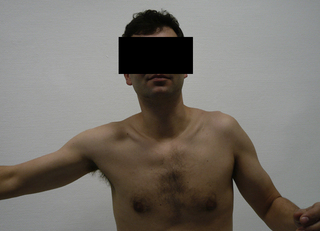
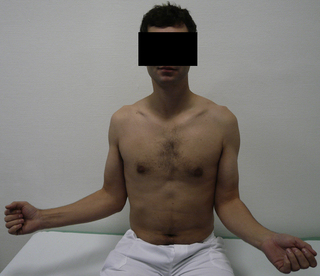
5.3 “Frozen shoulder” Frozen shoulder is a benign, independent disease which normally follows the same course. Diagnosis is made from the clinical symptoms. It was described as “frozen shoulder” by Codemann back in 1934 and as “adhesive capsulitis” by Neviaser in 1945, and these synonyms are both still used. A reduction in active and passive mobility is the predominant clinical symptom, accompanied by severe pain, depending on the stage. A distinction is made between the primary and secondary forms (Lundberg 1969). The causes of primary frozen shoulder are still unknown, although it is highly associated with diabetes mellitus or metabolic disorders. The underlying cause of secondary frozen shoulder is frequently a prior disease, injury, or operation in the area of the shoulder. In terms of clinical symptoms, both the primary and secondary forms progress in stages which can be divided into three phases. The term frozen shoulder covers diseases where the main symptom is active and passive restriction of movement. If the disease occurs without any evidence of any other cause, it is classed as primary or genuine frozen shoulder. This is generally understood as the cyclical picture of the disease of “capsular frozen shoulder” or “frozen shoulder” If a cause can be detected, however, which would in some way influence or provoke the limitation of movement of the shoulder joint, this is classed as a secondary form. This is where mechanical causes or e.g., glenohumeral arthritis can trigger immobilization, stiffness, or blocking of certain movements of the shoulder joint. Systemic causes can also favor the development of frozen shoulder, even if the association is not evident. The correct diagnosis is the most important step for primary frozen shoulder, where it is appropriate to rule out any other pathologies (Brue et al. 2007). The incidence of primary frozen shoulder is usually reported as 2–5% of the population Pal et al. 1986; (Hannafin & Chiaia 2000; Ricci et al. 2004), although many mild forms resolve without medical intervention. The incidence ranges from the ages of 40 to 70 years, and women are more commonly affected than men (Arslan & Celiker 2001). There is no prevalence of one side over the other (Bunker & Esler 1995). The chance of it occurring bilaterally is about 20–30% and a repeat occurrence of frozen shoulder once the patient has recovered from the disease is uncommon (Ogilvie-Harris & Myerthall 1997; Hannafin & Chiaia 2000). Over the years, many theories and possible associations have been described, but the etiology of primary frozen shoulder remains unknown. Bulgen et al. (1976) observed an increased occurrence of HLA-B27, although this was not substantiated in later studies (Miller et al. 1996). Bunker et al. examined cytokine expression, growth factors, and metalloproteinases with frozen shoulder and found slightly increased values compared to the healthy population and the Dupuytren collective. A lack of metalloproteinase MMP-14 was discovered, which is necessary for the activation of the proteolytically effective enzyme gelatinase A (Bunker et al. 2000). There is evidence from various working groups that the disease occurs more commonly with diabetes mellitus, where the risk of the disease is 10–19%, and with insulin-dependent diabetes mellitus even up to 36%. It is even possible that up to 42% of these patients can be affected on both sides. The course of frozen shoulder associated with diabetes is prolonged and incomplete regression with residual restriction of movement is reported (Bridgman 1972; Sattar & Luqman 1985; Fisher et al. 1986; Moren-Hybbinette et al. 1987). Lequesne et al. discovered a case of previously undiagnosed Type 1 diabetes among 60 patients with frozen shoulder (Lequesne et al. 1977). Other factors have been discussed, such as hyperthyroidism, autoimmune modulation, hormonal changes, and genetic predisposition (Hakim et al. 2003; Milgrom et al. 2008). Some authors suspect a correlation in connection with Dupuytren’s contracture in the hands (Bunker et al. 2000; Smith et al. 2001). Smith et al. found Dupuytren’s contracture at the same time in 52% of (frozen shoulder) patients examined and reported in the literature comparison an eight times higher occurrence of Dupuytren’s contracture. Ryu et al. found that in immunohistochemical tests in 11 operations for diabetic frozen shoulder there was an increase in neovascularization and an increased expressivity of vascular endothelial growth factor (VEGF) radiating from the synovia, and suspected a role in the pathogenesis (Ryu et al. 2006). The pathogenetic