanced walking skill is evident in those societies that give infants the opportunity to walk (see Chapter 1). Infants continue to experiment with lower limb movement when held upright, sometimes kicking, or flexing and extending hips and knees. Held in standing with feet on a supporting surface they bend and straighten their legs, ‘practicing’ the basic pattern of intersegmental co-ordination (flexion and extension at hips, knees, ankles) that they will need in many actions significant to daily life (see Annotation A, Fig. A.6). In raising and lowering the body mass over the supporting lower limbs, they gradually gain control until the limb segments can act together as a single functional unit, seen most clearly in standing up from crouch and from a seat. With the foot on the floor, foot, shank and thigh make up the segmental linkage, movement at one joint, by necessity, producing movement of the other joints (see Figs 1.3A, 1.10a, A.9, and A.6). As learning progresses, the motor control system appears to use simplifying strategies to ‘manage’ this segmental linkage, with co-operation between muscle forces produced over the three joints, varying according to the task and the conditions under which it is performed. Variability is a driving force of developmental change, evident in motor development and acquisition of skill throughout life (Dusing and Harbourne, 2010; Fetters, 1991; Hadders-Algra, 2002). Infants gradually co-ordinate the joints of their lower limbs and develop skilfull performance by repetitive but variable practice (Bernstein’s ‘repetition without repetition’), driven by curiosity and by the opportunities offered by the environment. Although this chapter is focused on the lower limbs, they do not function in isolation from the rest of the body. In the first few months, infants develop the ability to raise their head in supine and prone and to support the head when picked up. The arms reach out to explore the surroundings and arm and leg movements enable the infant to move about in prone and roll over (Fig. 11.2B, C). A major input to gaining control of head, trunk and limbs is vision: infants are driven to move by what they see around them, and with these exploratory movements they begin to develop and fine-tune an integrated movement system involving body, limbs and head. Co-ordination patterns of lower limbs in healthy infants are characterized by a coupling among hip, knee and ankle joints in which all joints tend to flex or extend in temporal synchrony (Thelen, 1985). These typically tight couplings change as the infant practices different joint combinations and a ‘decoupling’ begins as the infant investigates the possibilities during the first few months (Angulo-Kinzler et al., 2002; Jensen et al., 1994). Since infants before birth practice flexion and extension movements, it is likely that even in the first few weeks of life leg movements are not merely random but also exploratory. It is evident that infants can learn to move their legs to achieve a goal (Thelen, 1994). In early movements and attempts at movement the infant seems to be learning what is possible (see Annotation C). Chen et al. (2002) tested the hypothesis that 4-month-old infants can learn a kicking task that involved interacting with a mobile. The authors noted that ‘infants are capable of shifting the patterns they generate to bring back the responses they want.’ (p. 215). Such devices provide examples of how young infants can learn to fine-tune their lower limb (kicking) movements to achieve a goal. They enable the infant to practice independently. The pattern of kicking movements, particularly their variability, can provide early information about disordered motor control (Jeng et al., 2002). For example, any abnormalities in kicking co-ordination in young infants are observable during general movements testing (Chapter 8). Kinematic analysis of movement patterns enables kicking deficits to be detected as early as 1 month of age in premature low birth weight infants with white matter disorder (Fetters et al., 2004). The information gained from such testing of motor performance should lead to an earlier referral to remedial activity programmes. The most critical feature of motor development is the ability to balance the body when moving (e.g., reaching out) in sitting or standing. Some degree of standing balance is generally considered a necessary precursor to locomotor skills (Roncesvalles et al., 2001), but it also underpins virtually all our activities. The development of balance has been investigated in many studies utilizing a movable platform (Brogren et al., 1996; Forssberg and Nashner, 1982; Hirschfeld, 1992; Shumway-Cook and Woollacott, 1985). There has been less investigation of balance mechanisms during other actions. The perturbation studies have demonstrated the muscle activity, joint movements and shifts in CoM (i.e., postural adjustments) under conditions when the child’s balance was unexpectedly perturbed, but they give us no information about the complexity of anticipatory or preparatory and ongoing adjustments as the child balances during self-initiated movements. Studies of balance in adults, however, have examined actions such as reaching in sitting and standing (Eng et al., 