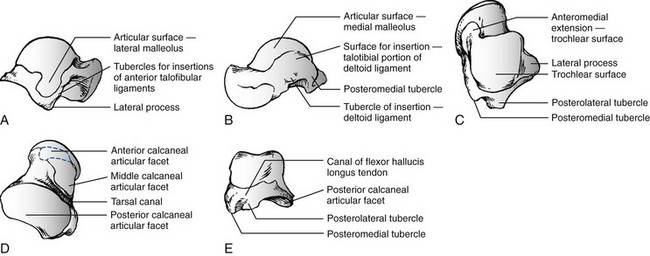
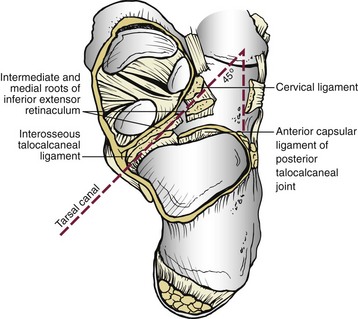
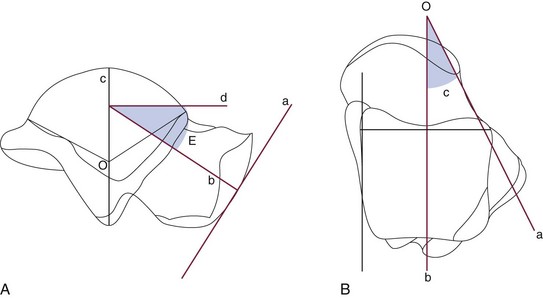
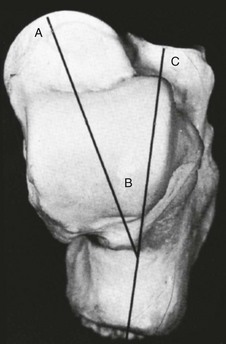
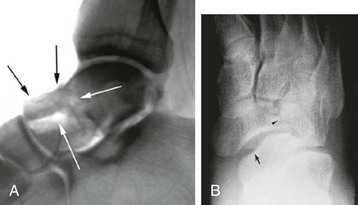
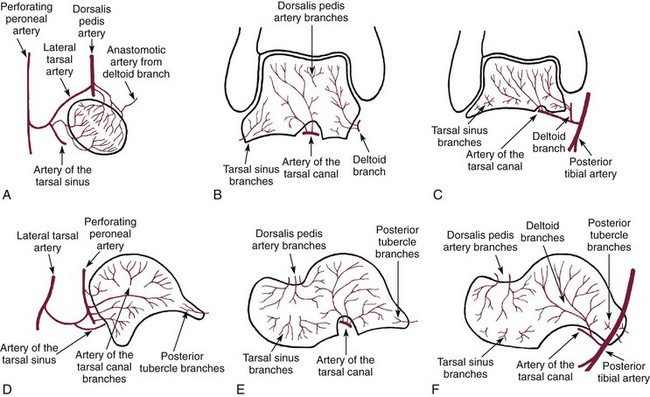
Chapter 39 TOTAL DISLOCATION OF THE TALUS SUBTOTAL DISLOCATION OF THE TALUS (SUBTALAR OR PERITALAR) COMPLICATIONS ASSOCIATED WITH FRACTURES OF THE TALAR NECK AND BODY FRACTURES OF THE POSTERIOR PROCESS FRACTURES OF THE POSTEROLATERAL TUBERCLE FRACTURES OF THE POSTEROMEDIAL TUBERCLE FRACTURES OF THE LATERAL PROCESS The talus has been referred to as “the universal joint of the foot” because of its multiple articulations.24 Fractures of the talus are uncommon, accounting for approximately 1% of all fractures, and are frequently the result of high-energy trauma, such as motor vehicle collisions and falls from height.132 The terms talus and astragalus date back to the pre-Christian era and relate to the manufacture of dice. The modern word talus comes from the Old French talo, meaning ankle, and originates in the Latin word for dice, or taxillus, because the Romans made their dice from the heel bone of a horse.144 The Greeks, on the other hand, made their dice from the second cervical vertebra of the sheep. The word for this vertebra in Greek is astragalus. Coltart24 credits Fabricius of Hilden41 with the first account of an injury to the talus in 1608. This complete dislocation was treated with talectomy. Astley Cooper26 first described the natural history of dislocation of the talus in 1818. In 1848, James Syme154 reported that of 13 patients admitted to the Royal Infirmary of Edinburgh with compound fracture-dislocation of the talus, only two survived. Therefore he recommended below-knee amputation for these injuries, a procedure that still produced a mortality rate of 25% in his era. In 1909, Stealy149 reviewed the literature to that date and noted a 50% mortality rate after open fracture-dislocation of the talus. Anderson,3 while serving as consultant surgeon to the Royal Flying Corps in 1919, reported on 18 cases of fracture-dislocation of the talus. Because parachutes were not in use at this time, pilots went down with their aircraft. Anderson identified the mechanism of injury as a hyperdorsiflexion force exerted on the sole of the foot by the rudder bar of the aircraft on impact and coined the term “aviator’s astragalus” for this injury because of its occurrence in belly landings of small aircraft.117 In 1952, in an excellent and detailed review, Coltart24 described 228 injuries of the talus that he collected from the Royal Air Force records during the World War II. This is the largest series ever reported and included 106 fractures or fracture-dislocations of the talar neck. In 1970, Hawkins66 suggested a classification of vertical fractures of the talar neck. This classification was based on the roentgenographic appearance of the fracture at the time of injury, and Hawkins divided these fractures into three groups. The significance of this classification was its prognostic value with respect to avascular necrosis (AVN). Since that time, a plethora of publications have documented a variety of problems associated with vertical fractures of the talar neck, including AVN, nonunion, malunion, infection, arthritis, and bone loss. Injuries to the talus are serious because this bone is the critical link between the subtalar, transverse tarsal, and ankle joint complex.134 The variety of coupled actions occurring from the motion of this bone or surrounding bones permit the effortless flexibility of the hindfoot and midfoot. If the talus is damaged, the universal combined motion of the foot and ankle becomes compromised, and severe disability can result. The talus is the second largest tarsal bone and has five articular surfaces, all of which have a weight-bearing function (Fig. 39-1). Two thirds of the talar surface is covered with articular cartilage, and neither tendons nor muscles insert or originate from this