substrate of the disease is initially a diffuse synovitis and capsulitis in stage I, which then proceeds in stage II to capsular fibrosis with an increase in fibroblasts and myofibroblasts. The typical development of a hypertrophic and contracted capsule thus leads to a restriction of movement (Neer et al. 1992; Hannafin et al. 1994; Bunker 1997). Ozaki et al. saw a central change in the coracohumeral ligament and the rotator interval. With frozen shoulder, both structures are definitely contracted, thickened, and adherent, which is how they oppose the mobility of the head of the humerus in the socket (Ozaki et al. 1989). Hand et al. found typical cells of the chronic inflammation of proliferative fibrosis in histological and immunohistochemical tests of biopsy material gained from arthroscopies from the rotator interval due to arthrolysis; the evidence of T-cells and B-cells suggests an immune modulated pathology and mast cells may play an important role in the cellular regulatory mechanism between inflammation and fibrosis (Hand et al. 2007). In stage III, the capsular fibrosis is more or less completely dissolved again and the mobility of the head of the humerus improves once more. Arthroscopy of the shoulder brought new acroscopic impressions, so Neviaser & Neviaser (1987) described four stages: Stage II: Adhesive capsulitis and proliferative synovitis Stage III: Reduction of synovitis, reduced size of the axillary recess The duration of the disease, which is in principle self-limiting, is reported as taking about 4–6 months for each stage; the course of the disease has also been described as up to 10 years without complete restitutio ad integrum (Warner 1997). The typical characteristic of frozen shoulder is the active and passive restriction of glenohumeral mobility. Movement is limited in all directions in the most common form of primary or genuine capsular frozen shoulder. Clinical testing shows predominantly medial, abduction, and lateral rotation problems (Figs 5.3.1 and 5.3.2). Fig. 5.3.1 • Glenohumeral abduction disorder on the left with compensatory elevation of the shoulder due to frozen shoulder. Fig. 5.3.2 • Reduction of lateral rotation with the arm adducted on the left due to frozen shoulder. Systemic secondary forms show the same findings. Mechanical alterations often deviate from this guideline; depending on the causative mechanical disorder, there is then a different pattern of restricted movement. Secondary, noninflammatory causes are indicative of frozen shoulder if the clinically restricted range of movement is not pronounced to the same extent in all planes. A typical example is the so-called “bipolar” reduction in movement found in chronic rotator cuff lesions. After treatment of fractures or open procedures, combinations are often found with extensive subacromial growths, so the expression “subacromial adhesion syndrome” is often heard. When progress is idiopathic, the clinical course of the disease is almost standard in the three stages, although the duration of each phase is not predictable (Reeves 1975). In phase I (“freezing”), the main symptom is the pain. Patients report a sudden event without an accident and rapid progression, with pain at rest and sometimes particularly severe pain at night. The inflammatory change to the joint capsule takes place. This is accompanied by a reduction in mobility (lateral rotation, abduction, medial rotation). The glenohumeral stiffness is initially scapulothoracically compensated, then is later demonstrated by abduction when lifting the shoulder. The time for this varies from a few weeks to several months (Murnaghan 1990; Bunker & Anthony 1995). The transition into phase II is blurred and is characterized by a regression in the pain, although the active and passive concentric stiffness remains and the shoulder is “frozen” The inflammatory process of the capsule is burnt out. Patients now report no pain at rest. Clinical examination shows the typical movement restrictions, often with a fixed stop at the end of the range of movement, although the examination may be almost pain free. In phase III (“thawing”), the stiffness is released and remobilization and release of restriction slowly take place. Here, too, the overall duration cannot be predicted. The self-healing tendency of secondary frozen shoulder is significantly less by comparison (Habermeyer & Agneskirchner 2002). If mechanical disorders are present, these do not disappear spontaneously and can only be eliminated by active therapy.
Introduction
Determining the concept and classification
Epidemiology
Etiology and pathogenesis
Clinical symptoms
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


