Hip Joint Orthopaedic Tests
Palpation
Descriptive Anatomy
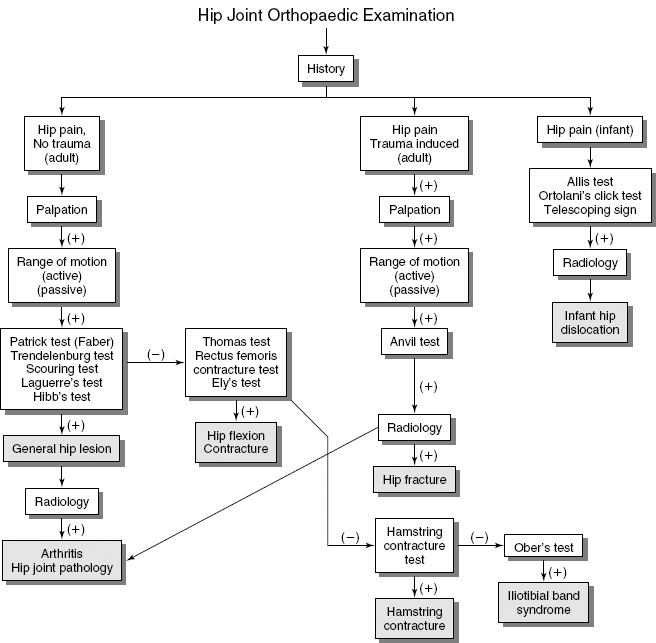
The iliac crest is at the inferior margin of the flank from the anterior; from the posterior, its highest point is at the level of the L4 spinous process (Fig. 13-1). The iliacus, external oblique, and tensor fasciae latae muscles originate from the iliac crest. At the anterior terminal end of the iliac crest lies the anterior superior iliac spine (Fig. 13-1). It is the attachment of the sartorius muscle and is easily palpable. The anterior inferior iliac spine is just below the anterior superior iliac spine. The rectus femoris muscle and iliofemoral ligament are attached to it (Fig. 13-1).
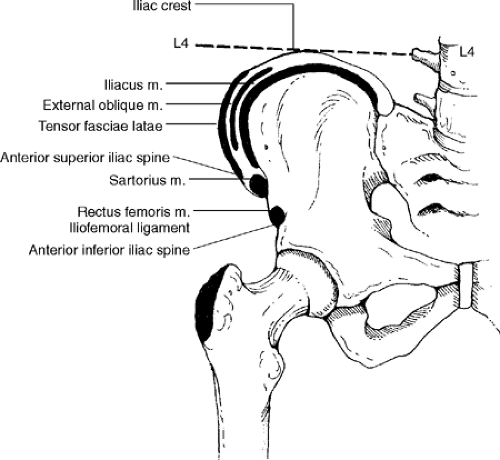 Figure 13-1 |
Procedure
With the patient supine, palpate the iliac crests for point tenderness and swelling (Fig. 13-2). This may indicate periostitis, strain or avulsion of the iliacus, external oblique, or tensor fasciae latae muscles. Contusion to the iliac crest secondary to trauma is common in the athlete. Palpate the iliac crests with the patient standing as well, checking for unevenness of the crests (Fig. 13-3). Unevenness may be a sign of scoliosis, anatomical short leg, or contracture deformity. The anterior superior iliac spine should be palpated next (Fig. 13-4). Look for point tenderness and swelling, which may indicate a sartorius muscle strain or avulsion fracture. Just below the anterior superior iliac spine is the anterior inferior iliac spine (Fig. 13-5). With your thumb or forefinger, palpate this area and note any point tenderness or swelling. It may indicate a sprained or avulsed rectus femoris muscle or strained iliofemoral ligament.
