4 Fractures of the Femur
Overview
 Anatomic Features
Anatomic Features
The femur is the longest and largest tubular bone in the human skeleton; the average length of an adult femur is 42.48 cm on the left side and 42.39 cm on the right side. The femur is cylindric in the upper third of its length, with the pectineal line running through the posterome-dial surface of the femur, up to the base of the lesser trochanter. The pectineal line then continues with the intertrochanteric line, and down to the medial lip of the linea aspera. The gluteal tuberosity lies on the posterolateral aspect of the femur, up to the base of the greater trochanter and down to the lateral lip of the linea aspera. The middle part of the femur is slightly twisted and curved, with an anterior convexity that is 30° rotated from the superolateral to inferomedial part of the femur. The lower third of the femur becomes flattened and widened anteroposteriorly. The linea aspera on the dorsal side of middle third has two lips that diverge and turn into the medial and lateral supracondylar ridge, respectively. The rough impression above the medial epicondyle gives origin to the medial head of the gastrocnemius, while the plantaris arises in the impression above and to the medial side of the lateral epicondyle (Plate 4.1).
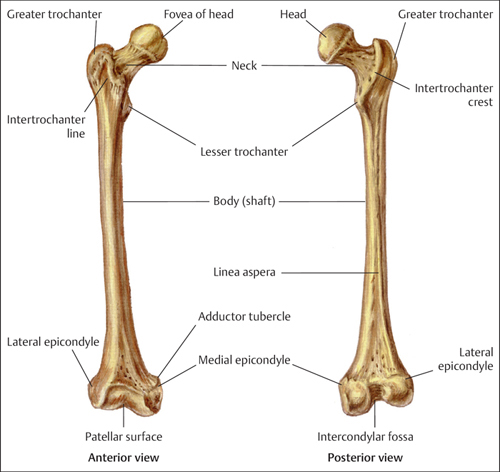
Plate 4.1
 AO Classification and Coding System for Femur Fractures
AO Classification and Coding System for Femur Fractures
Based on the AO classification, femur fracture is coded as number “3.” According to “Heim’s square,” the anatomic delineation of the proximal and distal shaft is number “31, 32, and 33,” respectively (Plates 4.2 and 4.3).
 Clinical Epidemiologic Features of Femur Fractures
Clinical Epidemiologic Features of Femur Fractures
A total of 7660 patients with 7756 femoral fractures were treated at our trauma center over a 5-year period from 2003 to 2007. All cases were reviewed and statistically studied; the fractures accounted for 12.71% of all patients with fractures and 11.88% of all types of fractures, respectively. Among these 7660 patients, 697 were children with 701 fractures, and 6963 were adults with 7055 fractures.
Epidemiologic features of femur fractures are as follows:
• more males than females
• more left-side than right-side injuries
• the highest-risk age group is 31–40 years. The most affected male age group is 31–40 years, while females aged 71–80 years have the highest risk
• the proximal femur fracture is the most common femur fracture.
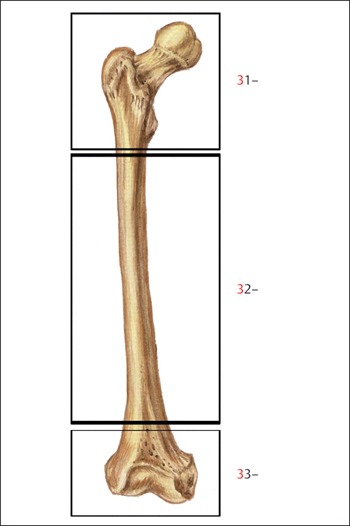
Plate 4.2
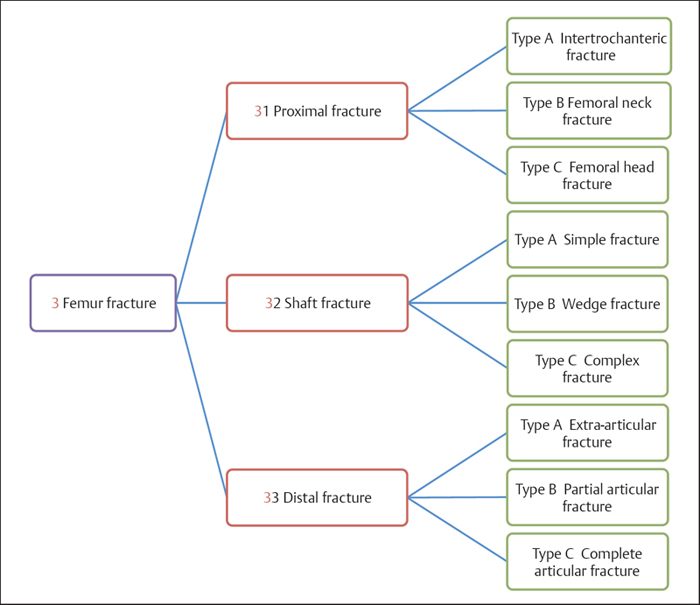
Plate 4.3
 Femur Fractures by Sex
Femur Fractures by Sex
Table 4.1 Sex distribution of 7660 patients with femur fractures
| Sex | Number of patients | Percentage |
| Male | 4936 | 64.44 |
| Female | 2724 | 35.56 |
| Total | 7660 | 100.00 |
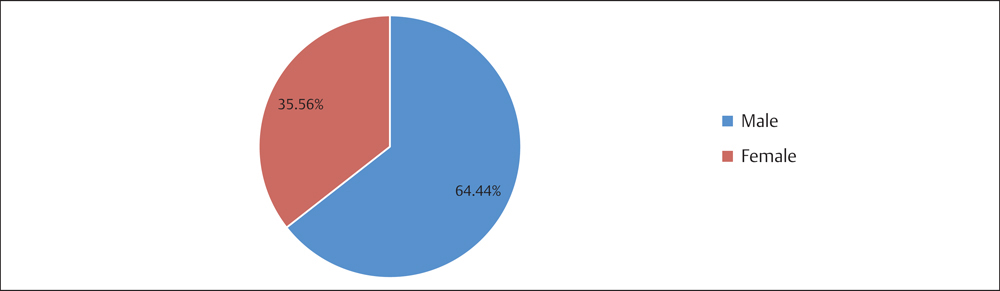
Fig. 4.1 Sex distribution of 7660 patients with femur fractures.
 Femur Fractures by Injury Side
Femur Fractures by Injury Side
Table 4.2 Injury side distribution of 7660 patients with femur fractures
| Injured side | Number of patients | Percentage |
| Left | 4041 | 52.75 |
| Right | 3562 | 46.50 |
| Bilateral | 57 | 0.74 |
| Total | 7660 | 100.00 |
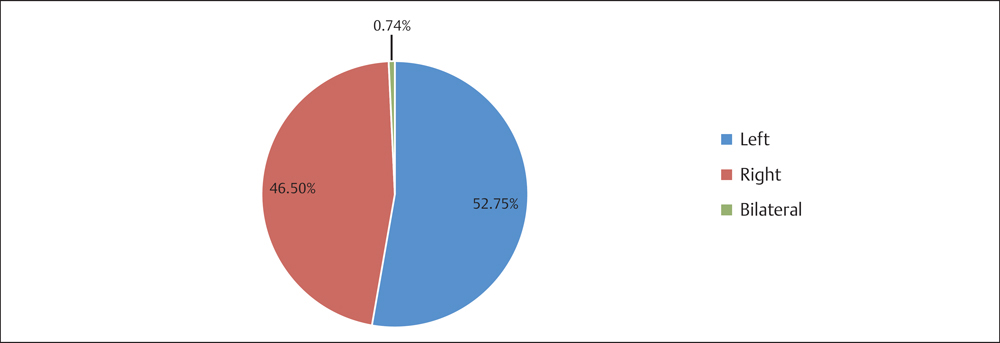
Fig. 4.2 Injury side distribution of 7660 patients with femur fractures.