bone.134 The talus is composed of three parts—the head, neck, and body—and two processes—the lateral and posterior. The head is the portion that articulates mostly with the navicular. The body includes the dome of the talus at the ankle joint and the posterior facet at the subtalar joint. Between the head and the body is the neck, which does not articulate with the ankle and sits over the sinus tarsi below. The body and neck of the talus are not coaxial because, in the horizontal plane, the neck angles medially with a variable angle of declination.134 The head of the talus is the distal portion that nests within an articulation known as the acetabulum pedis, or foot socket, as described by Sarrafian135 (Fig. 39-2). This socket is formed by the calcaneal middle and anterior surfaces, connected to the large navicular articular surface by the inferior and superomedial calcaneonavicular ligaments. The acetabulum pedis has a variable volume capacity and adapts to the changing position of the talar head during gait. It is hinged laterally by the lateral calcaneonavicular component of the bifurcate ligament and medially by the posterior tibial tendon and the spring ligament.135 The anteroinferior medial portion of the talar head is quadrilateral or oval and provides articulation with the anterior facet of the calcaneus. This portion of the head is flat and continuous anteriorly with the navicular articular surface. The neck of the talus has four surfaces: superior, lateral, medial, and inferior and is one of the few areas of the talus not covered by articular cartilage. The superior surface of the neck is limited posteriorly by the anterior border of the trochlea of the talus (the dome or body) and anteriorly by the articular surface of the talar head. The talotibial capsule inserts along this superior surface just proximal to the insertion of the capsule of the talonavicular joint. The lateral surface of the neck provides an insertion for the medial aspect of the inferior extensor retinaculum.134 The lateral cortex of the talar neck is concave and flares as it approaches the lateral cortex. The inferior surface of the neck forms the roof of the sinus tarsi and sinus canal and is the insertion point for the talocalcaneal ligament, a major stabilizer of the subtalar joint. The mildly convex medial surface provides an area for insertion of the talonavicular ligaments. The talar neck is angled at a mean of 24 degrees medially (range, 10-44 degrees) and plantarly (range, 5-50 degrees), and it is the portion of the talus most vulnerable to fracture (Fig. 39-3).134 The body of the talus is arbitrarily divided into five surfaces: lateral, medial, superior, inferior, and posterior. The lateral surface consists of a large articular surface, the facies malleolaris lateralis, which articulates with the distal fibula.134 Along the anterior, inferior, and posterior perimeter of this lateral articular surface is the lateral process, a nonarticular component of the talus. The lateral talocalcaneal ligament inserts at the inferior tip of the lateral process. Along the anterior border of the triangular lateral process are two tubercles for insertion of the anterior talofibular ligament. Along the posteroinferior border of this lateral surface lies a groove for the attachment of the posterior talofibular ligament. The medial surface of the body presents two areas: superior and inferior. The superior portion is occupied by the articular facet, or facies malleolaris medialis. This articular surface is shaped like a comma, with the long axis oriented anteroposteriorly. The inferior portion is nonarticular, and its anterior half is a depressed surface perforated by numerous vascular foramina. Under the tail of the superior surface, the posterior half of the inferior portion consists of a large oval area that provides insertion for the deep component of the deltoid ligament.134 The inferior surface of the talar body consists of the facies articularis calcanea posterior tali.134 This