how the intracranial contents are able to compensate for changes in volume. When compliance is reduced, small changes in volume lead to large changes in ICP. It is important to understand this rightward shift of the pressure-volume index (PVI), (see Fig. 2) because even when ICP is normal, very small changes in volume can have disastrous effects by causing herniation through a rapid increase in ICP.
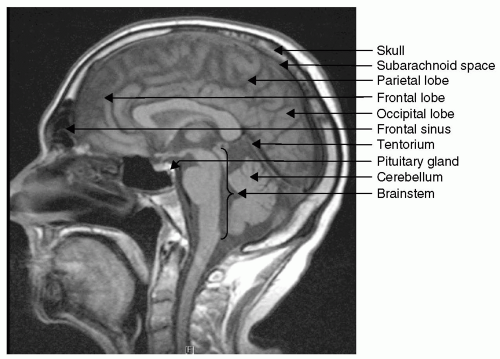 Figure 1 Sagittal magnetic resonance image (T1) of the skull and brain. |
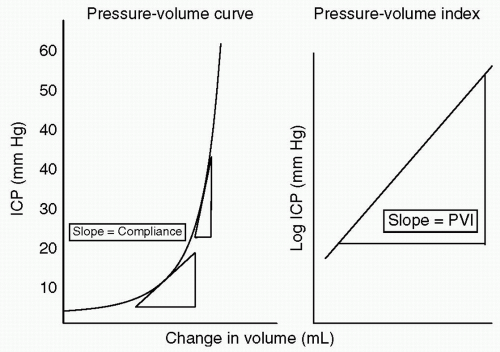 Figure 2 Brain compliance. After any injury, the brain will compensate for increases in pressure through elastance and compliance. As compliance is lost, small changes in volume can lead to large changes in pressure. In a patient who is on the right side of the curve, even with normal intracranial pressure (ICP), small changes in volume can precipitate large rises in pressure. |
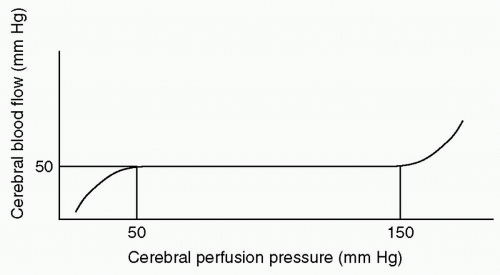 Figure 3 Cerebral autoregulation. |
 Figure 4 Right temporal epidural hematoma (arrow) on head computed tomography (CT). Note its smooth lentiform shape. |
coalesced mass in an ICH on CT scan. Contusions are often found in the frontal and temporal lobes because this tissue “glides” over the underlying rough bony surface of the skull base during impact and acceleration/deceleration of the head (see Fig. 6). The brain may also impact the inner table of the skull across from the area of impact, thereby causing a contusion or hemorrhage. This is known as a coup-contre-coup lesion. ICH may also occur with penetrating injuries (e.g., stab wounds or gun shot wounds, see subsequent text). Finally, ICH may develop or progress ≥24 hours after injury (delayed traumatic ICH) and therefore, patients at risk require careful follow-up and repeat imaging.14,15
 Figure 5 Subdural hematoma (SDH). Acute left temporal parietal subdural hematoma (arrow) and right temporal intraparenchymal contusion (curved arrow). In addition there is blood (subarachnoid) layering on the tentorium and involving the brainstem (large arrow). |
 Figure 6 Intracerebral hemorrhage. Right temporal occipital lobe intracerebral hemorrhage (arrow) with associated vasogenic edema (block arrow). Note the compressed right occipital horn of the lateral ventricle. |
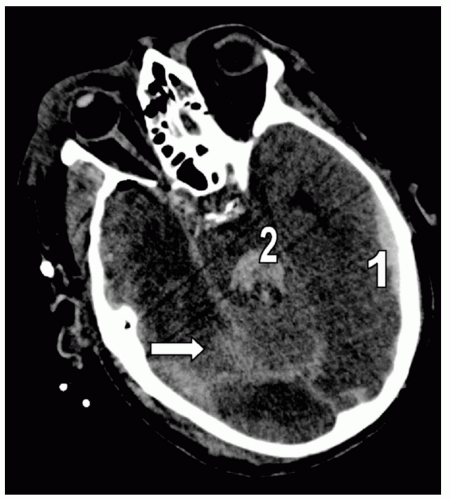 Figure 7 Subarachnoid hemorrhage (SAH). Different detail from the patient in Fig. 5 demonstrating extensive right posterior SAH (arrow). Note the accompanying left temporal subdural hematoma (1) and fourth ventricle blood (2). |
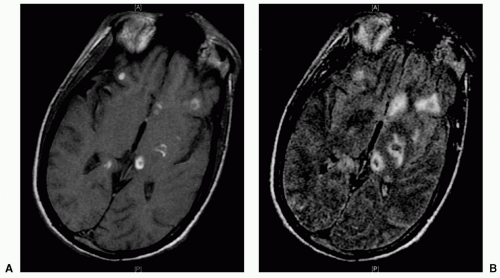 Figure 8 Diffuse axonal injury (DAI). A: T1 magnetic resonance imaging (MRI) demonstrating susceptibility artifact at the gray-white junction of the left thalamus, left internal capsule, right splenium, and corpus callosum. B: Equivalent image on flair MRI. |
before administration of sedatives and/or paralytics. A GCS of ≤8 indicates coma and airway intubation, and ventilation should be considered early. If necessary, an emergency surgical airway (cricothyroidotomy, tracheostomy) may be required.
TABLE 1 GLASGOW COMA SCALE | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 2 CLASSIFICATION OF TRAUMATIC BRAIN INJURY (TBI) | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