1992; Dean and Shepherd, 1997) and raising one leg to take a step (Kirker et al., 2000). Such studies provide information that can assist exercise planning (Carr and Shepherd, 2003, 2010). Even simple actions like turning the head in standing are characterized by oscillations in the line of gravity that are countered by muscle activity and small, barely detectable movements, usually at ankles and hips (Bouisset and Duchenne, 1994). Several studies of the role of vision in balancing the body were carried out with children during the 1970s and 1980s (Butterworth, 1986; Butterworth and Hicks, 1977; Lee and Aronson, 1974) showing that vision has a dominant proprioceptive function in developing children as it does in adults. Vision provides critical environmental and positional guidance for the control of all actions, including gait (see Chapter 10). Learning to judge and predict aspects of the environment, such as verticality and horizontality, provides visual cues about where we are in space, and these abilities probably depend on our experience during our own self-initiated movements in the upright position. There have been few biomechanical investigations of the actions of infants as they learn to gain control over their movements in the first year. However, for an understanding of the mechanisms of balance adjustments (muscle contractions and joint movements) as we move about in sitting and standing we need to know the critical biomechanical features, i.e., movements of the body’s CoG within the periphery of the base of support, kinematic and kinetic details of joint movements. Kinematic details give us joint angular displacements, linear movement of the limbs through space, and the overall topology of the movement. Kinetic analyses, i.e., estimating the forces responsible for an observed movement, yield variables that describe the cause of motion. Vertical and horizontal ground reaction forces, tested with a force plate, demonstrate the movements made in order to maintain an imaginary vertical line drawn from the CoG to the ground to remain within the base of support (Winter, 2009) (Fig. 11.7). From electromyographic studies we see the variability of muscle activity underlying a smoothly co-ordinated and skilled action. Getting to the feet independently and without relying on hand use is one of the most significant and physically demanding abilities developed by infants. Although infants get into standing by pulling themselves up from crouch or half-kneeling, gaining the ability to sit independently on a seat, using the lower limbs for support and balance, provides the opportunity to practice standing up without using the hands. Independent sit-to-stand and squat-to-stand are essential to the early practice of independent walking. One of the most difficult mechanical problems to be mastered by infants learning to stand up is the ability to control the destabilizing forces caused by joint movement, particularly the horizontal momentum of the body’s CoM that is generated by rapid movement of the upper body forward over the feet (Fig. 11.5). Angular momentum is created as the erect upper body rotates forward by flexion at the hips. Flexion of the hip changes to extension when the CoG is over the feet and the body mass is propelled vertically into standing. The muscular effort involved in raising the body mass against gravity is minimized in skilled performers by certain strategies. The feet are moved back (Fig. 11.8A), downward and backward pressure is exerted through the feet, as the upper body flexes forward at the hips bringing the weight forward over the feet as a single smooth movement, an example of a linked segment system in action (Fig. 11.8). The speed of this forward movement of the body mass at the hips and ankles creates horizontal momentum of the body mass. The movement forward is accompanied by active ankle dorsiflexion and vertical pressure downward that stabilizes and holds the shanks forward (dorsiflexed) at the ankles. Calf muscles, hip and knee extensors extend the lower limbs (at ankles, knees, hips) and move the body vertically over the feet and into standing. Fig. 11.8D illustrates the order of muscle onsets during the standing up action (Khemlani et al., 1998). The result is a smooth continuous movement, although one of the most physically demanding of the actions we commonly perform. Figure 11.8 (A) Moving the feet back to approximately 75° of ankle plantarflexion decreases the distance the body’s centre of mass has to move over the new base of support (the feet) and decreases extensor force generation. Foot position seems to be a major determinant of energy expenditure in sit-to-stand. (B) A simplified illustration to show the major kinematic features of sit-to-stand in the sagittal plane. (C) Stick figure drawings taken from a biomechanical study of standing up and sitting down showing the topology (shape) of the movement taken from joint displacement data. The young adult subject shows little difference in the topology of standing up compared to sitting down but some differences in joint movement in the eccentric sitting down phase compared to standing up against gravity (concentric). (D) Mean and standard error of time-normalized onsets and durations of six