articular surface is quadrilateral and is concave in the long axis and flat transversely. It articulates with the posterior facet of the calcaneus (Fig. 39-4). The posterior surface of the talar body consists of posterolateral and posteromedial tubercles that flank the sulcus for the flexor hallucis longus tendon. The posterolateral tubercle is larger and more prominent than the posteromedial tubercle. The posterolateral tubercle contributes an inferior articular surface that is in continuity with the posterolateral aspect of the posterior calcaneal surface of the talus. The posterolateral tubercle may appear as an oversized trigonal process known as the Stieda process or as a separate accessory bone, the os trigonum, which is seen in approximately 3% to 8% of the population.55,134 The blood supply to the talus has been studied in great detail because of the incidence of AVN after fractures and dislocations (Fig. 39-5). Although early reports indicated poor vascular flow, more recent investigators note the presence of an extensive extraosseous and intraosseous blood supply to the talus.59,110 However, because most of the talar surface is covered with articular cartilage and no muscles originate or insert into this bone, the areas available for vessels to enter are few.59,76,110 Fractures or dislocations of the talus are often associated with disruptions in the blood supply and thus pose potential problems for the healing and integrity of the talus. Figure 39-5 Vascular anatomy of talus. A to C, Coronal sections. D to F, Sagittal sections. A, Head. B, Middle third. C, Posterior third. D, Lateral talus. E, Middle talus. F, Medial talus. (Reproduced with permission and copyright of the British Editorial Society of Bone and Joint Surgery: Mulfinger GL, Trueta J: The blood supply of the talus. J Bone Joint Surg Br 52:160-167, 1970. [Figures 1a, 1b, 1c and 2a, 2b, 2c]) The extraosseous arteries to the talus include branches from the posterior tibial, dorsal pedis/anterior tibial artery, and peroneal arteries. In addition, these vessels anastomose to form several vascular networks that surround and supply blood to the talus.59,76,110,140 According to Wildenauer,166 the talar vascular supply arising from these three main arteries reaches the talus through a vascular network that covers all its cartilage-free surfaces. Although all three arteries provide some supply to the talus, the relative importance of each artery has been studied and debated. Earlier studies suggested that the main blood supply was from the anterior tibial artery.110,123 Others have suggested that the contribution of the posterior tibial artery provides the main blood supply to the talus.47,59 Most recently, Miller et al105 studied the blood supply of the talus using gadolinium enhanced magnetic resonance imaging (MRI) and demonstrated that the greatest contribution of the blood supply (47%) comes from the posterior tibial artery. The posterior tibial artery supplies the talus through two branches. First, the posterior tibial artery gives rise to the artery of the tarsal canal (see following discussion). About 5 mm past its origin, the artery of the tarsal canal gives rise to a branch that supplies the medial surface of the talar body. This vessel, known as the deltoid branch, passes between the talotibial and talocalcaneal portions of the deltoid ligament and supplies the medial periosteal surface of the talar body.59,76,110 The second branch derived from the posterior tibial artery consists of a vascular plexus over the posterior medial tubercle of the talus. It is formed by calcaneal branches of the posterior tibial artery and an anastomosis with branches from the peroneal artery.59,76,110,140 The anterior tibial, or dorsalis pedis, artery also provides blood to the talus from two groups of vessels. First, it sends branches to the superior surface of the talar neck. These branches arise either directly from the anterior tibial artery as medial tarsal branches or indirectly as branches