Golf
Richard J. Emerson
Kerry Graham
Golf is enjoyed worldwide by millions of people each year and is considered one of the most rapidly growing sports. In 2002, 32.3 million people in the United States played at least one round of golf. Of those golfers, 45% were between the ages of 18 and 39. Golfers 50 years and older represented 33%, and junior golfers make up 5% of the golf population. The National Golf Foundation (NGF) also noted that 20% of the golfing population plays over 25 rounds per year (avid golfers). There are 14,725 golf course facilities available in the United States, a 20% increase in the last 7 years. The golf economy in the United States accounted for over $62 billion worth of goods and services in the year 2000 (1).
THE ATHLETE
Much of golf’s popularity stems from its low physical demand on the body, allowing the sport to be enjoyed by young and old alike. For those unfamiliar with the game, golf appears to be relaxed and unathletic. However, muscle endurance, strength, flexibility, and cardiovascular fitness are all required for the sport (2). Because golf is considered to be low intensity with low physical demand, it has not been considered a high injury risk sport (3). Unfortunately, though, injury is one of the most common reasons for players to leave the game each year. The types and frequency of injuries that occur while playing golf are common among men and women, amateurs and professionals alike, with some variations related to the low back, wrist, and hand (4). Common injury sites in golf players include the wrist, elbow, shoulder, knee, and most commonly the back (5). Excessive repetition, poor swing mechanics, lack of conditioning, poor fitness, and improperly fitted golf clubs are primary factors in the etiology of these injuries.
Fitness and strength training programs are now routinely part of the golf program at colleges and universities throughout the United States. Junior golfers and high school golf teams have more interest in year-round performance enhancement programs that include skill assessment, strength, conditioning, and fitness. This positive trend will promote the safety and well-being of these young athletes.
THE GAME
Significant advances in technology have improved golf clubs and golf balls enhancing the player’s ability to hit longer and more accurate shots. New technology has also produced shafts and grips that decrease impact stress on the golfer’s elbows, shoulders, and wrists. Video and computer motion-measuring technology has dramatically influenced the ability to analyze the components of the golf swing meticulously and with precision. When combined with the proper medical evaluation, clinicians and golf pros can detect swing flaws that may create pain syndromes and have an impact on performance.
Golf Swing Biomechanics
With new innovations in equipment and technology, the swing has evolved over the years, allowing shot making with increased precision and distance. Players using the classic swing (pre-1930) (Fig. 31.1A) and playing with hickory
shafts and bulky clothing had a backswing that was on a more linear swing plane, allowing for concomitant hip and shoulder rotation with the player in an upright “I” position for follow-through. However, the modern swing (Fig. 31.1B) uses a more coiled body position in which there is a greater rotation of the shoulder with restriction of motion at the hips. As the swing has evolved, it has also created more stress on the body (6).
shafts and bulky clothing had a backswing that was on a more linear swing plane, allowing for concomitant hip and shoulder rotation with the player in an upright “I” position for follow-through. However, the modern swing (Fig. 31.1B) uses a more coiled body position in which there is a greater rotation of the shoulder with restriction of motion at the hips. As the swing has evolved, it has also created more stress on the body (6).
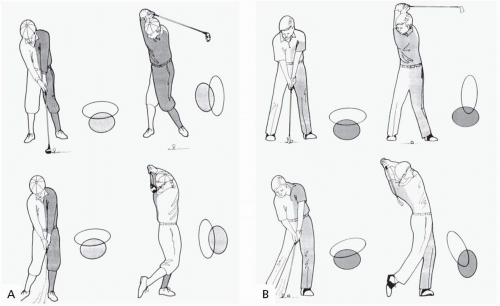 FIGURE 31.1. Evolution of the golf swing. A, Classic (pre-1930s). B, Modern (2000). |
Evolution of the Golf Swing
Classic (pre-1930s)
Club shafts could not be stressed or they would break.
Players wore suit coats, which made the swing more restricted.
Hips and shoulders turned almost equally.
The player rose up on the lead toe in the backswing.
More upright “I” follow-through position created less stress on the low back.
Modern (2000)
Based on economy of motion and coil.
Coil and weight shift have become the main focus.
Large shoulder turn and minimal hip turn—the X-factor.
A back-bend, “C”-shaped follow-through torques the low back.
During the swing of an elite golfer, a repeatable sequence of muscle activation occurs. The abdominal muscles contract, transferring the forces into the torso and activating the pectoralis and latissimus dorsi muscles. Transfer of kinetic energy then moves into the shoulders and rotator cuff, especially the subscapularis and arms. A very important counteraction occurs when abdominal muscle contraction causes the spine to move forward, forcing the lumbar paraspinal muscles to contract, counteracting the abdominal muscles. Of additional significance, the spine receives forces with four different stress loads: (a) lateral flexion, (b) anterior posterior shearing, (c) rotation, and (d) compression (7).
