Chapter 23 Tumour growth and spread


Benign and malignant tumours
Benign tumours grow by forming an expansile mass that gradually compresses adjacent tissues (Fig. 3.23.1 and Table 3.23.1). Examination of benign tumours with the naked eye shows that they are well-circumscribed lesions while histological examination may also reveal a compressed rim of non-neoplastic tissue. Sometimes a rim of fibrous tissue is present at the edge of benign tumours, and this is referred to as a tumour capsule. The clinical effect of compression of adjacent tissues by the tumour depends on the site (Ch. 24). Benign tumours do not possess the ability to metastasize to distant sites but they can still cause substantial damage (Table 3.23.2).
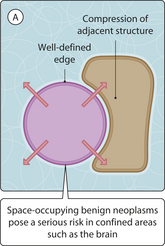
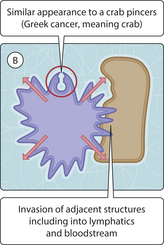
Table 3.23.1 THE MAJOR DISTINGUISHING FEATURES OF BENIGN AND MALIGNANT TUMOURS
| Feature | Benign | Malignant |
|---|---|---|
| Cardinal featuresa | ||
| Effect of primary tumour on adjacent tissues | Compression | Invasion |
| Edge of tumour | Well defined | Poorly defined |
| Distant metastases | Absent | Present |
| Other primary features | ||
| Vascular invasion: within lymphatics or blood vessels | Absent | Present |
| Cellularity: tumour cells per unit area of tumour | Low | High |
| Nucleus-cytoplasm ratio of tumour cell | Low | High |
| Differentiation: how much tumour overall growth pattern resembles that of its non-neoplastic counterpart | Good | Variable; often poor |
| Nuclear pleomorphism: size and shape of nuclei | Mild | Variable; may be marked |
| Mitotic index: morphological evidence of active cell division | Low | Variable; may be high |
bMarked nuclear pleomorphism is often associated with an irregular nuclear chromatin pattern and/or nuclear hyperchromasia (dark nuclei as seen on routine H&E staining).
a Most commonly used to determine biological behaviour of tumours.
Table 3.23.2 CLINICAL PROBLEMS ARISING ON ADJACENT STRUCTURES
| Primary site | Adjacent structure | Clinical problem |
|---|---|---|
| Breast | SkinChest wall | UlcerationTumour fixation |
| Brainstem | Cardiovascular centre | Death |
| Colon | Bladder | Fistula formation |
| Pancreas | Common bile duct | Obstructive jaundice |
| Lung | OesophagusPulmonary artery | DysphagiaFatal haemoptysis |
| Prostate | Prostatic urethra | Urinary retention |
Malignant tumours form a mass at their primary site, which may compress but which also characteristically invades into adjacent tissues. The term cancer means crab and was coined in reference to the ability of malignant tumours to infiltrate adjacent tissues with a growth pattern that resembles a crab with long legs and pincers. Malignant tumours often create significant clinical problems at their primary site (Ch. 24) but may additionally spread (metastasize) to distant sites. This latter characteristic accounts for most of the mortality associated with malignant tumours and is the subject of much research. Metastasis may occur through one or more of several routes (Table 3.23.3). In order to metastasize, tumour cells must be able to perform certain tasks at different times (Chs 26–29):
< div class='tao-gold-member'>

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


