posteriorly. Most of the fibers of the fibrous capsule take a spiral course from the hip bone to the femur. The synovial membrane, which lines the fibrous capsule, also covers the neck of the femur, which is intracapsular, and the nonarticular portion of the acetabulum as well as the ligament of the femoral head. The strong Y-shaped iliofemoral ligament reinforces the fibrous capsule anteriorly and is extremely important in preventing overextension of the hip during standing by screwing the head of the femur into the acetabulum.
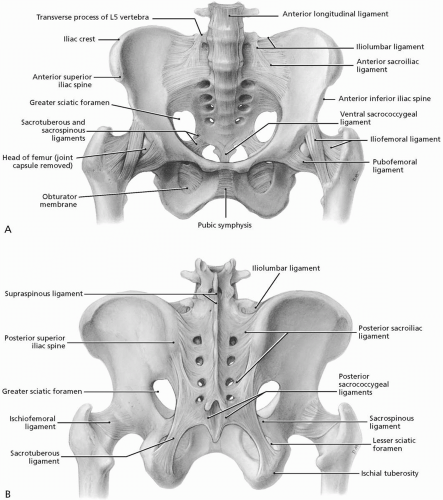 FIGURE 22.1.1. A, Anterior bony pelvis with important ligaments. B, Posterior bony pelvis. (From Agur AMR, Lee ML. Grant’s Atlas of Anatomy, 10th ed. Baltimore: Lippincott Williams & Wilkins, 1999.) |
which tightens during extension and abduction of the hip, thereby preventing overabduction at the joint. The ischiofemoral ligament reinforces the hip joint posteriorly where it screws the head of the femur medially into the acetabulum during extension, thereby preventing hyperextension of the joint. The intracapsular ligament of the femoral head, which connects the acetabulum to the femoral head, is weak and usually contains a small artery to the head of the femur. The hip joint movements are flexion-extension, abduction-adduction, medial-lateral rotation, and circumduction.
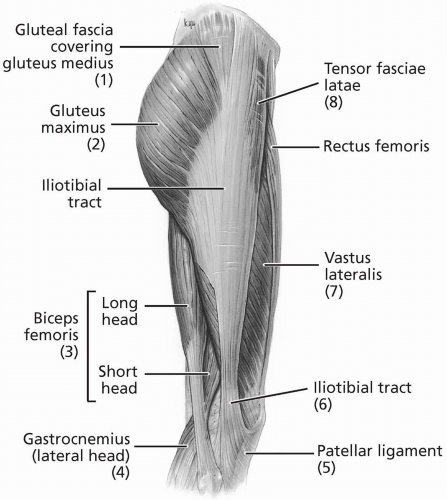 FIGURE 22.1.2. Lateral hip and thigh. Highlighted is the full extent of the iliotibial tract, from the iliac crest into the tibial plateau and fibular head. (From Agur AMR, Lee ML. Grant’s Atlas of Anatomy, 10th ed. Baltimore: Lippincott Williams & Wilkins, 1999.) |
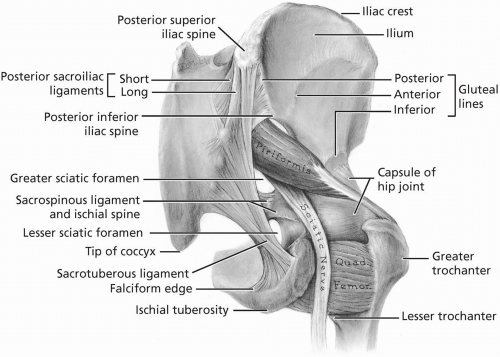 FIGURE 22.1.3. Posterior view of the hip. Note the relationship among the sciatic nerve, the piriformis muscle, the sacrotuberous ligament, and the hip capsule. (From Agur AMR, Lee ML. Grant’s Atlas of Anatomy, 10th ed. Baltimore: Lippincott Williams & Wilkins, 1999.) |
lymph nodes can be palpated in the most medial portion of the triangle.
Crosses L5-S1 and distributes forces from the large range of motion above through to the relatively limited movement of the sacrum.
Distributes forces from below the pelvis cephalad.
Originates at the inferior border of the transverse process of L1-L5 and the anterolateral surfaces of the vertebral bodies of T12-L5 and the intervertebral discs between them.
Anchors the crura of the diaphragm and is involved in respiratory function.
Moves the sacrum in an anterior-posterior fashion.
Acts as a prime mover of the lumbosacral junction, influencing sacral mechanics.
Affects the lumbar curve. Relaxation of the psoas muscle allows the normally present lumbar lordosis to flatten. Stretching of the iliopsoas muscle may alleviate low back discomfort. A home stretching program directed at the iliopsoas may alleviate pain in the low back.
Affects mechanics of gait, respiration, and the sequence of engagement, flexion, descent, and internal rotation of the fetus.
medius and minimus (Fig. 22.1.7). The gluteus medius is the main hip abductor. The superior gluteal nerve (L5, S1) innervates both muscles.
