Fig. 68.1
Joint fluid aspiration, acute gout, 400×. The coverslipped unstained specimen is viewed in polarized light with a first-order compensator. In this field are many neutrophils with ingested monosodium urate monohydrate crystals diagnostic of acute gout. The crystals are needle shaped, and those parallel to the extraordinary (“slow”) compensator axis (vector direction indicated by the black arrow) are bright yellow, indicating a negative sign of birefringence. Those perpendicular to this axis are blue, and those that are intermediate either vary in color or approach extinction

Fig. 68.2
This 43-year-old patient became hyperuricemic after having developed chronic renal failure secondary to diabetes mellitus. The radiographs of the foot demonstrate periarticular erosions of the foot and hands with preservation of the joint spaces and intraosseous tophaceous urate deposits of the terminal phalanges (white arrows). In addition, there is significant periosteal reaction about the right first metacarpal (black arrows) secondary to subperiosteal urate deposits extending into the soft tissues
Fig. 68.3
Tophaceous gout, right hand of a patient with chronic untreated gout. The interphalangeal and metacarpophalangeal joints are irregularly eroded and a few show advanced joint narrowing. There is obvious soft tissue swelling in the radiograph. The gross appearance of the hand demonstrates the obvious soft tissue deposits of urate with overlying erythema, epidermal atrophy, and skin defects corresponding to the sites’ gross drainage of crystalline deposits
Fig. 68.4
Tophaceous deposits of monosodium urate in subarticular region of femoral head with overlying collapse of articular cartilage (left) and in fragments of the synovium from the same joint (right). Note that the urate deposits appear friable and chalky white
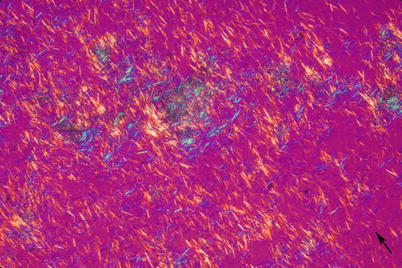
Fig. 68.5
Touch preparation of gouty tophus, unstained and coverslipped viewed in polarized light with first-order compensator (400×), demonstrates needle-shaped strongly anisotropic crystals with negative birefringence (black arrow is the direction of slow compensator axis). When aqueous fixation and processing is unavoidable, touch preparations are an important way to permanently document the presence of urate crystals
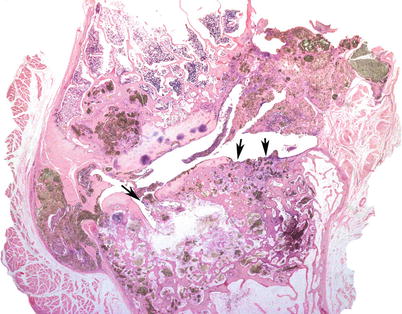
Fig. 68.6
Resected interphalangeal joint, advanced tophaceous gout. Crystalline deposits, appearing brownish green are visible at joint margins and in subarticular regions, and the joint cartilages are focally disrupted (arrows). (Hematoxylin and eosin, 10×)
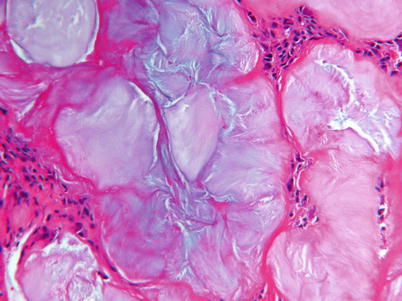
Fig. 68.7
Tophaceous urate deposit, (hematoxylin and eosin, 250×), after aqueous processing. The crystals are dissolved by the processing, leaving amphophilic, striate-appearing ghosts still surrounded by a foreign body reaction
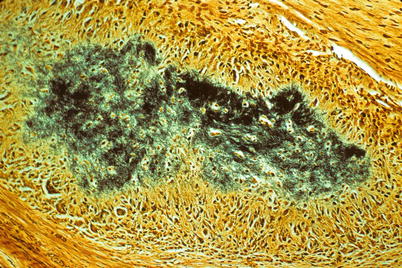
Fig. 68.8
Tophaceous gout deposit, DeGolantha stain for urate. The needle-shaped monosodium urate crystals appear black, and there is a prominent foreign body giant-cell reaction surrounding them (200×)
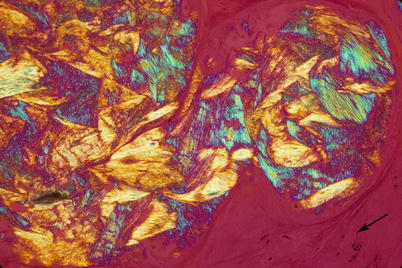
Fig. 68.9




Gout tophus, acid eosin processing, and alcohol fixation with preservation of monosodium urate monohydrate crystals that usually dissolve during aqueous fixation and staining (250×, polarized light with first-order compensator). The arrow designates the direction of the slow compensator axis
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
