Chapter 4 Acute inflammation: morphology and consequences



Morphological appearance
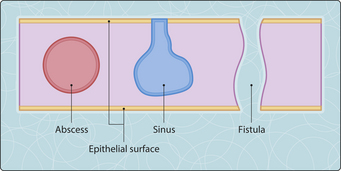
Abscesses, sinuses and fistulae
An abscess (Fig. 3.4.1) is a collection of pus within tissue. If it persists, it becomes walled off by a surrounding rim of granulation tissue. Sometimes, an abscess will spontaneously discharge via the skin or into a body cavity; it is said to ‘point’ as it erodes towards the surface of the tissue. When it has burst and discharged its contents, it may be obliterated by granulation tissue and healing will occur by fibrosis. Alternatively, the route along which the pus was discharged may persist as a sinus tract, which is defined as a connection between the tissue and a surface (epidermal or epithelial); the tract may be lined by granulation tissue and/or by epithelium derived from the surface. For example, osteomyelitis is often complicated by chronic sinuses connecting the infected bone to the surface of the skin, allowing pus from the site of inflammation to drain. Sometimes, an analogous process will produce a fistula, which is an abnormal connection between two epithelial surfaces or an epithelial surface and the skin. For example, a segment of ileum that is inflamed in Crohn’s disease may become adherent to the bladder, and if the inflammation spreads into the bladder wall a tract connecting the ileum and the bladder (an ileovesical fistula) may form. A similar process can produce fistulae between the ileum and another segment of bowel, the vagina or the skin. If a hollow organ (e.g. gallbladder or appendix) or anatomical space (e.g. pleural cavity) fills with pus, the term empyema may be used.
< div class='tao-gold-member'>


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