lower limb muscles as able-bodied adults stand up at their preferred speed. TA, tibialis anterior; RF, rectus femoris; BF, biceps femoris; VL, vastus lateralis; GAST, gastrocnemius; SOL, soleus. Percentage of total movement: 0%, movement onset; 31%, thighs-off; 100%, movement end. [(A–C) From Carr and Shepherd, 2010 Neurological Rehabilitation. Optimizing Motor Performance, with permission from Elsevier. (D) Adapted from Khemlani M, Carr JH, Crosbie WJ et al. (1998) Muscle synergies and joint linkages in sit-to-stand under two different initial foot positions.Clin Biomech 14:236–246, with permission from Elsevier.] Sitting down appears to be the reverse action to standing up, but there are significant differences that make it particularly difficult for an infant. There are different mechanical constraints as the movement is performed by gravity and controlled by eccentric (lengthening) contractions of the lower limb extensor muscles that slow the descent of the body mass. The limbs flex and, just before the seat is reached, flexion of the trunk at the hips increases and the body mass, moving at the ankles, shifts backward, with the tibialis anterior muscle contracting strongly (Carr and Shepherd, 2010). This is a destabilizing movement, and the balance, muscle and mechanical constraints are considerable. Even when the infant can sit down, he finds it difficult to initiate the descent. There appear to be few investigations of the stages an able-bodied infant goes through in the first year to learn these two actions or of the mechanical differences between an able-bodied infant and an infant with CP (da Costa et al., 2010). Nevertheless, biomechanical analysis can document clearly the mechanical reasons for poor performance in children with CP compared to able-bodied children (dos Santos et al., 2011; Park et al., 2003; Yonetsu et al., 2009;). A study of standing up (Cahill et al., 1999) involved 18 able-bodied children between the ages of 12 months and 10 years, six in each of three age groups (12–18 months, 4–5 years, 9–10 years). They wore reflective markers and were videotaped as they stood up from a height-adjustable seat that straddled a force plate (see Fig. 11.5A). Cahill and colleagues found infants as young as 13 months could stand up using a similar basic motor pattern to that of adults. However, although the younger children could stand up independently, they appeared to have difficulty understanding the idea of standing up as an end in itself. The authors commented that the children seemed unable to end the movement in quiet standing but either took a few steps forward or went up on their toes, depending on whether vertical or horizontal momentum was the more destabilizing. Older children showed less variability in performance than the younger children (Fig. 11.6B,C). By 4 years of age, children could flex the hips and rotate the upper body further forward and faster, and could end the action in quiet standing. Developmental trends were evident on the videotapes and in the kinetic and kinematic variables. Movement time, amplitude and peak angular velocity of hip flexion increased with age. Children in the older groups displayed a pattern of ground reaction forces similar to those reported for adults. The youngest reached peak force more slowly, often with fluctuations. Phase plane plots showed the co-ordination of the movement increasing with age and skill level (Fig. 11.6B). The authors suggested that differences in intersegmental co-ordination as the action developed may reflect the child’s increasing ability to control horizontal momentum and to balance. The results are of particular interest since they illustrate the changes taking place in a complex action as the infant/child develops skill after learning the basic motor pattern: feet back → push down through feet+flex trunk forward at hips → extend hips, knees, ankles → stand still. Gaining the ability to time joint movements, control muscle forces and balance the body mass throughout the action and from a variety of different seats required a great deal of practice. Data from another study of children 4- to 6-year-old children with diplegia also showed that they often overbalanced forward as they rose to standing (Fig. 11.5B). In addition, in most trials the children had difficulty producing peak vertical force at thighs-off, which suggests that both generating and timing lower limb extensor muscles forces were difficult (Shepherd and McDonald, 1995). More recently, Park et al. (2003) found increased hip flexion and slowness of movement, with decreased peak knee extensor moment of force and decreased extensor power generation at hips and knees in a group of children with hemiplegia or diplegia. Transitional quadripedal locomotion on hands and knees or hands and feet, such as crawling, creeping and bear walking (Fig. 1.10B), enables the infant to get about on the floor in the first year, before the muscles are strong enough and attempts at bipedal locomotion are sufficiently balanced for the infant to be independent in standing up and walking. These quadripedal actions may have a significant effect on the development of overall limb co-ordination, linking the upper and lower limbs in ways that may potentiate a child’s