The early scientific efforts by Jobe and Pink through their electromyographic analysis of the golf swing (8) set the stage for continued medical research that unfortunately has been fairly slow
and intermittent. Recently, SportExcel Health and Human Performance in Scottsdale, Arizona, has evaluated thousands of golf swings with video and computerized swing and motion analysis equipment to identify six common factors that separate the elite from less skilled players. These factors are measurable and found to be repeated by the more skilled and successful golfers.
and intermittent. Recently, SportExcel Health and Human Performance in Scottsdale, Arizona, has evaluated thousands of golf swings with video and computerized swing and motion analysis equipment to identify six common factors that separate the elite from less skilled players. These factors are measurable and found to be repeated by the more skilled and successful golfers.
The Six Common Factors
There is a correct address position that includes proper body posture, spine angle, grip, stance, and balance.
The club should stay on plane during the swing. The plane is established at setup and is determined by the golfer’s body and club dimensions.
The pelvis should be slightly rotated toward the target at impact.
Balance and weight transfer. The golfer must remain in balance throughout the swing, and his or her weight transfers to the back foot in the backswing and to the forward foot during the forward swing and follow-through.
The back leg is “posted” in the backswing— i.e., it does not move during the swing— and provides resistance and stability as body weight is moved onto it (loads) in the backswing. The angle of flexion in the knee and hip is retained as the upper body rotates and weight is transferred.
Golf clubs should be properly fit to the individual.
The likelihood of achieving squareness of club face and centeredness of hit at impact markedly increases with greater recruitment of the six common factors during the swing; squaredness and centeredness are necessary to achieve maximum distance and accuracy. Inability by a golfer to accomplish factors 1 through 5 with excellence is often due to physical deficiency or injury. Increasing flexibility, improving conditioning, or resolving the injury often allows the golfer to increase excellence in the first five common factors.
The sixth common factor—proper club fitting—is vital to the performance of the first five factors. Feedback to the golfer’s brain is instantaneous once the ball’s flight is observed. A “good swing” is rewarded with a “good shot” only if the equipment is fit for the individual. Otherwise, a “good swing” could result in an errant shot and the golfer then begins to compensate with biomechanical swing changes to control the ball’s flight. There is a marriage between proper club fitting and a biomechanically accurate golf swing. Equipment creates the swing shape.
In order to understand the biomechanics of the golf swing and golf-related injuries, one must keep in mind the effect that equipment fit has on the individual golfer’s performance. Proper swing mechanics can occur repetitively only if the golfer is swinging without hitting a ball (practice swing), or if the equipment is properly fit to the golfer. Improper swing mechanics and injury to the golfer can be caused by compensation for improperly fit equipment.
THE SWING
There are six phases to a properly executed golf swing:
Setup/Address
Backswing
Top/Transition
Forward swing/Acceleration
Impact
Early Follow-through/Late follow-through
Setup and Address.
The setup is where everything good or bad begins. By establishing the proper address position, the player has proper balance, both within his or her body and the golf club. Starting in a balanced position enhances the golfer’s opportunity to remain balanced throughout the execution of the swing. If the club is properly fit to the individual’s body dimensions and strength, the result of a balanced address and swing will give the desired outcome—an accurate shot in direction and distance.
At setup, the weight is evenly balanced both between the feet and toe-to-heel while maintaining proper spine angles (Fig. 31.2A). There is lateral spine flexion relative to the hips, but not
flexion of the spine itself (9). The feet should be wide enough to support the swing motion without restricting pelvic rotation (about shoulder width apart), and the toes should be turned slightly outward. Commonly, professionals turn the forward toe out more than the back toe. If the toes are turned in too much, the knees may resist the turning motion which leads to excess stress on the knee joints. The knees and hips are in a game-ready position when the body is balanced and the spine angles and flexion of the hips and knees are proper. Proper clubs and equipment analysis relative to the individual golfer’s body measurements, strength, and motion are critical as every sequence to follow is part of a domino effect, either positive or negative.
flexion of the spine itself (9). The feet should be wide enough to support the swing motion without restricting pelvic rotation (about shoulder width apart), and the toes should be turned slightly outward. Commonly, professionals turn the forward toe out more than the back toe. If the toes are turned in too much, the knees may resist the turning motion which leads to excess stress on the knee joints. The knees and hips are in a game-ready position when the body is balanced and the spine angles and flexion of the hips and knees are proper. Proper clubs and equipment analysis relative to the individual golfer’s body measurements, strength, and motion are critical as every sequence to follow is part of a domino effect, either positive or negative.
 FIGURE 31.2. The golf swing. A, Setup and address. B, Backswing. C, Top/transition. D, Acceleration/forward swing. E, Impact. F, Early follow-through. G, Late follow-through. |
Backswing.