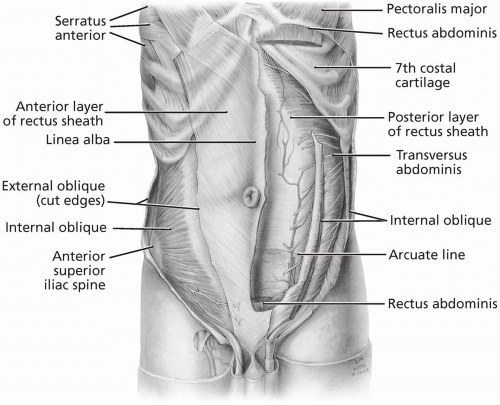 FIGURE 22.1.4. Abdominal wall musculature, deep dissection. (From Agur AMR, Lee ML. Grant’s Atlas of Anatomy, 10th ed. Baltimore: Lippincott Williams & Wilkins, 1999.) |
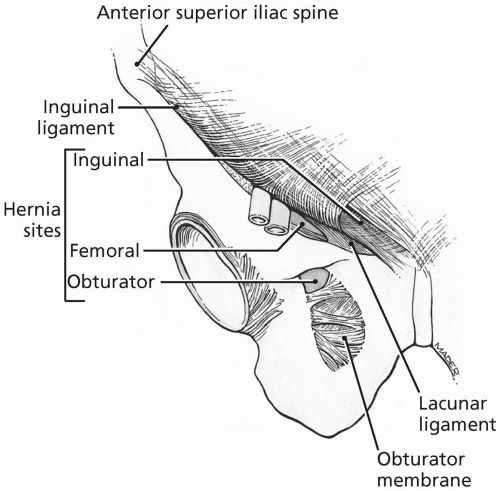 FIGURE 22.1.5. Anteroinferior view of the three hernia sites in the inguinal region. (From Agur AMR, Lee ML. Grant’s Atlas of Anatomy, 10th ed. Baltimore: Lippincott Williams & Wilkins, 1999.) |
and short heads, semitendinosus, and semimembranosus) muscles. The gluteus maximus is the primary hip extensor and can be located between two imaginary lines drawn between the posterior superior iliac spine and the greater trochanter superiorly and the coccyx and ischial tuberosity inferiorly. The hamstring muscles, except for the short head of the biceps femoris, all attach proximally to the ischial tuberosity deep to the gluteus maximus. The inferior gluteal nerve (L5, S1-S2) innervates the gluteus maximus. The tibial division of the sciatic nerve (L5, S1-S2) innervates the semitendinosus, semimembranosus, and long head of the biceps femoris, while the common fibular portion of the sciatic nerve (L5, S1-S2) innervates the short head of the biceps femoris.
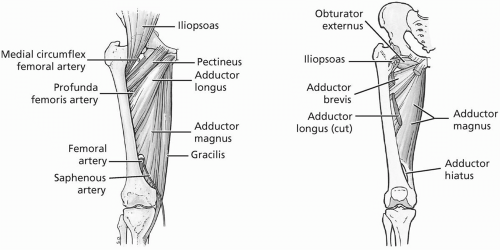 FIGURE 22.1.6. Medial thigh musculature. (From Agur AMR, Lee ML. Grant’s Atlas of Anatomy, 10th ed. Baltimore: Lippincott Williams & Wilkins, 1999.) |
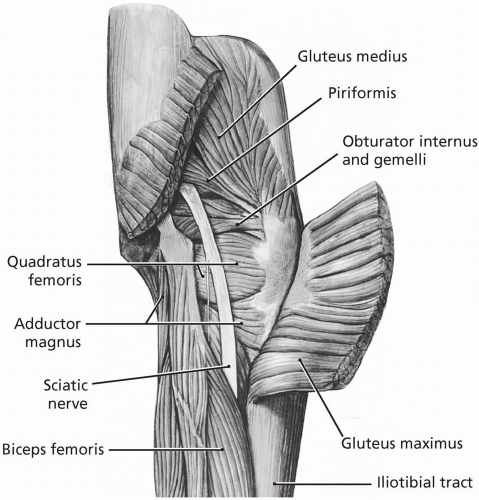 FIGURE 22.1.7. Muscles of the gluteal region. (From Agur AMR, Lee ML. Grant’s Atlas of Anatomy, 10th ed. Baltimore: Lippincott Williams & Wilkins, 1999.) |
 FIGURE 22.2.1. Posterior superior iliac spine. |
Anterior superior iliac spine (ASIS). Palpate the superior-anterior portion of the iliac crest.
Iliac crest. Assess pelvic obliquity.
Iliac tubercle. Located posteriorly on the lateral lip of the iliac crest, it marks the widest portion of the pelvis.
Pubic tubercle. Follow the inguinal ligament to the front of the pubis, which is at the same level as the top of the greater trochanter (5).