performance of any actions that involve interactions between all four limbs. Which method the infant prefers seems arbitrary but probably depends on the ground surface available, how often he/she is placed on the ground, and what possibilities the environment offers (Chapman, 2002; Groenen et al., 2010). Not all infants crawl, and there is evidence from studies of child-rearing practices that suggests that an infant’s preferred early locomotion depends on opportunity (Wong, 2009). Infants who are placed on the floor and who have developed the ability to push themselves up on their arms may pull themselves along the floor (Fig. 11.2B). The infant may then get on to hands and knees, rock to and fro (Fig. 11.2A), and crawl. Some children ‘bear walk’ on hands and feet before they get to their feet and start cruising around the furniture (Fig. 11.9B). There is considerable variability and the action selected seems to depend on opportunity and practice. Figure 11.9 (A) Half crawl–half bear walk. (B) Walking sideways, probably critical for controlling hip movement in walking. It enables practice of balancing on the feet. One of the few biomechanical studies of crawling (Freedland and Bertenthal, 1994) has described acquisition of a diagonal crawling pattern around 33 and 45 weeks. Variability of timing and some instability are observed at first, and once stability of performance is achieved the infant increases speed. The findings confirm the current view that, rather than being the result of neuromaturational processes, it seems likely that crawling is a learned behaviour contingent upon opportunity and being able to get on to the hands and knees. Locomotor-like behaviour and other movements similar to those seen in newborns have been observed in utero by 15 weeks’ post-gestation (de Vries et al., 1982). Thelen and Fisher (1982) showed similarities in newborn infants between the movement pattern seen when kicking in supine and the action of stepping present at birth, but with different mechanical demands. By the time independent walking commences, the infant already demonstrates the basic locomotor pattern learned from the simple stepping pattern present at birth (Thelen, 1986). Young infants, even pre-walkers aged 4 to 12 months, when placed on a treadmill show similar EMG patterns and interlimb co-ordination as appear in adult walking (Bradley and Westcott, 2006; Pang et al., 2003) (Fig. 11.10). Figure 11.10 Walking for infants on infant treadmill: (A) aged 2 months, (B) 4 months and (C) 9 months. [From Groenen A et al. (2010) Constraints on early movement: Tykes, togs, and technology. Infant Behav Dev 16–22, with permission from Elsevier.] As noted above, locomotion in the upright position depends on the development of support (weight-bearing), balance and propulsion of the lower limbs. These are the three basic necessities for over-ground progression (Winter, 1987). The study of the basic biomechanics (kinematics, kinetics) and muscle activity of walking in adults provides a framework for understanding the deviations that occur as infants slowly, over many years, develop skill and learn to vary aspects of walking to fit environmental circumstances and task. Knowing the basic biomechanical characteristics also forms a framework for analysis and intervention for individuals with impairments of the neuromuscular system (Fig. 11.11A,B). Figure 11.11A Upper: position of the R leg in the sagittal plane at 40 ms intervals during a single gait cycle. Lower: sagittal plane hip, knee, ankle joint angles (degrees) during a single gait cycle. IC, initial contact; OT, opposite toe-off; HR, heel rise; OI, opposite initial contact; TO, toe-off; FA, feet adjacent; TV, tibia vertical. [(A) From Whittle MW (2007) Gait analysis: An introduction 4th ed. with permission from Elsevier.] Figure 11.11B Left: averaged horizontal (upper) and vertical (lower) ground reaction forces (GRF). Horizontal GRF has a negative phase in the first half of stance, indicating a slowing down of the body, and a positive phase indicating forward acceleration of the body, during the latter half of stance. Vertical force has the characteristic double hump, the first related to weight-acceptance, the second to push-off. CV, coefficient of variation. Right: ensemble averages of power patterns of able-bodied subjects walking at their preferred cadence plotted over a single gait cycle showing the most important power phases for hip (H), knee (K) and ankle (A); 60% indicates the beginning of swing phase. CV, coefficient of variation. [(B) From Winter DA (1987) The Biomechanics and Motor Control of Human Gait Waterloo Biomechanics.] There have been several descriptions of the kinematics, kinetics and EMG parameters of gait in children with and without CP (Forssberg, 1985). Before walking independently, the infant ‘cruises’ the furniture, walking sideways. This has the advantage of providing practice of one of the critical features of walking, its initiation. For example, prior to lifting the left foot to take a step, pressure downward through this foot shifts the body mass to the right, over the stance leg (Kirker et al., 2000). In other words, a step can be taken only when there has been a shift of the body mass in the frontal plane