 Femur Fractures by Age Group
Femur Fractures by Age Group
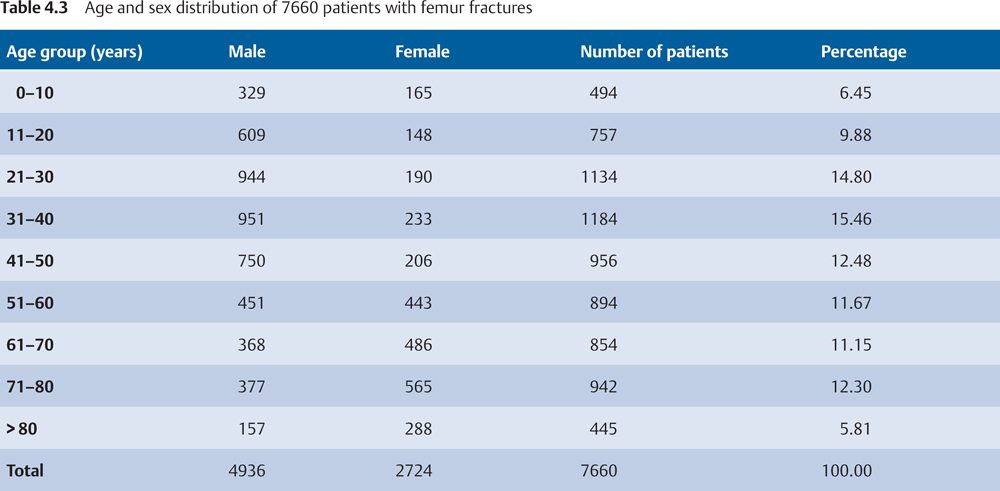
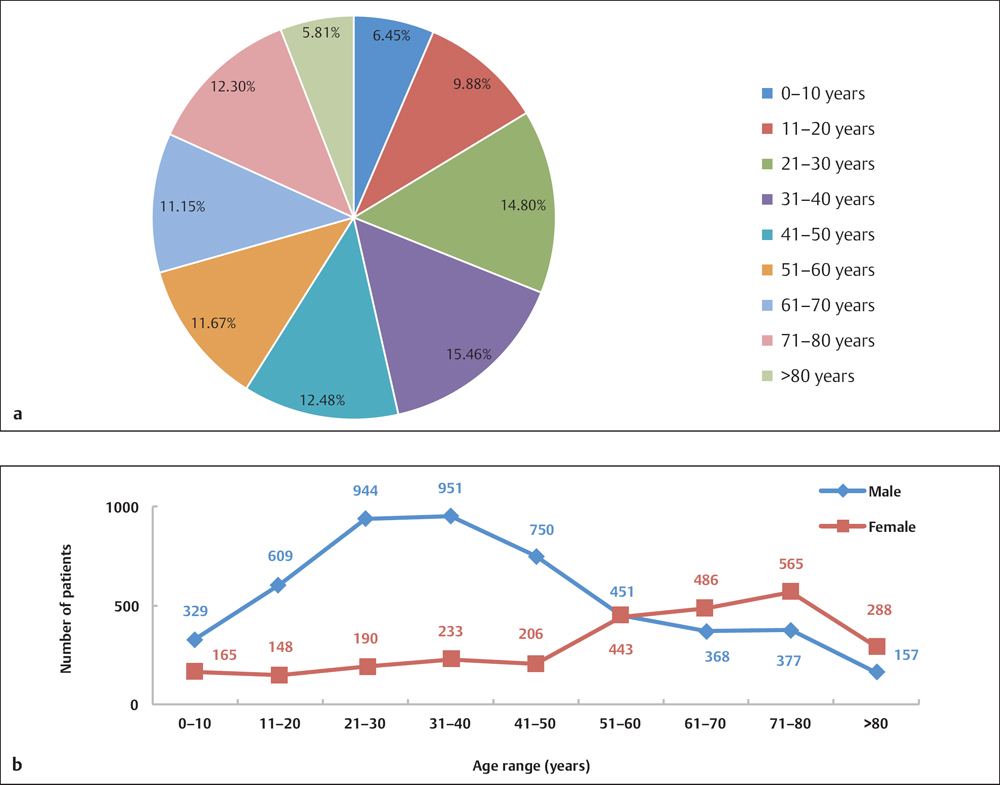
Fig. 4.3 a, b
a Age distribution of 7660 patients with femur fractures.
b Age and sex distribution of 7660 patients with femur fractures.
 Femur Fractures by Fracture Segment
Femur Fractures by Fracture Segment
 Segment Distribution of Femur Fractures in Adults Based on AO Classification
Segment Distribution of Femur Fractures in Adults Based on AO Classification
Table 4.4 Fracture segment distribution of 7055 femur fractures in adults based on AO classification
| Segment | Number of fractures | Percentage |
| 31 (proximal) | 3829 | 54.27 |
| 32 (diaphysis) | 2559 | 36.27 |
| 33 (distal) | 667 | 9.45 |
| Total | 7055 | 100.00 |
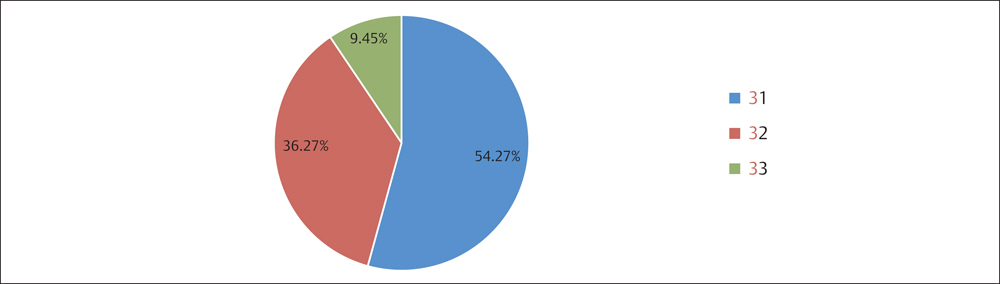
Fig. 4.4 Segment distribution of 7055 adult femur fractures based on AO classification.
 Segment Distribution of Femur Fractures in Children
Segment Distribution of Femur Fractures in Children
Table 4.5 Segment distribution of 701 femur fractures in children
| Segment | Number of fractures | Percentage |
| Proximal | 119 | 16.98 |
| Diaphysis | 519 | 74.04 |
| Distal | 63 | 8.99 |
| Total | 701 | 100.00 |
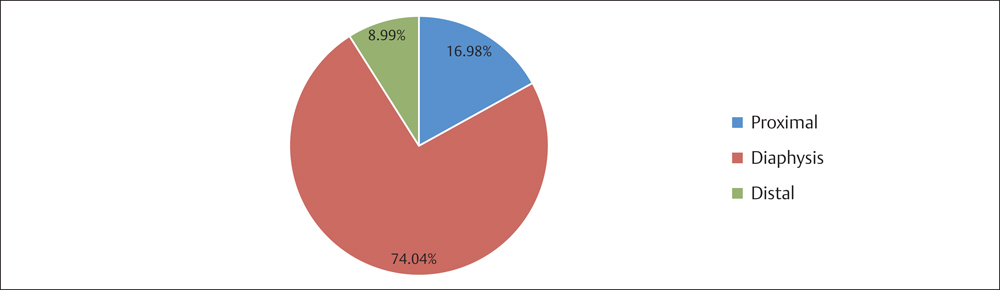
Fig. 4.5 Segment distribution of 701 femur fractures in children.
