Chapter 16 Inappropriate Sinus Tachycardia
Pathophysiology
Sinus tachycardia is a physiological response to sympathetic activation and/or parasympathetic withdrawal, such as during exercise, anxiety, pain, hypovolemia, orthostatic hypotension, fever, infections, hyperthyroidism, hypoglycemia, anemia, myocardial infarction, heart failure, pericarditis, diabetes-related autonomic dysfunction, drug abuse, catecholamine infusions, anticholinergic drugs, tobacco, caffeine, alcohol, and beta-blocking agent withdrawal. Inappropriate sinus tachycardia (IST) is a nonparoxysmal tachyarrhythmia characterized by a persistent increase in resting sinus rate unrelated to, or out of proportion with, the level of physical, emotional, pathological, or pharmacological stress or an exaggerated heart rate response to minimal exertion or a change in body posture.1 IST is neither a response to a pathological process (e.g., heart failure, hyperthyroidism, or drug effects) nor a result of physical deconditioning.
The underlying mechanism of IST remains poorly understood. Several potential mechanisms have been suggested, including enhanced automaticity of the sinus node, altered sinus nodal intrinsic regulation, disorder of autonomic responsiveness of the sinus node, and sympathovagal imbalance, with excessive sympathetic drive or reduced vagal influence on the sinus node, or both. A primary abnormality of sinus node function has been suggested, as evidenced by a higher intrinsic heart rate (after muscarinic and beta-receptor blockade) than that found in normal controls or a blunted response to adenosine with less sinus cycle length prolongation than in control subjects (with and without autonomic blockade).2,3 In addition, beta-adrenergic receptor hypersensitivity, alpha-adrenergic receptor hyposensitivity, M2 muscarinic receptor abnormalities, brain stem dysregulation, depressed efferent cardiovagal reflex, and impaired baroreflex control are likely explanations. Chronic beta-receptor stimulation by autoantibodies and autonomic neuritis or autonomic neuropathy can play a role in some cases. The extent to which each of these mechanisms contributes to tachycardia and associated symptoms is unknown, but the underlying mechanisms are likely multifactorial and complex.4–7
In some patients, there can be an overlap between IST and disorders such as chronic fatigue syndrome and neurocardiogenic syncope, and other patients can have a psychological component of hypersensitivity to somatic input.8 Other groups with similar or overlapping laboratory findings and clinical course include patients with hyperadrenergic syndrome, idiopathic hypovolemia,9 orthostatic hypotension, and mitral valve prolapse syndrome.2,3
Clinical Considerations
Epidemiology
Almost all patients afflicted with IST are young women (mean age, 38 ± 12 years), and many of them are hypertensive. IST affects people working in health care in disproportionate numbers. The explanation for these findings is lacking.3,10 The prevalence of IST in a middle-aged population (up to 1.16% in one report) appears to be higher than previously assumed. Despite the chronic nature of the disorder and long-lasting symptoms, the natural course and prognosis of IST are benign.10
Clinical Presentation
The most prominent symptoms are palpitations, fatigue, and exercise intolerance. IST can also be associated with a host of other symptoms, including chest pain, dyspnea, lightheadedness, dizziness, presyncope, and syncope. The clinical presentation of the arrhythmia is highly variable, ranging from totally asymptomatic patients identified during routine medical examination to those with paroxysmal short episodes of palpitations to individuals with chronic, incessant, and incapacitating symptoms.2,10 The risk of tachycardia-induced cardiomyopathy in untreated patients is unknown but is likely to be low.1,10,11
Initial Evaluation
IST is an ill-defined clinical syndrome with diverse clinical manifestations. There is no gold standard to make a definitive diagnosis of IST, and the diagnosis remains a clinical one after exclusion of other causes of symptomatic tachycardia. Clinical examination and routine investigations allow elimination of secondary causes for the tachycardia but are generally not helpful in establishing the diagnosis of IST.1–3
The syndrome of IST is characterized by the following: (1) a relative or absolute increase in sinus rate out of proportion to the physiological demand (there can be an increased resting sinus rate of more than 100 beats/min or an exaggerated heart rate response to minimal exertion or change in body posture); (2) P wave axis and morphology during tachycardia that are similar or identical to those noted during normal sinus rhythm; (3) lack of secondary causes of sinus tachycardia; and (4) markedly distressing symptoms of palpitations, fatigue, dyspnea, and anxiety during tachycardia, with an absence of symptoms during normal sinus rates.1–412
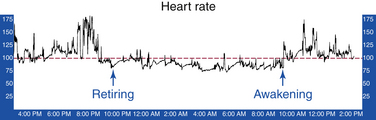
