General Considerations
Peter F. M. Choong
Tumor resections about the ankle are uncommon because primary and secondary malignancies infrequently develop in this region. Should they occur, then the two sites that have the greatest impact on ankle function are the distal tibia and the talus. In the nononcologic setting, the greater use of ankle prostheses has witnessed the potential for greater numbers of revision surgery. Advances in technique, biologic reconstructions, prosthetic design, and experience with ankle joint replacement coupled with a better understanding of the indications and contraindications have increased the popularity of limb-sparing surgery for distal tibial and ankle tumors. Whether surgery is for tumor or complex arthroplasty, procedures about the ankle require special care because of the confluence of neurovascular structures anteriorly and medially around the ankle, the relative thinness of the investing skin of the ankle, and the need for the ankle to sustain the entire body weight when standing or moving.
INDICATIONS
Primary malignancies of the distal tibia are few. Of these, osteosarcoma and Ewing sarcoma are by far the commonest. Both these tumors distinguish themselves by the soft tissue component, which frequently accompanies the tumor’s development (Fig. 23.1A,B). In the confined area of the ankle, extraosseous extension of the tumor may compromise the ability to undertake limb-sparing surgery. The main reasons are the lack of a robust layer of soft tissue around the ankle to provide the necessary structures to include in a wide margin and the vulnerability of the neurovascular structures that hug the ankle joint. Successful surgical management has a great reliance on chemotherapy or radiotherapy to assist in the containment and reduction of the soft tissue component of both these tumors.
If limb-sparing surgery is possible, then careful dissection would be required to prevent injury to the vital structures and the overlying skin or transgression of the tumor boundaries. In planning a wide resection of
the distal tibia, care must be taken to accurately calculate the amount of residual tibia remaining after tumor resection. This will determine the type of reconstruction possible. For example, short resections lend themselves to almost all varieties of reconstructions including biologic reconstructions (Fig. 23.2A-H), prosthetic reconstructions, and combinations of these (1,2,3,4,5,6). Long resections, however, make prosthetic reconstructions with megaprostheses difficult because of the lack of tibial length to contain the stem of a megaprosthesis. Unlike the femur where long resections of either the proximal or distal femur may be converted to total femoral resections, no device or reconstruction is readily available for extended tibial resections. In this regard, appropriate
care must be taken to exclude the presence of intramedullary skip lesions. If limb-sparing surgery cannot be undertaken with oncologically sound margins or the potential for postoperative complications outweigh the benefits of this surgery, then below knee amputation should be seriously considered (Fig. 23.3A-C). The function possible with appropriately fitted amputation prostheses, after below knee amputation, is generally excellent.
the distal tibia, care must be taken to accurately calculate the amount of residual tibia remaining after tumor resection. This will determine the type of reconstruction possible. For example, short resections lend themselves to almost all varieties of reconstructions including biologic reconstructions (Fig. 23.2A-H), prosthetic reconstructions, and combinations of these (1,2,3,4,5,6). Long resections, however, make prosthetic reconstructions with megaprostheses difficult because of the lack of tibial length to contain the stem of a megaprosthesis. Unlike the femur where long resections of either the proximal or distal femur may be converted to total femoral resections, no device or reconstruction is readily available for extended tibial resections. In this regard, appropriate
care must be taken to exclude the presence of intramedullary skip lesions. If limb-sparing surgery cannot be undertaken with oncologically sound margins or the potential for postoperative complications outweigh the benefits of this surgery, then below knee amputation should be seriously considered (Fig. 23.3A-C). The function possible with appropriately fitted amputation prostheses, after below knee amputation, is generally excellent.