Proximal Femur Fractures (Segment31)
 Anatomic Features
Anatomic Features
The head of the femur is globular in shape and forms about two-thirds of a sphere (Plate 4.4). The neck projects forward to some extent, with an average anterior projection of 10–15°. Flattened posteriorly, the neck is contracted in the middle, which is often the site of fractures. In adults, the neck forms an angle of ~ 120–130° with the body. At the junction of the neck with the upper part of the body, there is a large eminence called the greater trochanter. A smaller eminence projecting from the lower and posterior part of the base of the neck is called the lesser trochanter. Running obliquely downward and medial from the tubercle is the intertrochanteric line, while the intertrochant-eric crest courses obliquely downward and medially from the summit of the greater trochanter on the posterior surface of the neck.
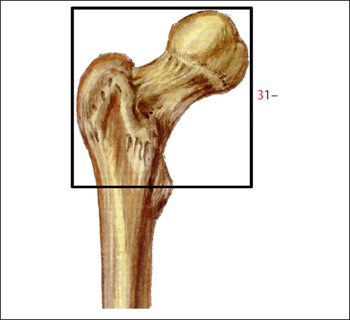
Plate 4.4
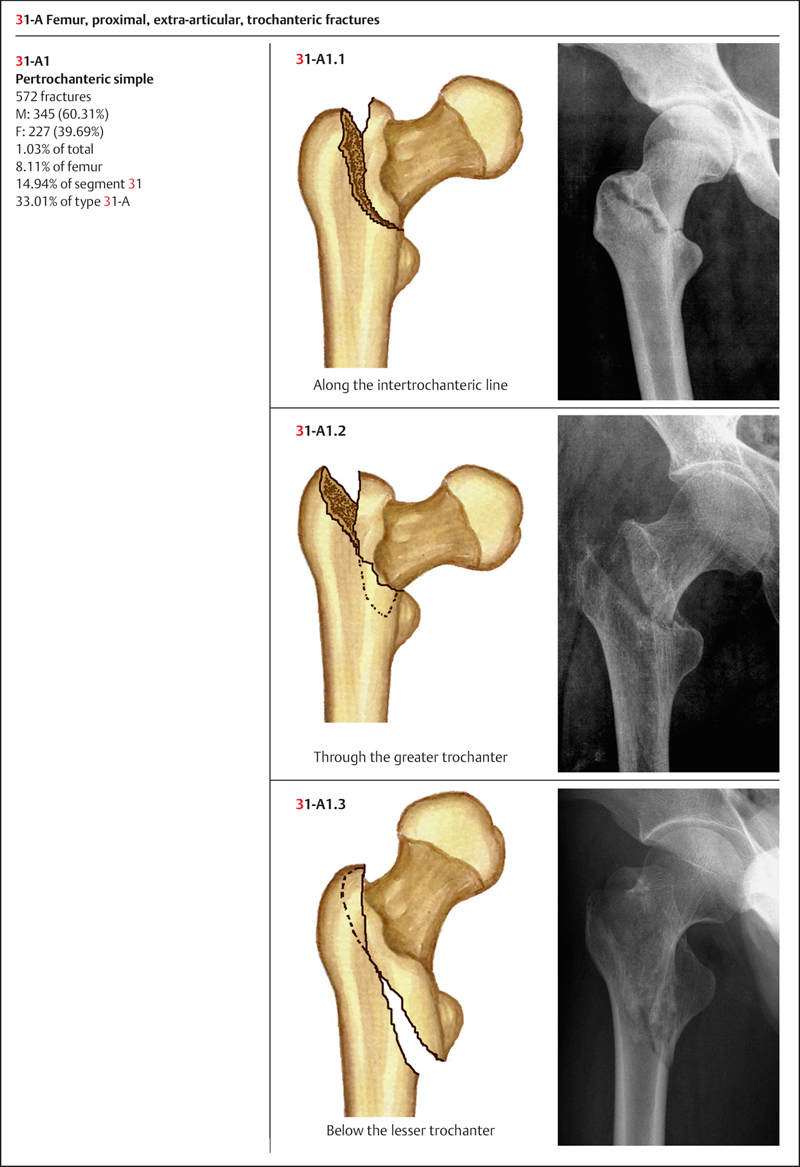
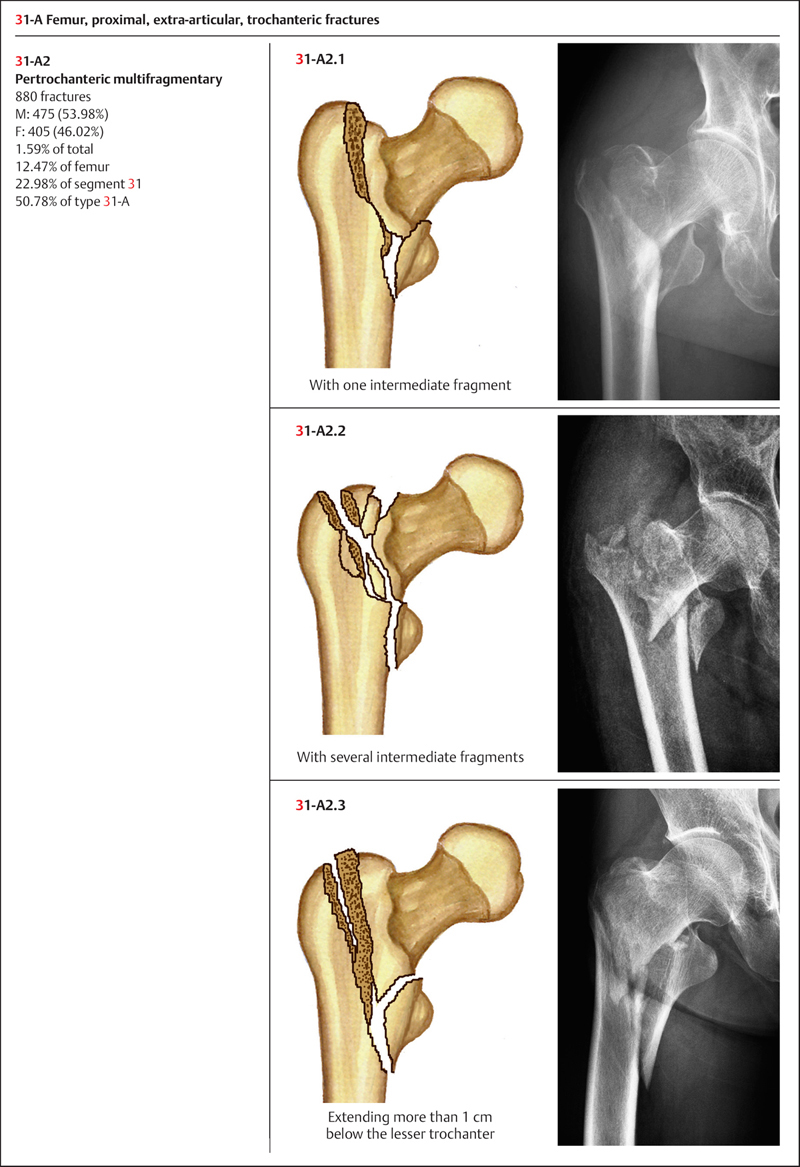
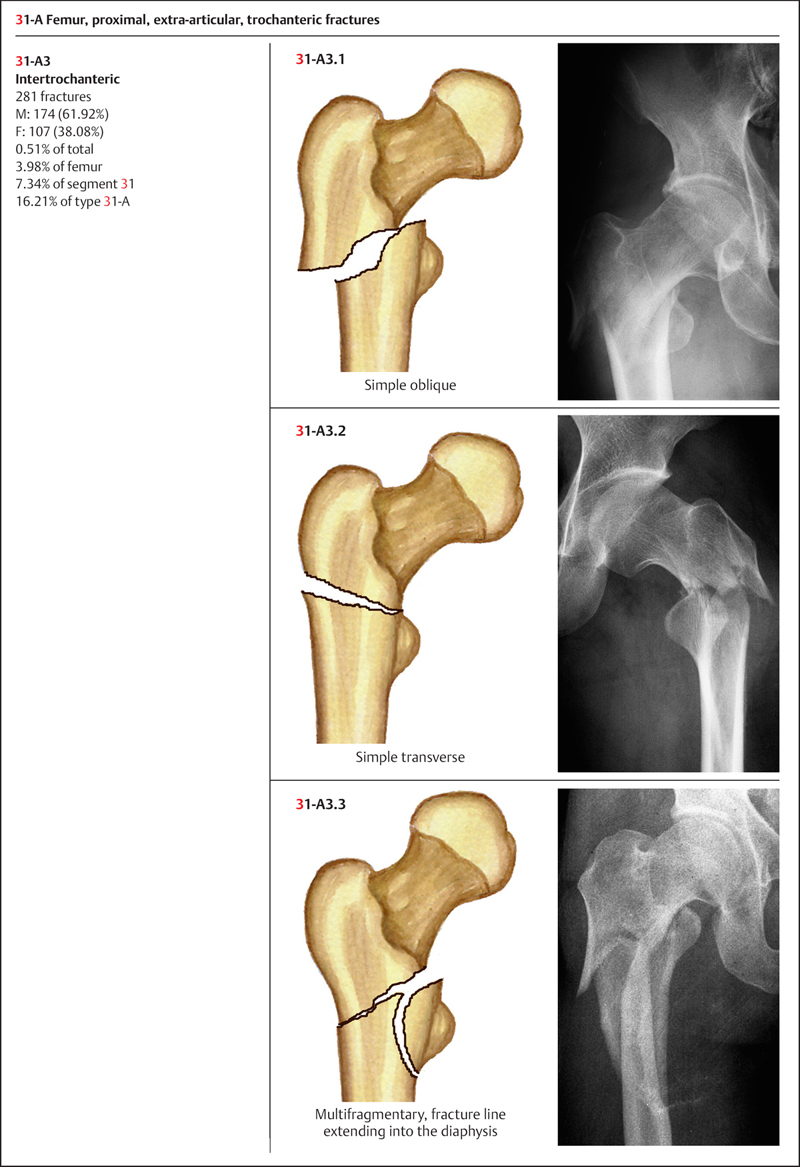
 AO Classification of Proximal Femur Fractures
AO Classification of Proximal Femur Fractures
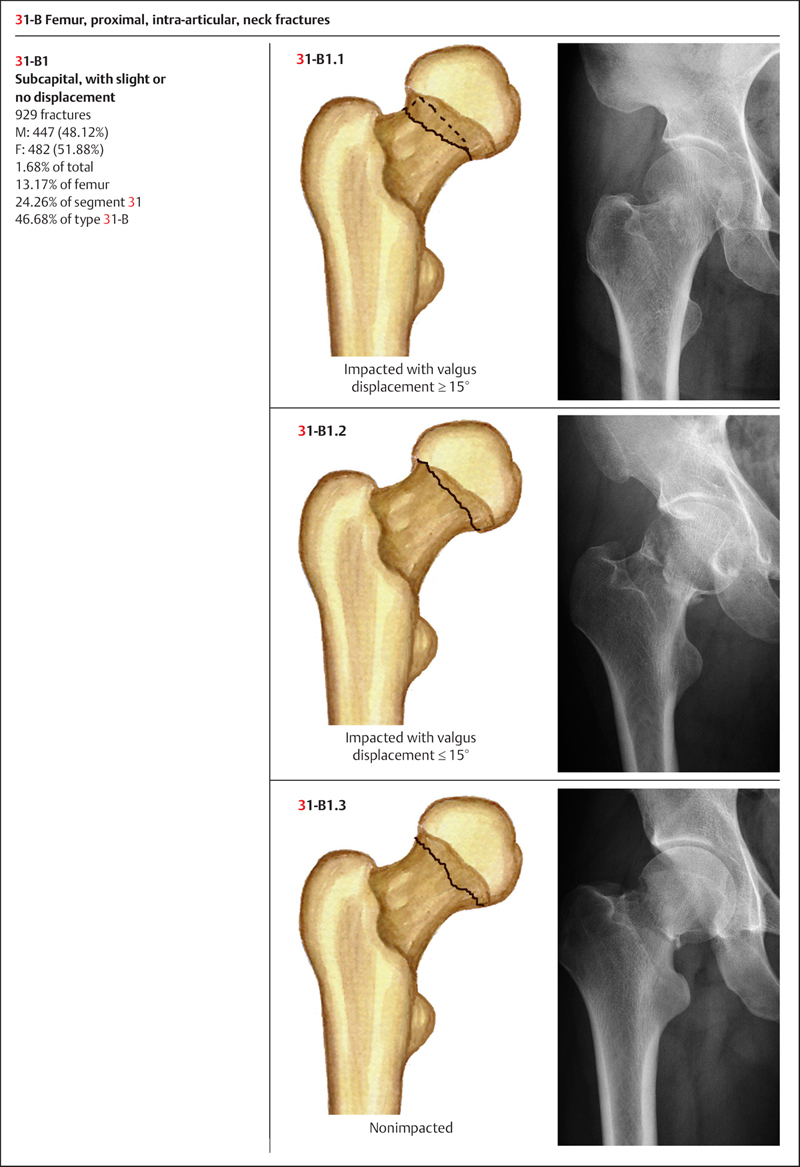
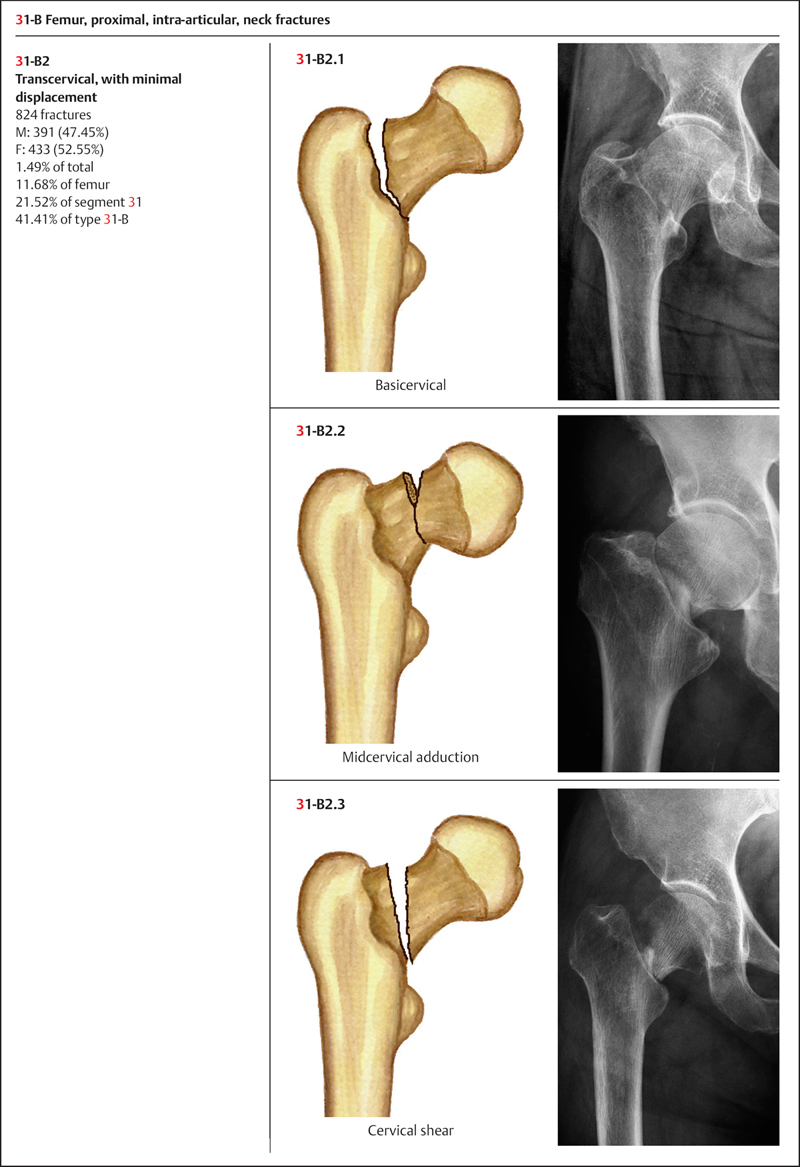