from the stepping leg to the standing leg, a shift that is initiated by the stepping leg. Early attempts at walking show the strain of balancing the body mass and the effects of poor motor control—the infant takes small flat-footed steps with feet apart to give a wider base of support. As balance in walking improves, the infant carries toys, pushes and pulls trailers, walks on different surfaces, and up and down small steps and inclines, and runs. As infants practice, they develop flexibility of performance. Although walking in varied environments involves the same basic movement pattern (stance phase, swing phase, double stance phase) and similar joint ranges, different environments demand different patterns of muscle force production; for example, the timing of peak forces varies and the type of muscle work differs when walking up and walking down steps and hills (concentric or eccentric; more or less muscle force and energy expenditure). Advanced actions such as jumping (2–3 years), standing on one leg (4 years) and hopping (5 years) take longer before skill is acquired. The dysfunction stemming from impairments (weakness and dyscontrol) and maladaptive changes to muscle (decreased extensibility) associated with CP become more obvious at the transition between dependent and independent walking. An interesting study carried out 20 years ago, using a treadmill, EMG, motion analysis (for kinematics) and foot contact measures, examined gait immediately before and after the acquisition of independent locomotion in children with and without CP. The children’s ages ranged from 9 months to 6 years. The gait pattern of the children with CP was similar initially to that of the able-bodied children. However as walking progressed, they retained some of the characteristics of the infant motor pattern but developed none of the major features of adult gait (dorsiflexion at heel strike, plantarflexion and hip extension at the end of stance phase, with knee flexion mid-stance) (Leonard et al., 1991; see also Berger et al., 1982, 1984; Berger and Adolph, 2007). It is these major characteristics that should be a focus of early exercise. Training should include exercises for lower limb muscles such as calf muscles and hip extensors (see Figs 11.15–11.24) and walking on a treadmill, since the moving belt tends to drive these aspects of gait. The change to a more adult pattern of walking normally begins when the child begins to walk independently and continues until 2–4 years of age (Forssberg, 1992). In the infant with CP, the foot is placed flat or on the toes, with premature activation of the calf muscles. In infants with diplegia or hemiplegia, however, when walking becomes independent, calf and hip flexor muscle contractures, if they have not been prevented, may become more evident, together with decreased hip flexion in swing, increased hip internal rotation and adduction and a hyperextended knee through stance phase (Fig. 11.11C,D). Poor activation of calf muscles, in particular, but also weakness and limited hip and knee extension in stance phase, result in weak or absent propulsive force at the end of stance phase. Figure 11.11C,D The little girl on the left with left hemiplegia demonstrates at mid-stance two mechanical effects of calf muscle (soleus) contracture—hyperextended knee due to decreased dorsiflexion, and limited hip extension. Note also the poor control of hip abduction in left stance phase, i.e., her pelvis drops down to the R when she takes weight through her left leg. (D) The boy on the right with diplegia is at the end of stance phase/start of swing phase (i.e., push-off). He demonstrates the mechanical effects of hip flexion contracture and extensor and abductor muscle weakness—internally rotated and adducted hips, and lack of knee and hip extension through stance phase. These effects are more obvious in the lateral view. [(C,D) From Shepherd (1995) Physiotherapy in Paediatrics, with permission from Elsevier.]
Training lower limb performance in early infancy
Support, balance and propulsion
Introduction
Part 1: support, balance, propulsion
Balance of body mass over base of support
Propulsion of body mass
Development of lower limb motor skills
Kicking
Balancing in sitting and standing
Standing up and sitting down
Sitting down
Crawling
Walking
Related posts:
 Re-thinking the brain: new insights into early experience and brain development
Effects of motor activity on brain and muscle development in cerebral palsy
Functional effects of neural impairments and subsequent adaptations
Early diagnosis and prognosis in cerebral palsy
Treadmill training in early infancy: sensory and motor effects
The changing face of intervention in infants with cerebral palsy
Re-thinking the brain: new insights into early experience and brain development
Effects of motor activity on brain and muscle development in cerebral palsy
Functional effects of neural impairments and subsequent adaptations
Early diagnosis and prognosis in cerebral palsy
Treadmill training in early infancy: sensory and motor effects
The changing face of intervention in infants with cerebral palsy
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Training lower limb performance in early infancy: Support, balance and propulsion