Femoral triangle (inguinal ligament, femoral artery, and inguinal lymph nodes). Place the athlete’s leg in a figure-four position: The femoral artery is in the midpoint of the triangle, and the hip capsule is approximately 2 cm laterally and proximally. From medial to lateral, the neurovascular structures are the femoral vein, femoral artery, and femoral nerve (VAN) (1,3).
Adductor muscle group is palpable with the athlete’s leg in an abducted position.
Abductor (gluteus medius).
Flexors (iliopsoas and sartorius).
 FIGURE 22.2.2. Lateral palpation of the greater trochanters. |
Posterior superior iliac spine. It lies under the dimples above the buttocks.
Ischial tuberosity (lateral side lying). Flex the athlete’s hip for easy palpation; it is located at the level of the gluteal fold.
Extensors (gluteus maximus and hamstrings).
Sacroiliac (SI) joint. It is not palpable with the overhang of the iliac crest. The top of the SI joint is even with the top of the L4-L5 vertebrae.
Greater trochanter (lateral side lying). The posterior aspect of the greater trochanter is relatively uncovered in this position and easily palpable.
Greater trochanteric bursa (sciatic nerve— midway between the greater trochanter and the ischial tuberosity).
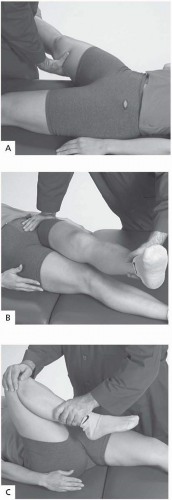 FIGURE 22.2.3. Range of motion. A, Abduction: 45 degrees. B, Adduction: 20 to 30 degrees. C, Flexion: 120 to 135 degrees. |
Abduction: 45 degrees (Fig. 22.2.3A). With true hip pathology or degenerative arthritis, abduction is much more limited than adduction.
Adduction: 20 to 30 degrees (Fig. 22.2.3B).
Flexion: 120 to 135 degrees (Fig. 22.2.3C).
The athlete lies supine on the examination table.
The examiner stabilizes the pelvis by placing a hand under the lumbar spine.
The examiner then flexes both hips up until the lumbar spine flattens.
The athlete can use his or her hands to hold the legs near the chest. From this point on, only hip flexion allows the leg to move, and the athlete should be able to touch the abdomen (120 to 135 degrees).
The athlete then extends one leg and lets it rest on the table. The leg will lie flat in a normal hip. (Fig. 22.2.4)
Extension: 30 degrees (Fig. 22.2.5). This is best tested in the prone position with the
knee slightly bent to relax the hamstrings. If the hip cannot extend, a flexion contracture is possible.
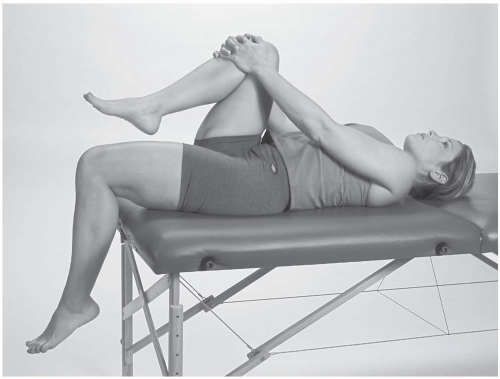
FIGURE 22.2.4. Thomas’s test.
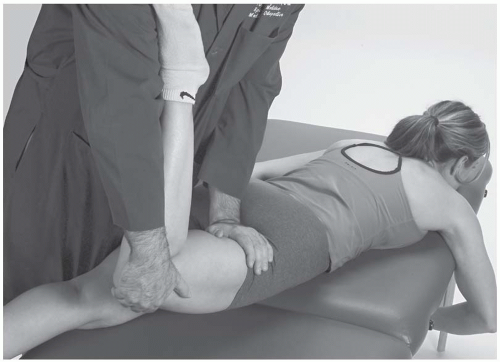
FIGURE 22.2.5. Extension.
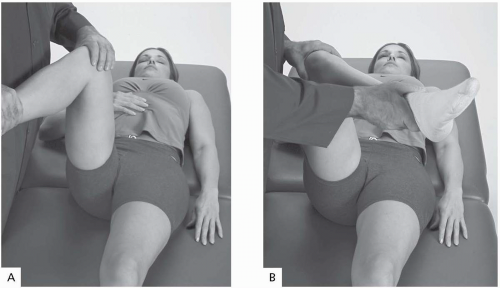
FIGURE 22.2.6. A, Internal rotation. B, External rotation.
Internal rotation: 35 degrees (Fig. 22.2.6A).
External rotation: 45 degrees (Fig. 22.2.6B).
Flexors
Extensors
Abductors
Adductors
Internal rotators
External rotators
TABLE 22.2.1. HIP MUSCLES | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