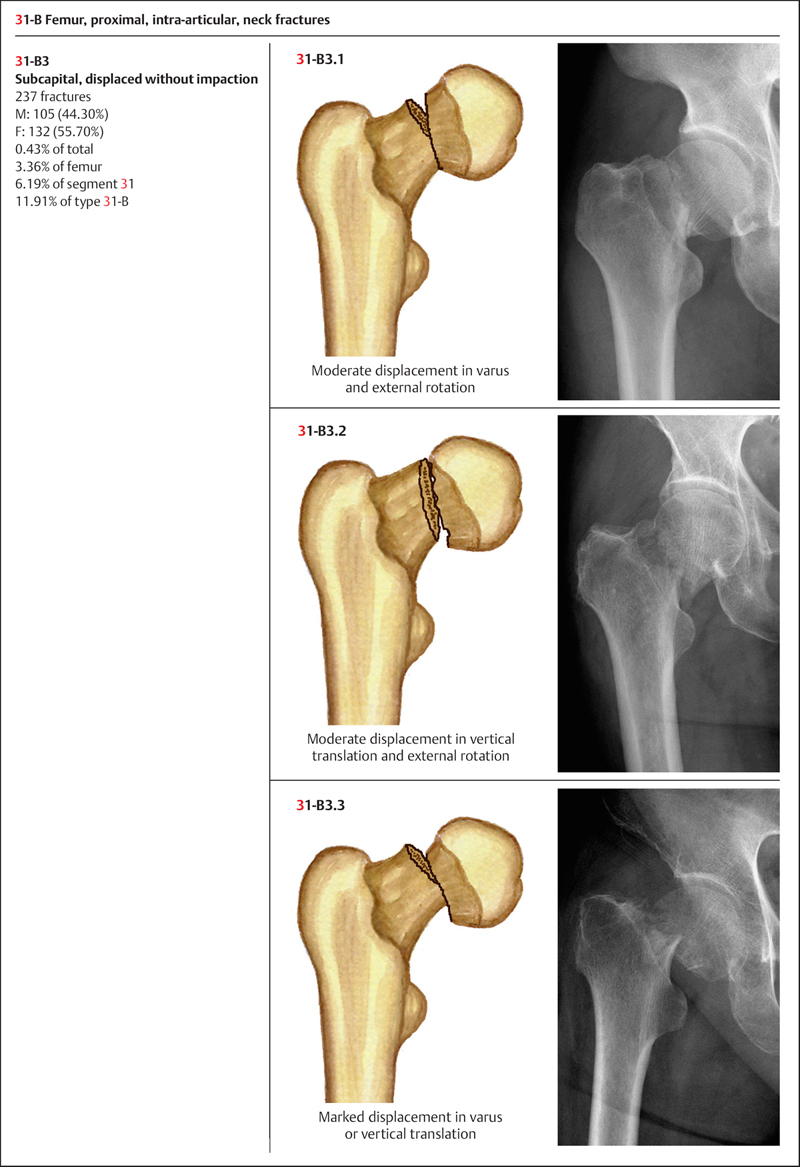
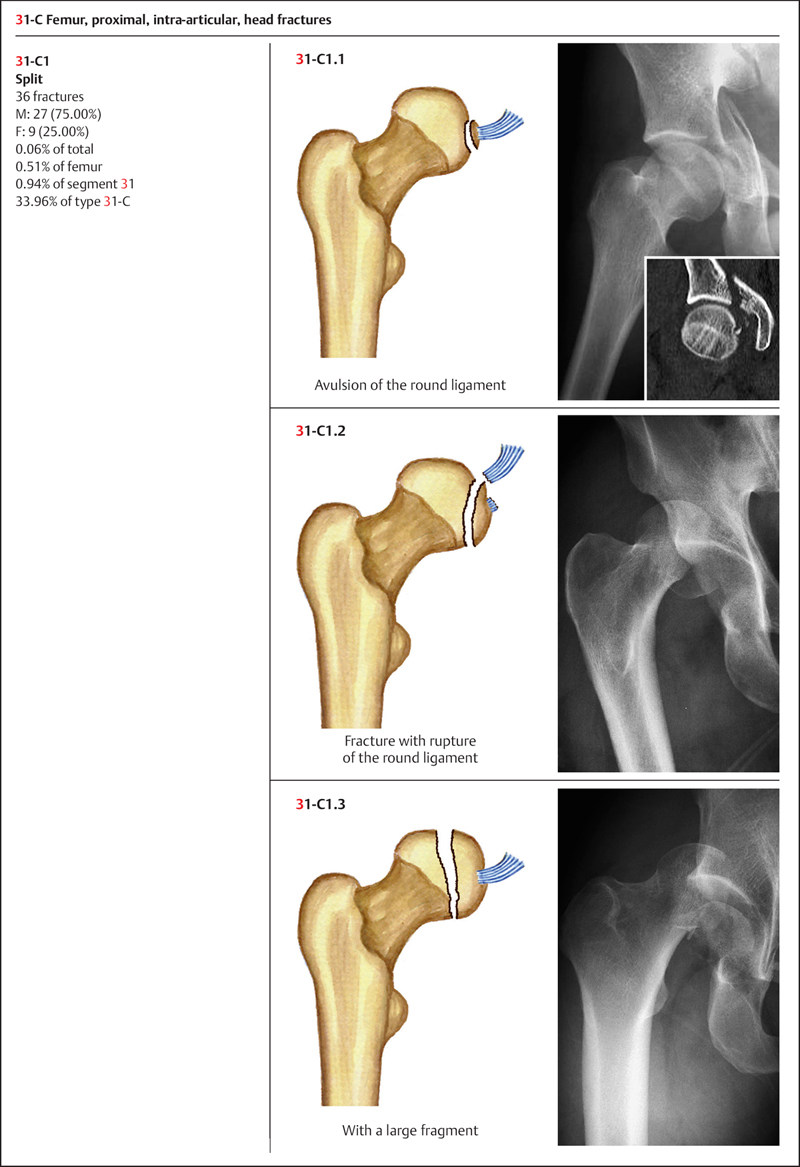
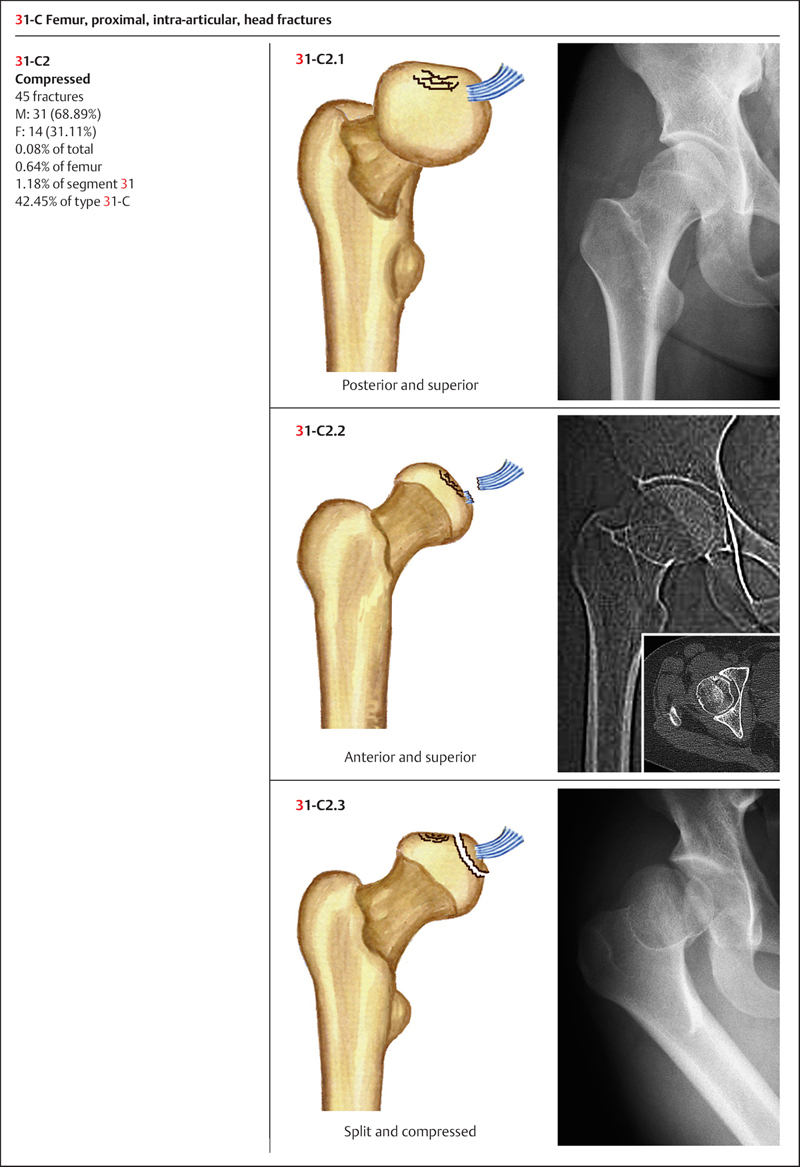
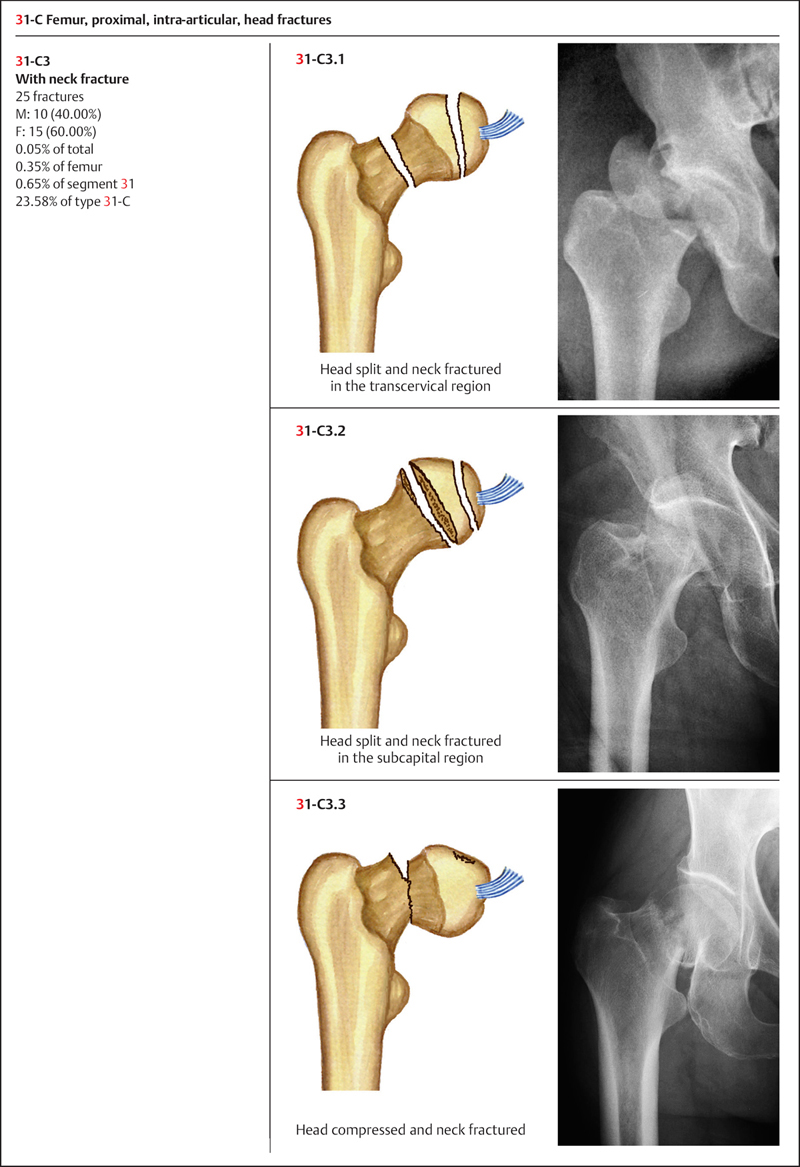
Based on AO classification, the proximal femur is coded as the number “31.” It is further divided into three types: 31-A: trochanteric fracture (extra-articular); 31-B: femur neck fracture (articular); 31-C: femur head fracture (intra-articular) (Plate 4.5).