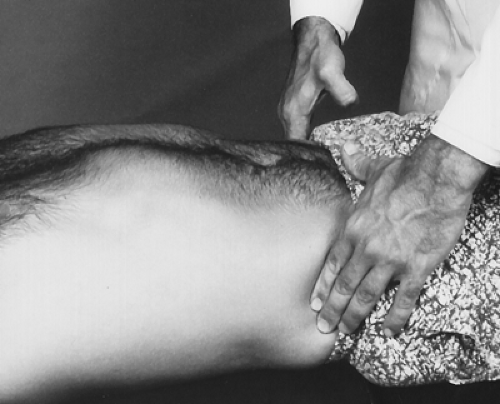 Figure 13-2 |
 Figure 13-3 |
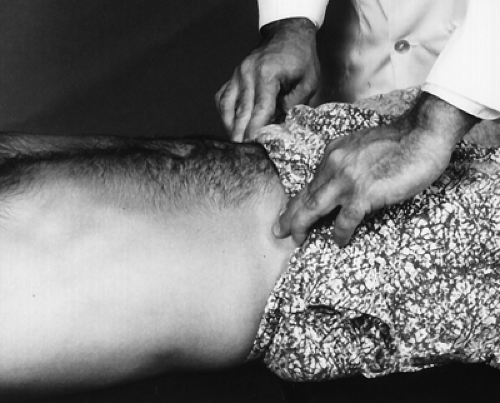 Figure 13-4 |
 Figure 13-5 |
Descriptive Anatomy
The greater trochanter is approximately 10 cm inferior and lateral to the anterior superior iliac spine (Fig. 13-6). The greater trochanter is the attachment of the gluteus medius, gluteus minimus, and vastus lateralis muscles. The trochanteric bursa also lies under these muscles.
Procedure
With the patient supine, slightly abduct the thigh and palpate the greater trochanter (Fig. 13-7). Note any point tenderness or swelling. This may indicate a strain of the gluteus medius, gluteus minimus, or vastus lateralis muscles. An increase in the temperature differential associated with tenderness and swelling is an indication of trochanteric bursitis.
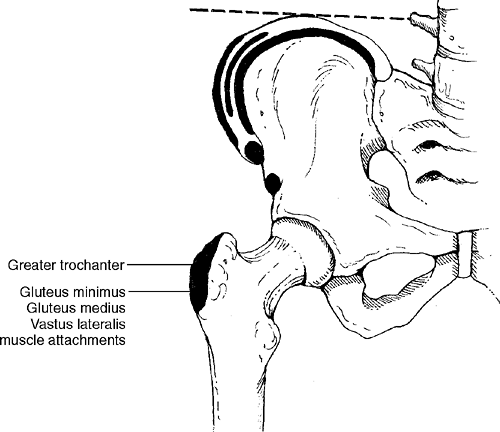 Figure 13-6 |
 Figure 13-7 |
Descriptive Anatomy
The hip joint is a ball and socket synovial joint, and the femur head is held in place by the iliofemoral, pubofemoral, and ischiofemoral ligaments (Fig. 13-8). The iliofemoral ligament is the largest and strongest of these ligaments that hold the femur into the acetabular cavity.
The hip joint at best is difficult to palpate because it lies deep in the body. Unless the joint is traumatized to the point of fracture or dislocation, palpation of the actual joint will reveal little clinical information. Palpation of the surrounding tissue may be a better indicator of hip joint pathology.
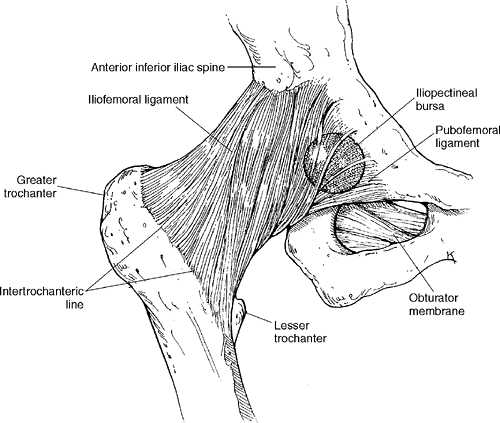 Figure 13-8 |
Descriptive Anatomy
The tensor fasciae latae muscle is on the anterior lateral side of the thigh. It originates from the anterior outer lip of the iliac crest and inserts into the iliotibial band, which attaches to the lateral epicondyle of the tibia (Fig. 13-9).
