Fig. 38.1
The 1960s to the 1970s with outstanding pioneers: Charles Neer [1, 2] was the first to implant shoulder anatomic hemiprosthesis. With Averill, he was also the first to implant a reverse prosthesis in case of no cuff since the anatomic and non-constrained designs were not efficient for eccentric arthritis. Reversed shoulder arthroplasty from Neer (mark 1 and mark 3). Center of rotation is lateralized from the normal anatomy (Courtesy of Emmanuel Baulot)
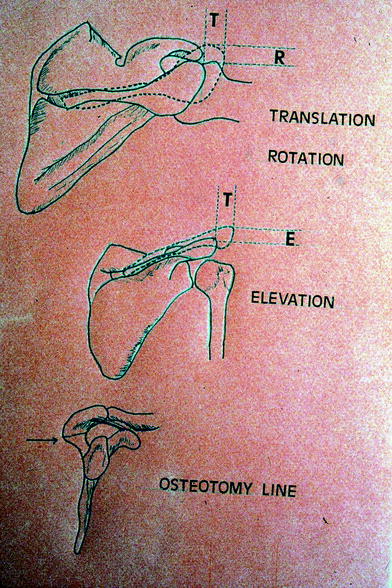
Fig. 38.2
In 1975, Paul Grammont imagined the «TRE acromion osteotomy» (translation and elevation) to increase the natural evolution of the scapula (more lateralized acromion) (Courtesy of Emmanuel Baulot: Paul Grammont original draw)

Fig. 38.3
In cuff tear arthropathy, anatomic conditions are not anatomic since there is no cuff at all. “TRE osteotomy” cannot work, since there is arthritis too. Therefore, Grammont looked for a non-anatomic arthroplasty design, which was to become the “ovoid prosthesis.” The goal was to lateralize humerus (Courtesy of Emmanuel Baulot)

Fig. 38.4
In 1985, the results were promising regarding pain with the “ovoid arthroplasty,” but active ROM was poor. Grammont was still looking for better prosthesis designs and imagined the first modern reversed prosthesis: the “Trumpet” design. The goal was to medialize the center of rotation (Courtesy of Emmanuel Baulot)
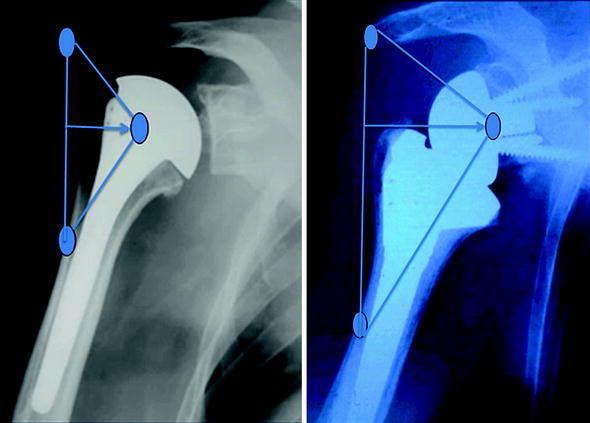
Fig. 38.5
The Delta 3 prosthesis was created in 1987 [3–5]. As with the “Trumpet,” the aim was neither to lateralize acromion such as “TRE osteotomy” nor to lateralize the humerus like the “ovoid prosthesis” but to medialize the center of rotation of the humerus with a new and special implant design. The deltoid moment is stronger for the Delta 3 (right arrow) than for anatomic design (left arrow)
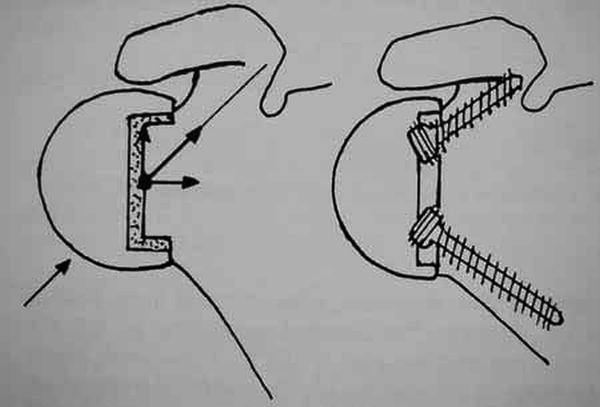
Fig. 38.6
“Trumpet” design on the left, “Delta 3” design on the right. Center of rotation is more medialized for the “Delta 3” (into the neck of the scapula), more lateralized for the “Trumpet” (into the ball)
The Arrow Platform System from FH Orthopedics: Biomechanics
High rates of glenoid notching have been reported with the Delta 3. In order to avoid glenoid notching and to get better rotations, we decided to make a less medialized glenoid implant design. The center of rotation is not in the glenoid neck (in the bone), but in the ball, 8.5 mm more lateralized than the Delta 3 (Fig. 38.7). The humeral implant is more lateralized (3.5 mm) too (Fig. 38.8). Because of this new design, there is less impingement between the socket and the neck of the scapula and therefore no notching. In addition, this new design gets more tension onto the soft tissue around the shoulder (anterior and posterior deltoid portion) and increases rotations for better daily-life activities. Instability is less frequent as well.