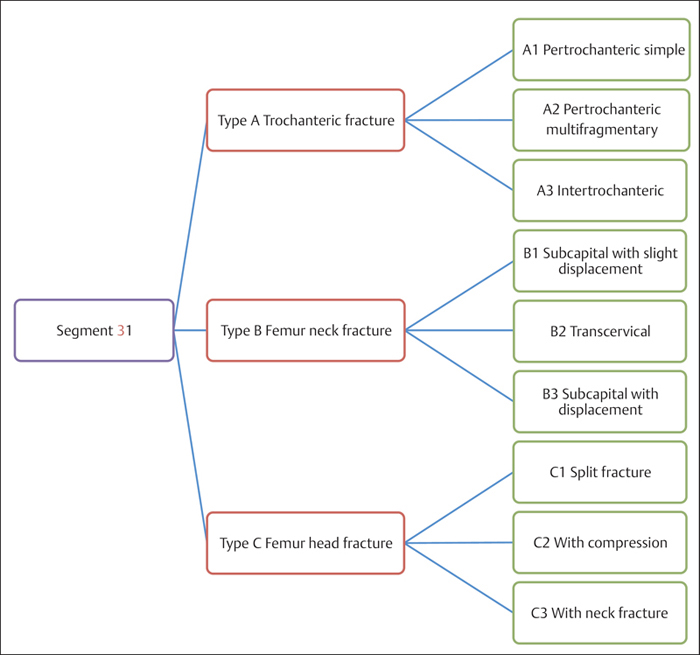
Plate 4.5
 Clinical Epidemiologic Features of Proximal Femur Fractures (Segment 31)
Clinical Epidemiologic Features of Proximal Femur Fractures (Segment 31)
A total of 3829 adult proximal femur fractures were treated at our trauma center over a 5-year period from 2003 to 2007. All cases were reviewed and statistically studied; the fractures accounted for 54.27% of femur fractures in adults. Their epidemiologic features are as follows:
• more males than females
• the highest-risk age group for both sexes is 71–80 years
• the most common fracture type among segment 31 fractures is type 31-B. However, 31-A is more common in males, while 31-B is more common in females
• the most common fracture group among segment 31 fractures is group 31-B1. However, group 31-A2 most commonly occurs in males, while group 31-B1 is most prevalent in females.
 Fractures of Segment 31 by Sex
Fractures of Segment 31 by Sex
Table 4.6 Sex distribution of 3829 fractures of segment 31
| Sex | Number of fractures | Percentage |
| Men | 2005 | 52.36 |
| Women | 1824 | 47.64 |
| Total | 3829 | 100.00 |
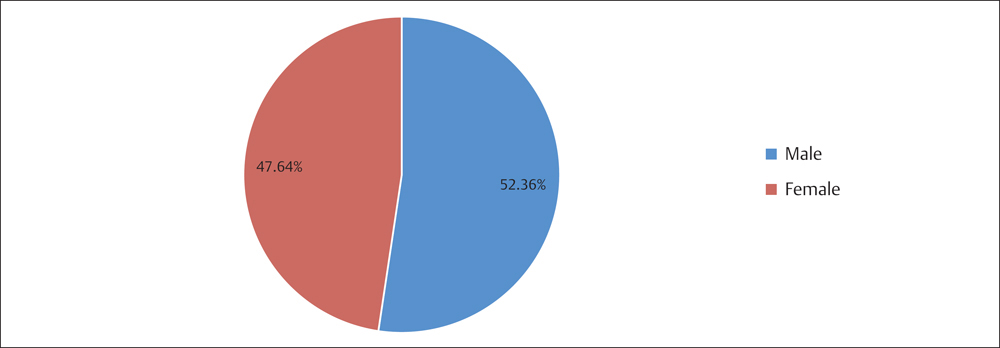
Fig. 4.6 Sex distribution of 3829 fractures of segment 31.
 Fractures of Segment 31 by Age Group
Fractures of Segment 31 by Age Group
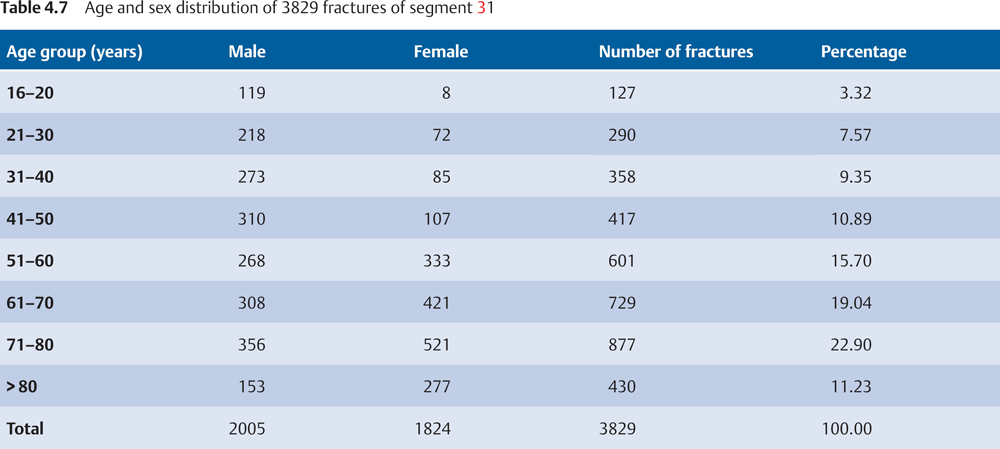
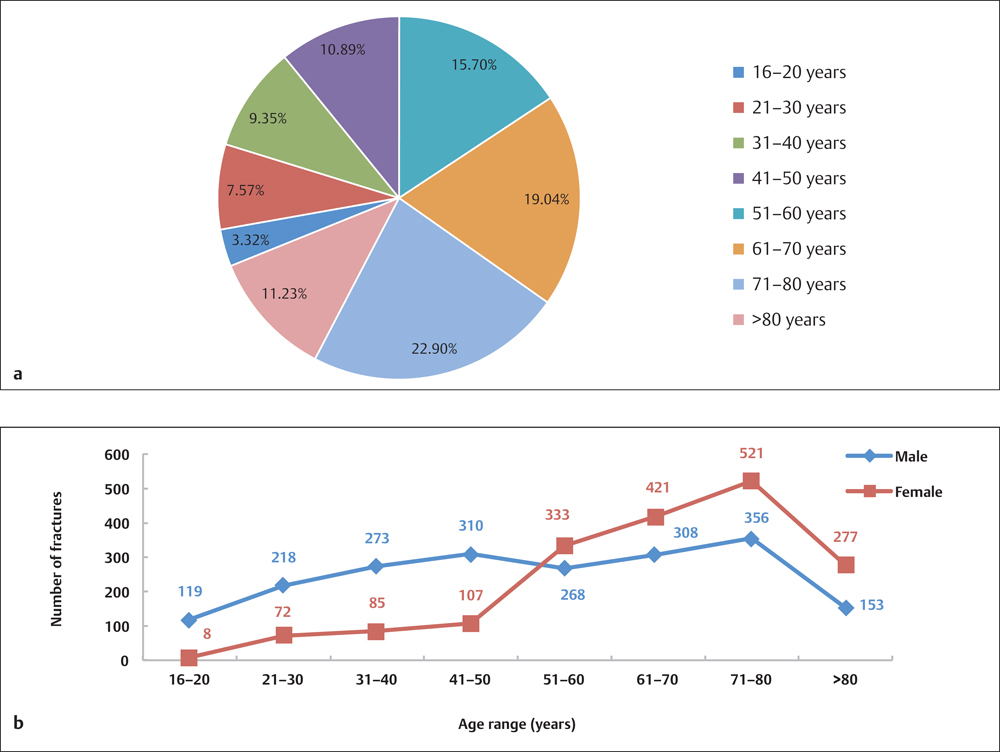
Fig. 4.7 a, b
a Age distribution of 3829 fractures of segment 31.
b Age and sex distribution of 3829 fractures of segment 31.