Procedure
With the patient laying on the unaffected side, palpate the tensor fasciae latae muscle from just below the anterior superior iliac spine down over the greater trochanter to the lateral aspect of the knee (Fig. 13-10). Note any tenderness, spasm, increase in skin temperature, or inflammation. These may indicate a strain of the muscle. If point tenderness is present, suspect an active trigger point that may refer pain to the upper half of the medial thigh. If the muscle becomes strained through microtrauma as it moves over the greater trochanter of the femur, it can cause greater trochanteric bursitis.
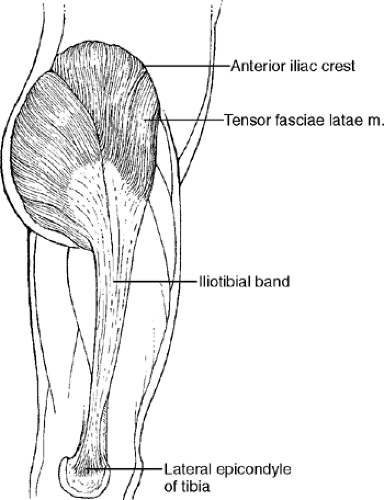 Figure 13-9 |
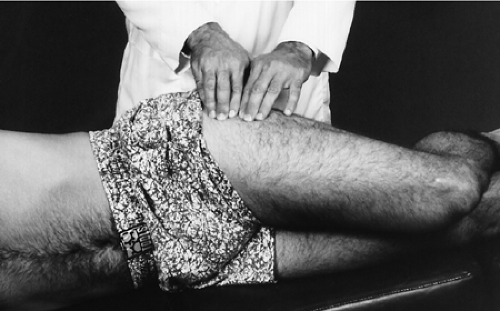 Figure 13-10 |
Descriptive Anatomy
The femoral triangle is a clinically important region. It is bound superiorly by the inguinal ligament, medially by the adductor longus muscle, and laterally by the sartorius muscle (Fig. 13-11). The triangle contains lymph nodes and the femoral artery, vein, and nerve.
Procedure
With the patient supine, palpate the inguinal ligament, which extends from the anterior superior iliac spine to the pubic tubercle. Note any tenderness, which may indicate a sprain. Next, palpate the adductor longus and sartorius muscle, again noting any tenderness or inflammation. This may indicate a strain or active trigger points in the affected muscle. Once the borders are palpated, palpate the interior of the triangle for inflamed lymph nodes, which may indicate a lower extremity or systemic infection (Fig. 13-12). Palpate the femoral artery for amplitude. A decrease in the amplitude indicates a compromise of the vascular supply to the lower extremity.
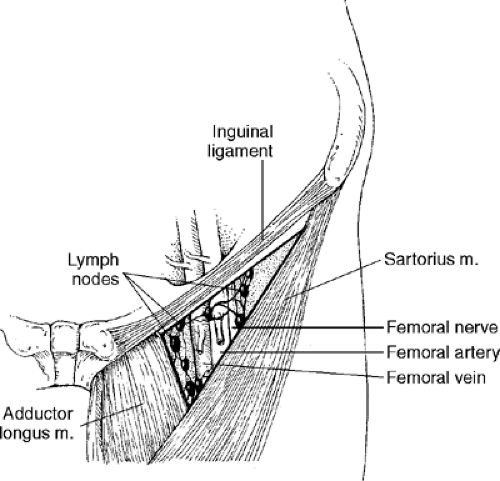 Figure 13-11 |
 Figure 13-12 |
Hip Range of Motion
With the patient supine, place the goniometer in the sagittal plane at the level of the hip (Fig. 13-13). Instruct the patient to flex the hip, and follow the thigh with one arm of the goniometer (Fig. 13-14).