Ambulatory Holter recordings characteristically demonstrate a mean heart rate of more than 90 to 95 beats/min (Fig. 16-1). However, some patients have either a physiological or normal heart rate at rest (less than 85 beats/min) with an inappropriate tachycardia response to a minimal physiological challenge or a moderately elevated resting heart rate (more than 85 beats/min) with an accentuated (inappropriate) heart rate response to minimal exertion.2,3,13 However, this quantitative definition of inappropriate is arbitrary, and validation of the reproducibility of the heart rate and activity correlation can be challenging.12,14
Exercise ECG testing typically shows an early and excessive increase of heart rate in response to minimal exercise (heart rate greater than 130 beats/min within 90 seconds of exercise; Bruce protocol). This heart rate response is differentiated from physical deconditioning by chronicity and the presence of associated symptoms.2
Isoproterenol provocation helps demonstrate sinus node hypersensitivity to beta-adrenergic stimulation. Isoproterenol is administered as escalating intravenous boluses at 1-minute intervals, starting at 0.25 µg, with doubling of the dose every minute, until a target heart rate increase of 35 beats/min higher than baseline or a maximum heart rate of 150 beats/min is reached. In patients with IST, the target heart rate is reached with an isoproterenol dose of 0.29 ± 0.1 µg (versus 1.27 ± 0.4 µg in normal controls).2
Invasive electrophysiological (EP) testing may be considered when other arrhythmias are suspected or when a decision to proceed with catheter ablation is undertaken. It is important to recognize that sinus node modification to target IST is a clinical decision, and it must be made prior to the invasive EP study itself. The diagnosis of IST and the treatment approach have to be established before the patient is brought to the EP laboratory.2,3
IST shares several characteristics with postural orthostatic tachycardia syndrome (POTS), and it is sometimes challenging to differentiate between the two conditions. POTS is characterized by the presence of symptoms of orthostatic intolerance (i.e., the provocation of symptoms on standing that are relieved by recumbence) associated with a heart rate increase of 30 beats/min (or a rate that exceeds 120 beats/min) that occurs within the first 10 minutes of standing or upright tilt and is not associated with other chronic debilitating conditions such as prolonged bed rest or the use of medications known to diminish vascular or autonomic tone. Patients with POTS tend to display a more pronounced degree of postural change in heart rate than do those with IST. Additionally, in the supine position, the heart rate in patients with POTS rarely exceeds 100 beats/min, whereas in IST the resting heart rate is often higher than 100 beats/min. Patients with IST do not display the same degree of postural change in norepinephrine levels as do patients with hyperadrenergic POTS. The distinction between IST and POTS is important because catheter ablation of the sinus node rarely improves, and can even worsen, symptoms in patients with POTS.15
Principles of Management
The treatment of IST is predominantly symptom driven. Medical management remains the mainstay of therapy. Beta-blockers can be useful and should be prescribed as first-line therapy for most patients. Nondihydropyridine calcium channel blockers (verapamil and diltiazem) can also be effective.1 However, pharmacological therapy for IST has been limited by the poor long-term tolerance to the drugs and the disappointing long-term outcome.
Ivabradine is a novel selective inhibitor of cardiac pacemaker If ion current, which is highly expressed in the sinus node and contributes to sinus node automaticity. Ivabradine selectivity induces heart rate reduction in humans and animals without any modification in cardiac contractility and atrioventricular and intraventricular conduction times. Blockade of the If current induced by ivabradine is dose and heart rate dependent, resulting in greater effects during fast heart rates and limiting the risk of symptomatic bradycardia. This agent is commonly used to relieve pain in patients affected by chronic stable angina. Preliminary data suggest that orally administered ivabradine lowers the mean daily and maximal heart rates in patients with IST, improves symptoms, enhances exercise-stress tolerance, and markedly improves quality of life, even in patients refractory to beta-blocking therapy. This pharmacological treatment could be considered a second-line therapy in patients refractory to and intolerant of beta-blockers and nondihydropyridine calcium channel blockers. However, more large-cohort studies are needed to confirm these preliminary results.11,16,17
Despite advances in ablation technologies, the long-term success of catheter ablation for IST remains disappointing. Nevertheless, sinus node modification by catheter ablation remains a potentially important therapeutic option in the most refractory cases of IST.1,2
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


