Femoral Neck Fractures
EPIDEMIOLOGY
More than 250,000 hip fractures occur in the United States each year (50% involve the femoral neck). This number is projected to double by the year 2050.
Eighty percent occur in women. This incidence doubles every 5 to 6 years in women age >30 years.
There is a bimodal incidence. The incidence in younger patients is very low and is associated mainly with high-energy trauma. The majority occur in the elderly (average age of 72 years) as a result of low-energy falls.
The incidence of femoral neck fractures in the United States is 63.3 and 27.7 per 100,000 population per year for women and men, respectively.
Risk factors include female sex, white race, increasing age, poor health, tobacco and alcohol use, previous fracture, fall history, and low estrogen level.
ANATOMY
The upper femoral epiphysis closes by age 16 years.
Neck-shaft angle: 130 ± 7 degrees
Femoral anteversion: 10 ± 7 degrees
There is minimal periosteum about the femoral neck; thus, any callus that forms must do so by endosteal proliferation.
Calcar femorale: This is a vertically oriented plate from the posteromedial portion of the femoral shaft radiating superiorly toward the greater trochanter.
The capsule is attached anteriorly to the intertrochanteric line and posteriorly 1 to 1.5 cm proximal to the intertrochanteric line.
Three ligaments attach in this region:
1. Iliofemoral: Y-ligament of Bigelow (anterior)
2. Pubofemoral: anterior
3. Ischiofemoral: posterior
Vascular supply (see Fig. 27.3)
Forces acting across the hip joint
Straight leg raise: 1.5 × body weight
One-legged stance: 2.5 × body weight
Two-legged stance: 0.5 × body weight
Internal anatomy: The direction of the trabeculae parallels the direction of compressive forces. The bony trabeculae are laid down along the lines of internal stress. A set of vertically oriented trabeculae results from the weight-bearing forces across the femoral head and a set of horizontally oriented trabeculae results from the force of the abductor muscles. These two trabeculae systems cross each other at right angles.
MECHANISM OF INJURY
Low-energy trauma: This is most common in older patients.
Direct: A fall onto the greater trochanter (valgus impaction) or forced external rotation of the lower extremity impinges an osteoporotic neck onto the posterior lip of the acetabulum (resulting in posterior comminution).
Indirect: Muscle forces overwhelm the strength of the femoral neck.
High-energy trauma: This accounts for femoral neck fractures in both younger and older patients, such as motor vehicle accident or fall from a significant height.
Cyclical loading-stress fractures: These are seen in athletes, military recruits, and ballet dancers.
Insufficiency fractures: Patients with osteoporosis and osteopenia are at particular risk.
CLINICAL EVALUATION
Patients with displaced femoral neck fractures are typically nonambulatory on presentation, with shortening and external rotation of the lower extremity. Patients with impacted or stress fractures may lack deformity and they may be able to bear weight. They may, however, demonstrate subtle findings, such as groin pain and pain with axial compression.
Those involved in high-energy trauma should be subjected to standard Advanced Trauma Life Support (ATLS) protocols.
Pain is evident on attempted range of hip motion, with pain on axial compression, and with tenderness to palpation of the groin.
An accurate history is important in the low-energy fracture that usually occurs in older individuals. Obtaining a history of loss of consciousness, prior syncopal episodes, medical history, chest pain, prior hip pain (pathologic fracture), and preinjury ambulatory
status is essential and critical in determining optimal treatment and disposition.
All patients should undergo a thorough secondary survey to evaluate for associated injuries.
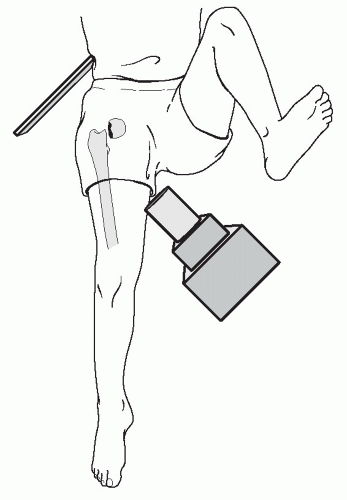 FIGURE 29.1 A cross-table lateral view of the affected hip is obtained by flexing the uninjured hip and knee 90 degrees and aiming the beam into the groin, parallel to the floor and perpendicular to the femoral neck (not the shaft). This allows orthogonal assessment of the femoral neck without the painful and possible injurious manipulation of the affected hip required for a “frog-leg” lateral view. (From Bucholz RW, Heckman JD, eds. Rockwood and Green’s Fractures in Adults. 5th ed. Baltimore: Lippincott Williams & Wilkins; 2002.) |
RADIOGRAPHIC EVALUATION
An anteroposterior (AP) view of the pelvis and an AP and a cross-table lateral view of the involved proximal femur are indicated (Fig. 29.1). A frog lateral is contraindicated.
A physician-assisted internal rotation view of the injured hip is always helpful to further clarify the fracture pattern and determine treatment plans.
A computed tomography (CT) scan is of value in the trauma patient. Abdominal-pelvic CT cuts can be scanned for nondisplaced femoral neck fractures.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