of the anteromedial malleolar artery.81,119 According to Kelly and Sullivan,76 these branches are important sources for circulation to the talar head. Second, the anterior tibial artery gives rise to the anterolateral malleolar artery, which can anastomose with the perforating peroneal artery that becomes the artery of the tarsal sinus. Wildenauer166 stressed the importance of two vessels, the artery of the tarsal sinus and the artery of the tarsal canal, in supplying blood to the talus. Schwarzenbach et al,140 using arteriography, specifically described the arterial and venous blood vessels in the sinus tarsi in a series of amputation specimens. The sinus tarsi artery was formed in all cases from anastomoses among various arteries of the lateral region of the foot. These included the anterior lateral malleolar and proximal lateral tarsal arteries in all cases. In seven specimens an additional branch was from the distal lateral tarsal artery, and in the remaining three specimens, an additional anastomotic branch was from the peroneal artery. Whatever its origins, the sinus tarsi artery was the principal supplier of the intrasinus structures and of the talus. In all cases, anastomoses were within the sinus tarsi between the sinus tarsi artery and the artery of the tarsal canal.140 The posterior tibial artery gives rise to the artery of the tarsal canal about 1 cm proximal to the origin of the medial and lateral plantar arteries. This artery of the tarsal canal passes anteriorly between the sheaths of the flexor digitorum longus and flexor hallucis longus muscles to enter the tarsal canal.59,76,110 Within the canal, the artery lies in the dorsal half of the canal, closer to the talus than the calcaneus.110 It anastomoses with the artery of the tarsal sinus to form what is called the artery of the tarsal sling; this artery is located beneath the talus and passes through the tunnel formed by the tarsal sinus and the tarsal canal. In this tunnel, it gives rise to branches that enter the inferior aspect of the talar neck.76 Mulfinger and Trueta110 found this anastomosis in all their specimens. Wildenauer,166 Schwarzenbach et al,140 and others59,76,81 believe that the arteries of the tarsal sinus and tarsal canal, together with the medial periosteal network, are the most important sources of blood supply to the talus. The head of the talus has two sources of blood supply. Branches from the anterior tibial (dorsalis pedis) artery supply the superior medial half, and the lateroinferior half is supplied directly from the arteries of the tarsal sling.59,76,110 Inferiorly, the part of the talar neck that forms the anterior boundary of the tarsal sinus is the entryway for the intraosseous circulation to the talar head of the talus. According to Mulfinger and Trueta,110 this vascular pattern to the talar head is relatively constant. Peterson et al119,120 described a rich vascular connection between the head of the talus and the navicular arising from the many supporting ligaments and the talonavicular capsule. The body of the talus is supplied by vessels that enter through five surfaces: the superior surface of the talar neck, the anterolateral surface of the talar body, the inferior surface of the talar neck (roof of the tarsal canal), the medial surface of the talar body (deltoid ligament), and the posterior tubercle.59,76,110,140 The main blood supply to the lateral two thirds of the talar body is from the artery of the tarsal canal, which provides four or five main branches into the body, and the medial one third of the body is supplied by the deltoid branch, which enters from the medial surface of the talus.59,119,134 The arteries that enter the superior aspect of the neck send one or two branches into the central anterosuperior aspect of the body. Finally, the posterior tubercle of the talus is supplied by small branches from the posterior anastomotic network formed by the peroneal artery and posterior branches from the posterior tibial artery.110 Peterson and