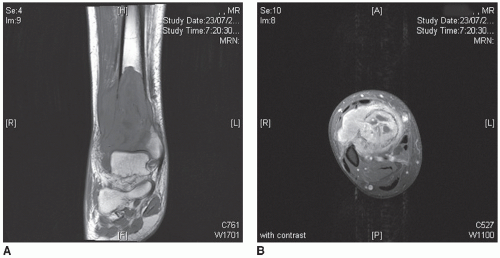 FIGURE 23.1 A: T1-weighted coronal MRI of a distal right tibial Ewing sarcoma in a 36-year-old male. Note the prominent lateral soft tissue component, which is a feature of this tumor and which may complicate a tumor of the lower leg because of the confined anatomy in this region. B: T2-weighted contrast-enhanced fat-suppressed axial magnetic resonance image of a distal right tibial Ewing sarcoma in a 36-year-old male. Extension of the soft tissue component anteriorly and along the interosseous membrane will compromise the anterior tibial neurovascular structures. |
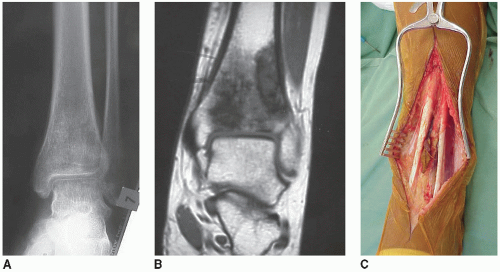 FIGURE 23.2 A: Anteroposterior radiograph of a distal tibial osteosarcoma characterized by a mixed sclerotic and lytic appearance. B: T1-weighted coronal magnetic resonance image demonstrates excellent soft tissue contrast and marrow definition. The tumor extends down to the articular margin and in this case has complicated the joint by invading it. C: Anterior incision to expose the tumor identified in (B). Note that the biopsy tract between tibialis anterior and extensor digitorum tendons has been isolated and left in continuity with the tumor. |
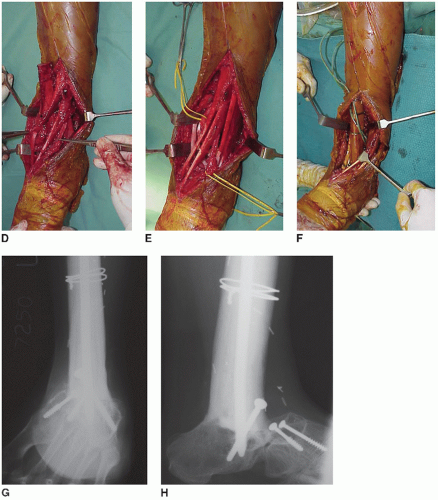 FIGURE 23.2 (Continued) D: The distal tibia and fibula have been osteotomized and the tumor specimen is being mobilized to be delivered to the medial side of tibialis anterior tendon. The extensor hallucis tendon and anterior tibial neurovascular structures, which are lateral to the anterior tibialis tendon, are indicated by the forceps. E: The tumor has been extracted and the major structures around the ankle are clearly visible. From left to right, tibialis posterior tendon (retracted), posterior tibial vessels and nerves (yellow sling), tibialis anterior tendon, extensor hallucis longus tendon, anterior tibial neurovascular structures, extensor digitorum longus tendons, and peroneus tertius tendon. F: Defect between calcaneus and tibia spanned by allograft arthrodesis. Anteroposterior (G) and lateral (H) radiographs at 8 years after allograft arthrodesis reconstruction. Reconstruction was supported by intramedullary rod fixation with supplementary interfragmentary screw fixation between the distal allograft and calcaneus. The navicular was fused to the cuneiform bones with interfragmentary screws. |
Metastatic carcinoma infrequently involves the distal tibia or tarsal bones. These lesions are either sclerotic, lytic, or a combination of these. Extraosseous extension of tumor may occur but typically is not as prominent as for primary malignancies, thus allowing local surgical treatment such as excisional curettage with maximal preservation of host bone (Fig. 23.4A-G). As with all metastatic diseases, if the diaphysis of the tibia is affected and there is a risk of development of other lesions, then protection of the entire bone with a durable construct should be planned.
 FIGURE 23.3 A: A 73-year-old male with chronic osteomyelitis following a distal tibial fracture sustained over 30 years previously. The sequestrum and involucrum are clearly visible on the oblique radiograph. B: The discharging sinus related to the chronic osteomyelitis is now complicated by extensive skin ulceration secondary to the development of a squamous cell carcinoma. C: T1-weighted fat-suppressed image with marked intramedullary tibial enhancement demonstrating significant marrow replacement after destruction of the overlying cortical bone. There is involvement of all three compartments of the leg and permeation of the carcinomatous change along the dermis and skin has occurred for a quite a distance from the epicenter of the ulcer. |
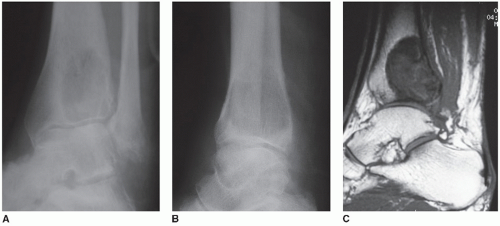 FIGURE 23.4 Anteroposterior (A) and lateral (B) plain radiographs of a melanoma deposit in a distal tibia. T1-weighted sagittal (C) and coronal. |
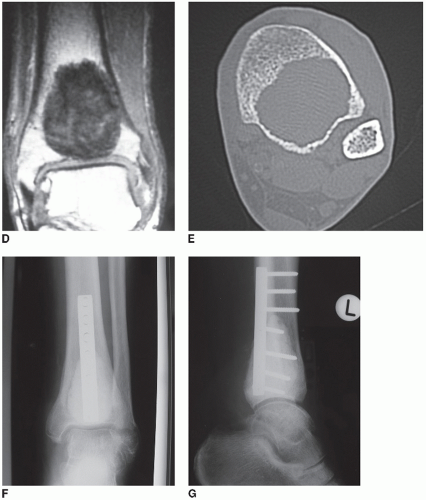 FIGURE 23.4 (Continued) (D) images showing an intramedullary lesion with minimal breach of the tibial cortex. The perimeter of the tumor is clearly visible with this sequence, which highlights the contrast between tumor and fatty marrow. E: Axial computed tomographic scan highlighting the excellent delineation of trabecular destruction with this imaging modality. F,G: Surgical treatment of an osseous melanoma deposit with curettage, cementation, and internal fixation. |
CONTRAINDICATIONS
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


