CHAPTER 36  Extensive labral tears—pathology and surgical treatment
Extensive labral tears—pathology and surgical treatment





Introduction
Shoulder instability and glenoid labral injuries are commonly seen in an athletic population. Traumatic lesions of the anterior glenoid labrum, Bankart lesions, were first described by Perthes1 and Bankart.2 The association between Bankart lesions and anterior glenohumeral instability has been well documented. Arthroscopic repair of anterior instability and posterior or reverse Bankart lesions for posterior glenohumeral instability has shown good results in returning athletes to their preinjury level of participation.3–7 Superior labral lesions were first described by Andrews8 in a throwing athlete population. Snyder9 later classified the superior labrum anterior and posterior (SLAP) lesions into four categories and initially described arthroscopic repair techniques.
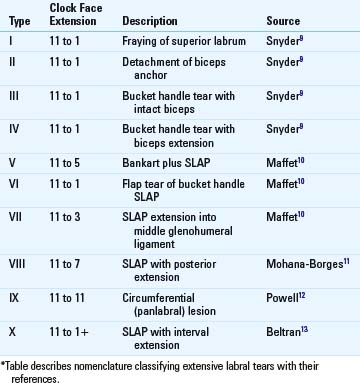
Labral lesions can exist in combination. Maffet10 expanded on Snyder’s original SLAP classification with three additional types. In a type V lesion, the SLAP extends into a Bankart lesion, giving a combined superior and anterior lesion. A type VI lesion demonstrates a flap tear of the bucket handle tear of the biceps, and is a variant of a type III lesion. A type VII tear is another combined superior-anterior tear, with the SLAP extending into the middle glenohumeral ligament. Mohana-Borges11 described a type VIII lesion as a SLAP tear extending into the posterior inferior glenohumeral ligament. The most extensive of labral lesions was described by Powell et al12 as a type IX, or panlabral lesion, denoting a complete circumferential tear of the glenoid labrum. Finally, Beltran13 noted a combined SLAP lesion with extension into the rotator interval on MR arthrography, now often described as a type X lesion. This classification system and each type’s unique quality are listed in Table 36-1.
The diagnosis and treatment of combined labral lesions is more complex than that of its isolated cousins. Making a complete and accurate diagnosis requires careful attention to patient history, physical examination, and appropriate imaging.14 Patient positioning, increased operative time and technical difficulty, order of repair, adequate resourcing, and postoperative rehabilitation precedence are all issues that must be addressed in a comprehensive approach to these lesions.
Preoperative history
Furthermore, patients with prolonged symptoms with multiple dislocations should elevate one’s level of suspicion for a complex labral lesion. In a series comparing isolated Bankart lesions with combined Bankart and SLAP lesions, Hantes noted that the number of dislocations was significantly higher in the combined group.15 In a review of 41 panlabral lesions, Tokish14 et al, noted that all patients in their series had sustained at least 5 prior dislocations, and all had chief complaints of pain and instability. The authors noted that this complaint of pain persisted well after reduction of the joint. This was in contrast to their experience with isolated anterior lesions that were often relatively painless between instability episodes. They concluded that multiple dislocations and pain that persisted between instability episodes were clinical tips for diagnosing combined labral lesions.
Examination findings
Provocative tests can be quite helpful in making a diagnosis of a complex labral lesion. We recommend that every patient with a suspected labral lesion undergo cardinal testing for the anterior, posterior, and superior lesions. For the anterior (Bankart) lesion, the gold standard test is that of apprehension16 in an abducted externally rotated position. This test is performed by bringing the patient’s arm into maximum external rotation while at 90 degrees of abduction, in an attempt to reproduce the patient’s sensation that the shoulder is unstable. It is important to differentiate this sensation from a sensation of pain, which is more consistent with superior labral tears. Patients who have both apprehension and pain may demonstrate a combined SLAP and Bankart lesion.
Tests for determining tears of the superior labrum are notoriously nonspecific. This is likely because of the overlap with SLAP tears and impingement, especially in older populations. Nevertheless, we consider the active compression test17 as the cardinal test for superior pathology. In our experience, this test is rarely positive in patients with unidirectional instability, so a patient who has a history and physical examination consistent with dislocations and who demonstrates a positive active compression test raises our suspicion that the labral tear extends up into the superior labrum. This is especially true in the absence of impingement signs such as Neer and Hawkins16 sign.
The cardinal test for the posterior labral tear is the push-pull test.16 This test is performed with the patient supine, and the arm at 90 degrees of abduction and neutral rotation. The examiner “pushes” the shoulder out posteriorly, while “pulling” the grasped wrist to stabilize the arm. The resultant motion subluxes the shoulder in most patients. In patients with posterior labral pathology, this test often exactly reproduces a patient’s symptoms, and if it does, a posterior labral tear should be suspected. We have found this test to be nearly universally present in complex labral lesions with a posterior component.14 Other tests, such as a posterior load-and-shift, or jerk test, can be equally provocative but may be effectively guarded against by the apprehensive patient.
Pearls and Pitfalls of Complete Diagnosis of a Labral Lesion
Radiographic findings
Radiographic evaluation is of critical importance in the diagnostic workup of suspected combined labral lesions. Although radiographs will not show a labral tear directly, a standard true AP, scapular Y view, and an axillary lateral view should be obtained in all patients. Such views can demonstrate subluxation or osseous pathology suggestive of instability, such as bony Bankart and Hill-Sachs lesions. These bony lesions can exist in the presence of combined labral lesions,14 and should be identified and addressed when necessary (Video 36-1). Radiographs also should be evaluated for the absence of concomitant pathology (e.g., glenohumeral arthritis).
Complete characterization of labral lesions can be difficult. The ideal imaging study for evaluation of the complex labral lesion is a magnetic resonance arthrogram (MRA). In one study, the addition of contrast helped identify 77% of panlabral lesions compared with only 9% completely identified with noncontrast MRI.14
Related posts:
 Recurrent instability due to capsular deficiency
Open treatment of anterior instability—surgical technique
Arthroscopic treatment of multidirectional instability—surgical technique
Radiographic studies and findings
Examination and classification of instability
Imaging findings in posterior instability
Recurrent instability due to capsular deficiency
Open treatment of anterior instability—surgical technique
Arthroscopic treatment of multidirectional instability—surgical technique
Radiographic studies and findings
Examination and classification of instability
Imaging findings in posterior instability
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


