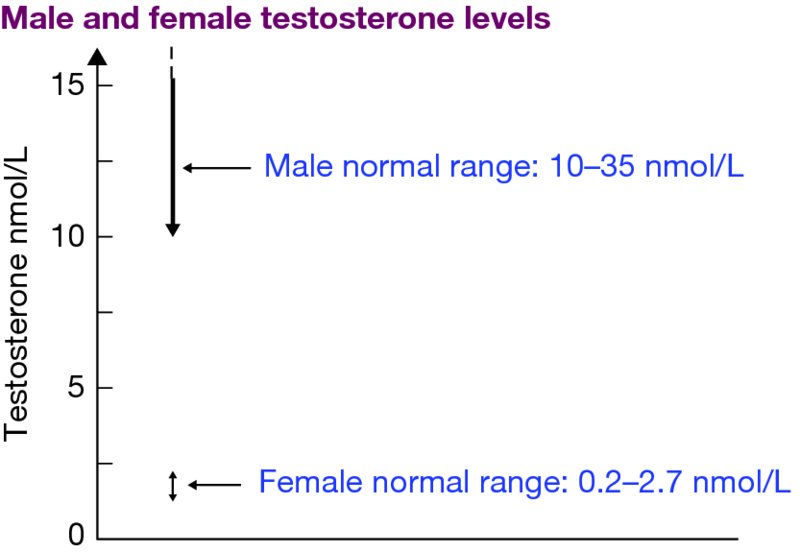
Chapter 10 Martin Ritzén Department of Women’s and Children’s Health, Karolinska Institutet, Stockholm, Sweden In almost all sports, the athletes are divided into two categories: male and female. Early on, this categorization may have had its roots in the belief that women were too fragile to expose themselves to heavy exercise. Women were therefore forbidden to take part in very strenuous activities. For example, the very popular 90-km Swedish ski race “Vasaloppet” was until 1981 out of bounds for women, in spite of protests from able women skiers. A TV interview of a competitor at that time revealed that the moustache-carrying competitor was a woman, masquerading as a male! She did so well in the race that the organizers later were forced to accept women as unofficial participants. Not until 1997 were the women fully accepted. They now ski together with the men, but the results are listed separately. Today, almost all sports arrange competitions for both men and women—but always in separate categories. Horseback events seem to be the exception. Why are the two sexes separated in all other sports? The simple answer is that the average man is stronger and faster than the average woman. This is true also at the highest elite level, where both men and women are professionals and undergo strenuous full-time training to get to the top. This is obvious for the true strength-dependent events (weight lifting, boxing, etc.) but also in running; the world records are about 10% better in the male than the female category, and none of the female medallists in 2013 Athletic World Championships would have ended up among the top athletes in the male events (Table 10.1). Therefore, women in general do not want to compete against men, which necessitates rules and regulations on who is qualified to compete as a woman. Table 10.1 Results from World Championships in Athletics, Moscow 2013. The winning woman would not have been better than number 32 in any of these events if she had competed in the men’s qualification heats (100–1500 m) or finals (10 000 m and marathon) Men are on average about 13 cm taller than women, which gives them an advantage in many sports. But there is a major overlap between the sexes; the mean height of Swedish men is 181 cm, but the 95% confidence limits are wide (169–193 cm). Similarly, the variation around the mean height of young women (167 cm in Sweden) is between 155 and 179 cm. It has long been accepted that anabolic/androgenic hormones can enhance physical performance. Therefore, heavy penalties are cast on those athletes, male and female, that cheat by doping themselves with such hormones. The natural difference in testosterone levels in blood of men and women is the most decisive factor that during and after puberty makes the average man to build much more muscles than the average woman. And in the case of testosterone, there is no overlap between healthy men and women (Figure 10.1). This nonoverlap is unique—no other hormone or other known factors are so discriminating between the two sexes. However, during and immediately after heavy exercise, testosterone levels increase somewhat in women and decreases in men. Figure 10.1 Illustration of levels of testosterone in the blood of healthy men and women. The exact values may vary a little, depending on the laboratory and the methods used. Under resting conditions, there is no overlap between the sexes. Both men and women have both male and female sex hormones, although the normal levels are widely different. Estrogens are necessary for skeletal health in both sexes—a complete deficiency of estrogenic hormones or insensitivity to them results in severe osteoporosis also in men. Furthermore, such rare men never cease growing! Similarly, small amounts of androgens from adrenals and ovaries are present in the blood of healthy women (Figure 10.1), although an androgen deficiency in women does not manifest itself by severe symptoms. For women, a major increase in testosterone levels in blood will lead to more or less pronounced virilization, with increased hair growth over the pubic, axillary and facial areas, acne, male sweat odour, deepening of the voice, increased clitoral size, and increased muscle volume and strength. This condition with increased levels of testosterone in blood is called hyperandrogenism, which can be caused not only by a number of inborn errors in the metabolism of steroid hormones, but also by acquired diseases later in life. However, the tissues must also be able to respond to the androgens to elicit a response. In rare instances, this response is diminished or absent; the individual has the so-called “Complete or Partial Androgen Insensitivity Syndrome (CAIS or PAIS),” and consequently little or no benefit from the elevated testosterone levels. All de novo steroid hormone synthesis occurs in either the adrenals or the gonads (ovaries and testes). Thus, diseases that affect these organs sometimes results in increased production of testosterone, in both women and men. Such diseases may be acquired in postnatal life (steroid-producing tumours, abnormal regulation of steroid synthesis as in polycystic ovary syndrome, PCOS), or they may be due to inborn errors of steroid hormone synthesis or metabolism. Examples of such disorders are listed in Table 10.2. If the sensitivity to androgens is normal, the increased testosterone levels will lead to virilization of women and as a result of that, increased muscle mass and an advantage in sport when competing against other women. Table 10.2 Some benign conditions that lead to hyperandrogenism in women
Hyperandrogenism and gender change
Introduction
Event
Winning man
Winning woman
Best woman among men’s qualification
Percent difference best man/woman
100 m
9.77 sec
10.71 sec
56
9
400 m
43.74 sec
49.41 sec
32
11
1500 m
3.36 min
4.02 min
35
11
10 000 m
27.21 min
30.43 min
Last of 35
11
Marathon
2 hr 9 min
2 hr 25 min
40
11
Why are males stronger and faster than women?
Hyperandrogenism in women
Causes of hyperandrogenism in women
Condition
Incidence
Comments
Advantage in sports?
Polycystic ovary syndrome (PCOS)
5–10%
In adults, testosterone levels often exceed the range for healthy women
Yes
Congenital adrenal hyperplasia (CAH)
Classic form 1/12 000Nonclassic form1/150?
XX. Classic form: virilized at birth.Nonclassic form: not virilized at birth. May be undiagnosed
Yes, but only if undertreated
5α-reductase type 2 deficiency
Very rare
XY individuals may be assigned female sex. At puberty, virilization proceeds
Yes
Complete androgen insensitivity (CAIS)
1/50 000?
XY. Completely female external genitalia. As adults, they have high testosterone, without effect
No
Partial androgen insensitivity (PAIS)
1/30 000?
XY. Ambiguous at birth. If the testes are in place, testosterone production may give moderate androgen signs at puberty
No
Ovotesticular DSD
Very rare
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access