Goldie119 emphasize that these posterior vessels also provide communication between the intraosseous blood supply of the tibia and that the talus through the posterior capsule of the talotibial joint. Anastomoses between the various intraosseous arteries of the talus are responsible for the survival of the talus in severe injuries.59 Mulfinger and Trueta110 noted definite vascular anastomoses within the talus in 60% of their specimens. Arteries entering the superior neck anastomosed with branches of the artery of the tarsal canal in 26% of cases, and anastomoses between the inferior and superior vessels of the talar head were noted in 13% of cases. Anastomoses between branches of the artery of the tarsal sinus and the artery of the tarsal canal occurred within the talus 13% of the time, and anastomoses between the posterior tubercle branches and branches arising from the artery of the tarsal canal occurred in 3% of specimens. Finally, the deltoid branches medially anastomosed with branches from the artery of the tarsal canal in 3% of patients. These anastomoses may protect the talus when it sustains a major injury. The lack of these connections in certain areas of the talus may also explain why AVN can affect portions of the talar body differentially. Peterson et al119–121 demonstrated that although nondisplaced fractures of the talar neck disrupted some of the intraosseous branches arising from the tarsal sinus and tarsal canal arteries, the major portion of the vascular supply of the talus remained intact through the deltoid ligament and major branches from the artery of the tarsal sling. With displaced fractures of the talar neck, however, the deltoid branches, the superior talar neck branches, and the artery of the tarsal sling could all be potentially disrupted, thereby increasing the incidence of AVN. Furthermore, when one of these three major sources was spared injury, intraosseous anastomoses possibly permitted the talus to survive. These findings support the concept that damage to a significant portion of the talar blood supply is directly related to fracture displacement.110,119 Less than 10% of all fractures of the talus involve the talar head.24,116 Many fractures of the talar head do not occur as isolated injuries but occur instead in conjunction with complex talar neck and/or body fractures, or as part of complex Chopart fracture dislocations. The disability arising from these fractures primarily results from involvement of the articular surface with pain on weight bearing secondary to the development of posttraumatic talonavicular arthritis. Talar head fractures are usually the result of falls or motor vehicle accidents. The two types of fractures of the talar head are compression fractures and shear fractures. Compression fractures represent impaction injuries to the talar head.24,77,81,116 The force of impaction is transmitted along the longitudinal axis of the plantar-flexed foot through the metatarsals and navicular to compress the talar head. This force usually produces a compression fracture in the medial portion of the talar head and also can be associated with compression fractures of the navicular. Coltart24 noted an association with midtarsal joint dislocations and suggested that abduction and adduction may be important, in addition to longitudinal compression, in producing these injuries. The talonavicular joint may be unstable if the fracture involves a large portion of the talar head.36 The second type of talar head fracture is a result of shear, secondary to an inversion injury.81 This in turn causes midtarsal adduction and results in the navicular shearing off a portion of the medial talar head at the articulation. Shear fractures may be undisplaced, displaced, or comminuted, but they usually manifest with two distinct fragments (Fig. 39-6). These patients give a history of an injury in which the foot is plantar flexed at the time of impact. They complain of pain over the dorsal aspect of the foot in the region of the