 Fractures of Segment 31 by Fracture Type
Fractures of Segment 31 by Fracture Type
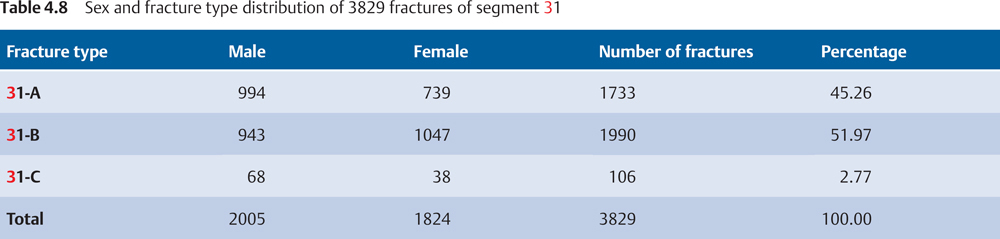
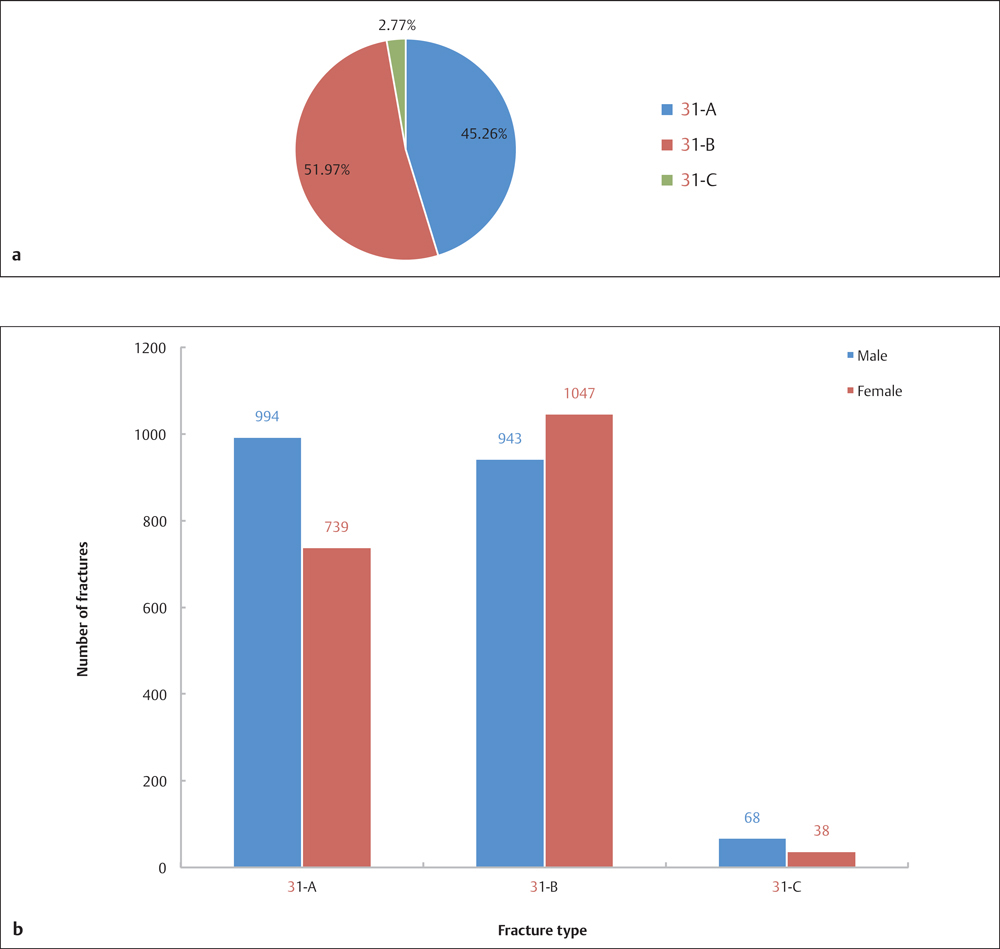
Fig. 4.8 a, b
a Fracture type distribution of 3829 fractures of segment 31.
b Sex and fracture type distribution of 3829 fractures of segment 31.
 Fractures of Segment 31 by Fracture Group
Fractures of Segment 31 by Fracture Group
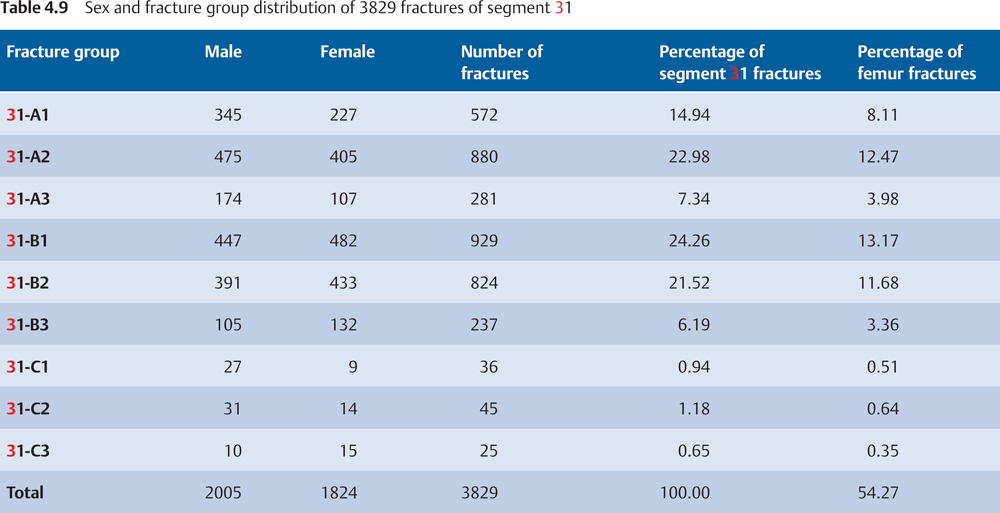

Fig. 4.9 a, b
a Fracture group distribution of 3829 fractures of segment 31.
b Sex and fracture group distribution of 3829 fractures of segment 31.
 Injury Mechanism
Injury Mechanism
Intertrochanteric fracture can be caused by a direct force applied perpendicularly to the trochanteric area, or an indirect varus force transmitted to the intertrochanteric area through the hip. The forceful contraction of the gluteus medius and gluteus minimus muscles, or having the lower limb in hyperadduction, may lead to an avulsion fracture of the greater trochanter, while the pull of the iliopsoas muscle may result in avulsion of the lesser trochanter. Intertrochanteric fractures often occur in the elderly, mostly caused by falls. Since elderly patients often have osteoporotic bones, the resulting fractures are frequently complex fractures.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