Less than one fourth of all injuries occur during the backswing (10). It is a synchronous, linked progression of torque, rotation, and load transfer through the feet up through the knees, hips, torso, lumbar spine, and cervical spine (Fig. 31.2B). The player’s weight transfers to the back foot, the left thumb hyperextends, the left wrist radially deviates, and the right wrist dorsiflexes and radially deviates (10). The head position remains fairly constant; however, individual preferences occur. While the head may move slightly away from the target during the backswing, it is improper for it to ever move toward the target during this phase of the swing. The key to a successful backswing is to allow each motion to flow and coordinate with the other motions; thus, flexibility is essential.
Golf swing motion theories often get validation from golf magazines and television instruction programs instead of scientific research or small sample groups. There has been little long-term scientific research conducted on the modern golf swing in relation to the effects on the body and parameters for success. For instance, research in 1996 was presented in popular golf magazines and on television golf instruction claiming that the difference between the hip and shoulder rotation at the top of the backswing is critical in generating power (11). The concept of creating torque by increasing shoulder rotation while keeping a more fixed hip rotation at the top of the backswing became known as the X-factor. McTeigue and Anderson noted that by creating a larger gap at the top of the backswing, a
more complete closure occurred on the downswing allowing for greater club head velocity at impact (11).
more complete closure occurred on the downswing allowing for greater club head velocity at impact (11).
However, attempting to execute the X-factor has created an increased risk of injury for many golfers. Increased torsion of the upper torso with fixed hip placement causes an aggressive shoulder rotation with increased stress to the lower back. Cheetham and coworkers in 2001 noted that research does not prove that the X-factor increases club head speed or distance for professionals or amateurs (12). They claim instead that the X-factor stretch, which measures a separation distance at a point “between” the top of the backswing and impact, has a higher correlation to greater club head velocity at impact. Both of these theories invite additional research on a larger population.
Biomechanical inconsistencies during the backswing can lead to numerous injuries:
Left wrist flexor carpi ulnaris stretching, leading to tendinitis.
Neuropathy of the left wrist with ulnar nerve compression.
Dorsal carpal ligament syndrome and extensor tendinitis from right wrist dorsiflexion.
Impingement of the right shoulder during hyperabduction.
Low back strain from lumbar spine hyperrotation.
Medial epicondylitis from overstretching of the right elbow flexors.
Top/Transition.
Differences in terminology exist for when the top of the backswing is completed (Fig. 31.2C) due to the fact that the body is beginning its forward motion while the club is still in a backswing mode, thus the resulting label of transition stage (13).
Acceleration/Forward Swing.
During the forward swing, the club is returned to its original position to hit the ball at the correct angular trajectory and at maximum speed (Fig. 31.2D). Several events are occurring at this moment:
The player’s weight is shifted to the forward foot by a parallel movement of the hips and shoulders, while he or she maintains a constant spine angle and hip flexion.
The hips initiate the change of direction, and the upper body rotates faster than the hips.
The abdominal muscles provide the power for the trunk to rotate.
The rotation of the hips and knees accompanies trunk rotation.
The paraspinal muscles stabilize the spine.
The subscapular and pectoralis major muscles contribute to arm acceleration.
The rotational capacity of the trunk is the most important lever in achieving maximum speed during the swing. Golfers that do not have the rotational capacity must compensate with greater muscular activity.
Biomechanical inconsistencies during the forward swing can lead to numerous injuries, such as the following:
Tendinitis as a result of left thumb hyperabduction.
Medial epicondylitis from right elbow forearm load of the flexors.
Ulnar-deviated wrist impaction leading to ulnar neuropathy, hamate fracture, or flexor carpi ulnaris tendinitis.
Right knee medial valgus strain, leading to tibial collateral ligament strain.
Lateral epicondylitis resulting from left elbow lateral extensor tendon lengthening with deceleration or impact with the ground.
Impact.
When the club impacts the ball, the kinetic energy produced during the forward swing is transferred to the ball (Fig. 31.2E). At the point of impact, the acceleration that is created from the forward swing is coupled with acceleration from the wrist and hands. To maximize the distance that the ball will travel, acceleration does not stop until after the ball is struck. Weight transfer to the forward foot is critical to create proper balance and ball flight but also to avoid injury that could be caused by excess transfer of energy to the back and extremities.
At impact, skilled golfers transfer more weight to the heel, as opposed to lesser skilled golfers who transfer their weight toward the middle or toe of the foot. Valgus stress occurs on the right knee, both wrists are under compression, and the left elbow extensor muscles contract. Therefore, the left wrist, hand, and elbow are at risk during impact, not only from contact with the golf ball but also from contact with the ground.
At impact, skilled golfers transfer more weight to the heel, as opposed to lesser skilled golfers who transfer their weight toward the middle or toe of the foot. Valgus stress occurs on the right knee, both wrists are under compression, and the left elbow extensor muscles contract. Therefore, the left wrist, hand, and elbow are at risk during impact, not only from contact with the golf ball but also from contact with the ground.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


