Fig. 14.1
Images in patient with calcific tendinitis. X-ray (left) and 3D CT (right)
14.2.5 Shoulder Stiffness Associated with Osteoarthritis
Osteoarthritis around the shoulder girdle restricts shoulder motion, and the degree of restriction normally depends on severity of osteoarthritis. In shoulders with glenohumeral osteoarthritis, shoulder motion is mechanically restricted due to capsular fibrosis and to excessive osteophytes and malcongruity of the joint, which is very easily detected by X-rays (Fig. 14.2). Rotator cuff is normally well preserved in primary osteoarthritis on MRI. In shoulders with osteoarthritis in the acromioclavicular joint, forward flexion is often restricted due to less mobility and pain at the joint. In these shoulders, external rotation and internal rotation are normally well preserved (Fig. 14.3).

Fig. 14.2
Images in patient with primary glenohumeral osteoarthritis. X-ray (left) and an axial image of CT (right)
Fig. 14.3
X-ray image in patient with primary osteoarthritis in the acromioclavicular joint
14.2.6 Shoulder Stiffness in Full-Thickness Rotator Cuff Tears
Shoulder stiffness is frequently associated in patients with symptomatic rotator cuff tears. Recently, Iwamoto and coworkers reported characteristics of shoulder stiffness in patients with full-thickness rotator cuff tears in a Japanese journal [26]. They investigated patterns and prevalence of shoulder stiffness in 155 patients with unilateral symptomatic full-thickness rotator cuff tear who underwent surgery and compared with 20 patients who underwent arthroscopic pancapsular release for refractory stiff shoulder during the same period. In this article, 89 % of 155 shoulders with full-thickness rotator cuff tears demonstrated passive range of motion deficit in at least one of the following motions which includes forward flexion (FF), external rotation at side (ER), and internal rotation (IR) preoperatively. Among them, unidirectional motion restriction was seen in 41 shoulders (26.5 %) and bidirectional restriction observed in 48 shoulders (31.0 %). The rest of 49 shoulders (31.6 %) demonstrated global motion restriction (Fig. 14.4). On the other hand, all 20 refractory stiff shoulders who underwent capsular release demonstrated severe and global loss of motion, which was less than 100° in FF, 10° in ER, and less than L5 in IR. However, none of the 49 shoulders (31.6 %) with full-thickness rotator cuff tears who demonstrated global motion loss did not meet above criteria (severe and global motion loss). Therefore, they concluded that range of motion deficit in patients with full-thickness rotator cuff tears was relatively mild compared with that in refractory stiff shoulders which requires pancapsular release.
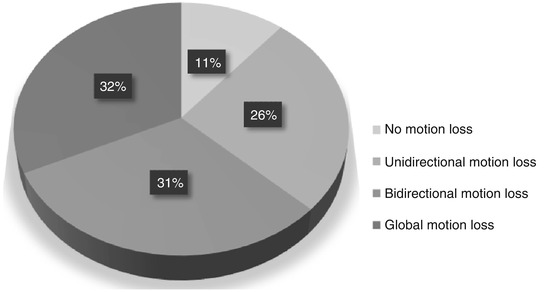
Fig. 14.4
Patterns and prevalence of range of motion loss in shoulders with full-thickness rotator cuff tears. Eighty-nine percent of shoulders demonstrated passive range of motion deficit at least one of the following motion: forward flexion, external rotation at side, and internal rotation preoperatively. Twenty-six percent of shoulders demonstrated unidirectional, 31 % demonstrated bidirectional, and 32 % demonstrated global motion restriction. However, none of the 49 shoulders who had global motion loss demonstrated severe and global loss of motion
14.3 Imaging of Frozen Shoulders or Adhesive Capsulitis
It has been believed that rotator cuff disease and adhesive capsulitis can typically be distinguished based on a careful history and physical examination [27]. However, since the recent progress of diagnostic imaging revealed high prevalence of rotator cuff lesions in frozen shoulders, several articles reported that the rotator cuff lesions are strongly associated with frozen shoulders or idiopathic adhesive capsulitis [6, 28–30]. Although these conditions may be present concomitantly, it is less likely for patients with idiopathic adhesive capsulitis to have rotator cuff pathology.
Loeffler and colleagues retrospectively reviewed the medical records of 38 consecutive patients who underwent arthroscopic capsular release for adhesive capsulitis [31]. A preoperative MRI diagnosis was compared to the actual status of the rotator cuff during surgery. Although preoperative MRI interpretations predicted an incidence of rotator cuff tears of 57.9 %, operative findings revealed a true incidence of rotator cuff pathology of only 13.2 % (P < .0001). They concluded that MRI interpretations in patients with adhesive capsulitis may provide misleading information with a high percentage of false-positive reports of rotator cuff tears [31].
In a very recent study, Ueda and colleagues have investigated rotator cuff lesions in frozen shoulders with global and severe motion loss using a large cohort of patients [32]. A consecutive series of 379 stiff shoulders, in which patients with evident secondary stiff shoulders were excluded, was prospectively investigated using MRI or ultrasonography. Among them, 89 shoulders demonstrated severe and global loss of passive motion based on the criteria in the previous literature [26]. In these shoulders, only 9 % showed a partial-thickness cuff tear; in 91 % an intact rotator cuff was seen. Interestingly, none of the patients demonstrated full-thickness rotator cuff tears.
In this manuscript, they also insisted of importance of ROM measurement methods since many patients complain pain during measurement. Therefore, they recommend to measure external rotation with the patient in the supine position in order to diminish the effect of pain, in addition to standard measurement with the patients in the standing or sitting position [32].
Case Presentations
Following are the examples showing how the pain, range of motion, and position of the body are intimately related.
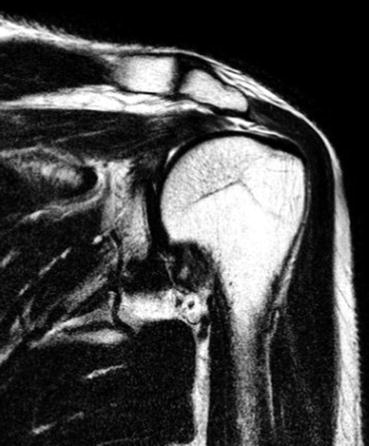
Case 1. A 51-year-old female presented to our institute with left shoulder pain and range of motion deficit. Her external rotation with the arm at the side was −5° in the standing position and 0° in the supine position, with similar pain in both positions. MRI demonstrated intact rotator cuff (Fig. 14.5).

Fig. 14.5
MRI on the left shoulder in a 51-year-old female. T2-weighted coronal image demonstrates intact rotator cuff
Case 2. A 55-year-old male complained of left shoulder pain and limited range of motion. His external rotation at the side in the standing position was 10° with pain, whereas it increased up to 50° in the supine position where he felt much less pain. MRI demonstrated a full-thickness rotator cuff tear (Fig. 14.6).