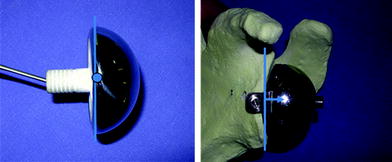
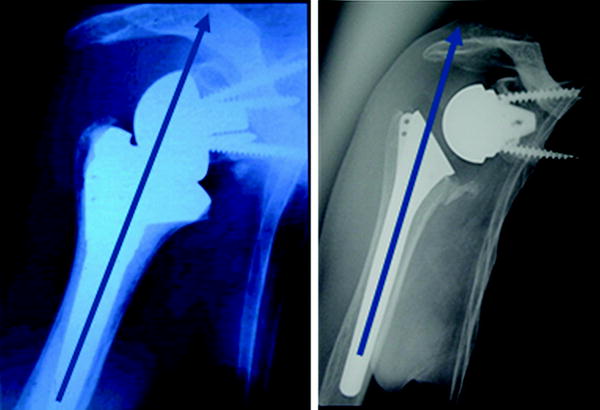
Fig. 38.7
Arrow (left the center of rotation is put over baseplate) is less medialized (8.5 mm) than Delta 3 (right the center of rotation is embedded in baseplate)
Fig. 38.8
Arrow shape (right) of humeral component more lateralized (3.5 mm) than delta 3 (left)
The metal-backed component is a posterior convex back to decrease risk of loosening. A keel with a winglet offers a very strong press fit for an efficient primary fixation, which enhances the bone fixation.
Two compressive non-locked screws (superior and inferior) limit loosening. A third sagittal screw can be added in case of insufficient press fit (Fig. 9). In case of the need for glenoid component revision or glenoid bone loss, it is possible to use a keel with a long stem, which penetrates the native glenoid cortical bone allowing glenoid reconstruction with cancellous bone graft.
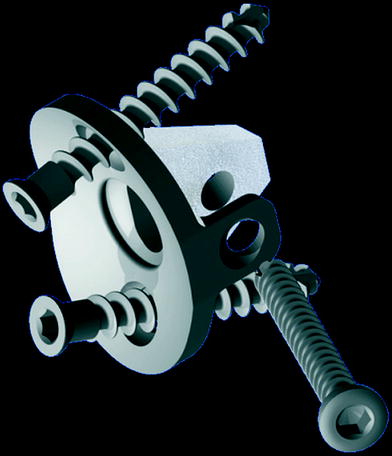
Fig. 38.9
Convex back metal-backed component with a winglet
Less medialization of reverse shoulder arthroplasty improves external and medial rotation, thus facilitating the daily-life activities of older patients. The absence of glenoid notching and glenoid loosening hopefully reflects longer prosthesis survival.
Surgical Technique
Soft tissue surgery of the shoulder is the main point to obtain an optimal exposition of the humerus and the glenoid fossa and to fix in good positions the prosthetic implants. Arrow prosthesis is characterized by a center of rotation less medialized than original Grammont prosthesis to restore better external rotation and less glenoid notching. An improvement of the primary fixation of the glenoid component should be necessary to oppose tilting forces at the beginning of the abduction.
Anesthesia and Patient Positioning
General anesthesia is always used and is supplemented by an interscalene block. A catheter is left in place for 48 h to ensure postoperative analgesia and to facilitate immediate postoperative rehabilitation. The patient is positioned in a «semi sitting» beach chair position, with the entire upper limb draped. The arm should be completely free within the operative field to facilitate humerus and glenoid exposure.
Related posts:
 Intact Rotator Cuff
Origins of Reverse Shoulder Arthroplasty and Common Misconceptions
Proximal Humerus Tumors
Value and Reverse Total Shoulder Arthroplasty: The Foundation for Orthopaedic Research and Education Perspective
Aston Medical Duocentric® Reversed Prosthesis: Proposition of New Glenoid Component Design to Prevent Scapular Neck Notching
DJO Surgical Reverse Shoulder Prosthesis (RSP™)
Intact Rotator Cuff
Origins of Reverse Shoulder Arthroplasty and Common Misconceptions
Proximal Humerus Tumors
Value and Reverse Total Shoulder Arthroplasty: The Foundation for Orthopaedic Research and Education Perspective
Aston Medical Duocentric® Reversed Prosthesis: Proposition of New Glenoid Component Design to Prevent Scapular Neck Notching
DJO Surgical Reverse Shoulder Prosthesis (RSP™)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