talonavicular joint.24,77,116 Usually, point tenderness and swelling are located over the talar head, and the motion of the midtarsal joint reproduces the pain. Fractures of the talar head are usually evident on anteroposterior (AP), lateral, and oblique radiographs of the foot. Careful evaluation of the outline of the talar head and neck on the lateral and AP views is particularly important in making the diagnosis and determining displacement.35 Isolated talar head fractures are subtle and may occasionally be missed, so careful scrutiny of radiographs is required. If routine radiographs do not give a clear indication of fracture location and size, particularly in longitudinal or oblique (nonimpaction) fractures, computed tomography (CT) is recommended. Associated fractures of the navicular and subluxations or dislocations of the transverse tarsal joints should also be sought. Nondisplaced fractures of the talar head can be treated with a below-knee non–weight-bearing cast for 4 weeks, followed by progressive weight bearing until the fracture is seen healed on radiographs and is painless on clinical examination.24,35,77,81,116 When the fracture of the talar head is displaced, resulting in either articular surface incongruity or disruption of the talonavicular joint, open reduction and internal fixation (ORIF) are required.35,54,155 The goal of surgery is to restore the articular surface (talonavicular and talocalcaneal joints) and the length and alignment of the medial and lateral columns of the foot. For crush, coronal, and medial shear fractures, the talar head is typically approached through an anteromedial or medial extensile approach.9,36 More central or lateral head fractures are difficult to visualize through a medial approach without extensive dorsal dissection, and therefore, in these cases, a more dorsal incision over the fracture line may be preferred. Smaller fragments may place pressure on the skin and may occasionally block talonavicular or ankle motion. Coltart55 and others77,116 recommended excision of these small fragments. For larger fragments requiring reconstruction, displacement or shortening of the medial column may be reversed using a small external fixator placed from the talar neck or calcaneus to the cuneiform or navicular. Distraction along this axis facilitates disimpaction and reduction of the talar head fracture.9,36 After anatomic reduction of the fragments and provisional Kirschner (K)-wire fixation, fixation is performed with mini- or small-fragment (1.5, 2.0, or 2.7 mm) lag screws. In most cases, screws will need to be placed through the articular surface and therefore should be countersunk, or headless screws should be used.9 Large impaction injuries may require cancellous bone grafting and/or temporary spanning of the talonavicular joint with the small external fixator until healing has occurred. In rare cases with severe comminution or articular injury to the talar head or the navicular, primary talonavicular arthrodesis may be considered.13 More commonly, this is performed as a salvage procedure in patients with recalcitrant pain. Dunn et al35 preferred a triple arthrodesis for isolated talonavicular arthritis. Although rare, malunion of the fracture is also possible. Verhaar164 reported a case of recurrent midtarsal dislocation secondary to a malunion of the talar head. This required an osteotomy and repositioning of the fragment to correct the problem successfully.
Fractures and Fracture-Dislocations of the Talus
Anatomy
Skeletal
Talar Head
Talar Neck
Talar Body
Vascular
Extraosseous Arterial Supply
Posterior Tibial Artery
Anterior Tibial Artery
Artery of the Tarsal Sinus
Artery of the Tarsal Canal
Intraosseous Arterial Supply
Talar Head
Talar Body
Intraosseous Anastomoses
Fractures of the Talar Head
Incidence
Mechanism of Injury and Classification
Clinical Evaluation
Radiographic Evaluation
Treatment
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Musculoskeletal Key
Fastest Musculoskeletal Insight Engine
 )
)