Normal Range (2)
Normal range is 131° ± 6.4° or greater from the 0 or neutral position.
| Muscles | Nerve Supply |
|---|---|
| Psoas | L1–L3 |
| Iliacus | Femoral |
| Rectus femoris | Femoral |
| Sartorius | Femoral |
| Pectineus | Femoral |
| Adductor longus and brevis | Obturator |
| Gracilis | Obturator |
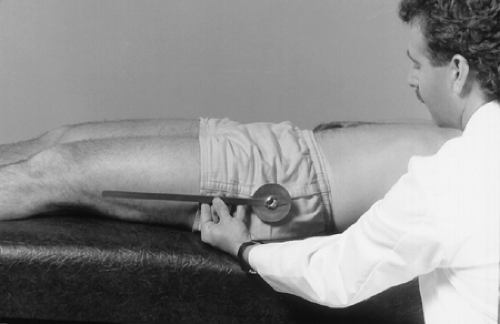 Figure 13-13 |
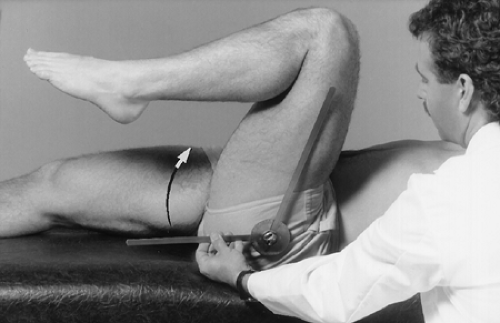 Figure 13-14 |
With the patient prone, place the goniometer in the sagittal plane at the level of the hip joint (Fig. 13-15). Instruct the patient to raise the thigh off the table as far as possible, and follow the thigh with one arm of the goniometer (Fig. 13-16).
Normal Range (2)
Normal range is 13° ± 5.4° or greater from the 0 or neutral position.
| Muscles | Nerve Supply |
|---|---|
| Biceps femoris | Sciatic |
| Semimembranosus | Sciatic |
| Semitendinosus | Sciatic |
| Gluteus maximus | Inferior gluteal |
| Gluteus medius | Superior gluteal |
| Adductor magnus | Sciatic |
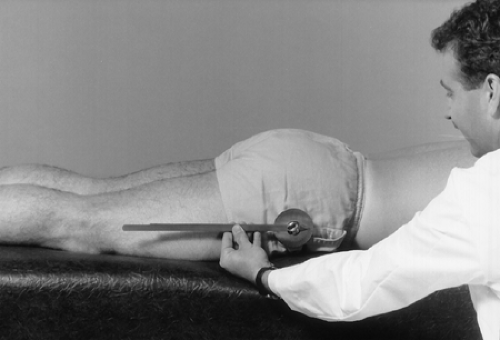 Figure 13-15 |
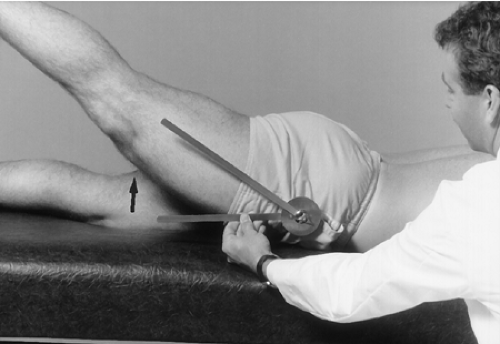 Figure 13-16 |
With the patient supine, place the goniometer in the coronal plane with the center at the level of the hip (Fig. 13-17). Instruct the patient to move the thigh laterally while following the thigh with one arm of the goniometer (Fig. 13-18).
Normal Range (2)
Normal range is 41° ± 6° or greater from the 0 or neutral position.
| Muscles | Nerve Supply |
|---|---|
| Tensor fasciae latae | Superior Gluteal |
| Gluteus minimus | Superior Gluteal |
| Gluteus medius | Superior Gluteal |
| Gluteus maximus | Inferior Gluteal |
| Sartorius | Femoral |
 Figure 13-17 |
 Figure 13-18 |
With the patient supine and the opposite hip flexed, place the goniometer in the coronal plane with the center at the level of the hip (Fig. 13-19). Instruct the patient to move the thigh medially while following the thigh with one arm of the goniometer (Fig. 13-20).
Normal Range (2)
Normal range is 27° ± 3.6° or greater from the 0 or neutral position.
| Muscles | Nerve Supply |
|---|---|
| Adductor longus | Obturator |
| Adductor brevis | Obturator |
| Adductor magnus | Obturator |
| Gracilis | Obturator |
| Pectineus | Femoral |
 Figure 13-19
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
