Fig. 36.1
Forearm bones fractures treated with open reduction and internal fixation
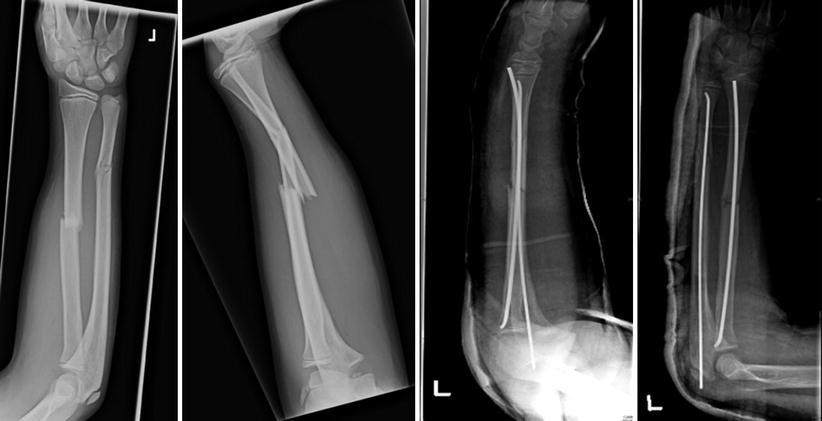
Fig. 36.2
Forearm bones fractures treated with elastic nailing
Surgical intervention is aimed at reduction followed by stabilisation of the fracture. Fracture reduction reduces the deformity following a fracture by normalising the alignment of the radius and ulna. Reduction can either be closed (externally by manipulation under X-ray control) or open (by surgical exposure, visualisation and instrumentation). Surgical stabilisation of the fracture involves holding the reduction such that the restored alignment following reduction is maintained. Devices for surgical stabilisation can be either internal to the forearm or external such as an external fixator. Internal devices can either be elastic stable intramedullary nails (ESIN) or a combination of plates and screws. Whilst in adults ORIF has been established as the optimal surgical intervention for diaphyseal forearm fractures, in children the options of ORIF and ESIN are both widely used and equally popular.
Not only is there an increase in the incidence of forearm fractures but there is a trend towards surgical stabilisation [3, 7, 14]. An 11 year period from 1998 saw the proportion of fractures being managed with ESIN triple from 10 % to 30 % [7]. The increasing popularity of ESIN can be attributed to the less invasive surgical technique of ESIN with the possibility (perceived) of less complications, the resulting reduced risk of redisplacement postoperatively [20, 21] and the attraction of a prosthesis that is relatively easier to remove than the traditional plates and screws.
The trend has generally been to remove orthopaedic implants once the operated bone has fully healed. This is usually undertaken a year or so after operation before new bone formation buries the implant completely. Removal of ESINs is much easier than plates or other implants that are fixed to the bone. Access to the ends of the ESIN is usually in safe zones, where neurovascular structures (nerves and blood vessels) are not at risk. Conversely plate removal requires a surgical dissection though inter-nervous or inter-muscular planes. These planes are often scarred and less discrete following previous open reduction and internal fixation. Thus repeat surgery, for the removal of plates and screws, requiring dissection may endanger neurovascular structures.
Surgical stabilisation prevents motion at the fracture site, thereby preventing displacement and recurrence of deformity at the fracture site. Anatomical restoration should help to maximise function of the forearm once rehabilitation from the injury is complete.
Generally intramedullary nailing consists of a manipulation (closed reduction) with percutaneous insertion (through a small incision in the skin) of the Elastic Stable Intramedullary Nail (ESIN). This technique allows for the formation of callus from the fracture haematoma which subsequently ossifies. The fracture ends are manipulated to approximate the shape of the pre-fracture radial shaft before being secured using an ESIN.
Open reduction and internal fixation (ORIF) involves surgical dissection and exposure of the fracture. The two ends of the fractured bone are perfectly matched like a jigsaw. This type of reduction is both macroscopic and microscopic allowing for the restoration of the microscopic, cellular and matrix bone anatomy, without the need for bridging callus. The reduced bone is then stabilised using an implant, typically a plate with screws.
The indications for surgical interventions, for diaphyseal fractures of the radius and ulna in children, are not clear. Similarly, the relative effects of various methods of surgery, particularly intramedullary nailing and plate fixation are not established.
There is paucity of Level I and II data that compares either surgical versus non-surgical interventions, or different surgical interventions for the fixation of fractures of the forearm in children. A review of the literature reveals a handful of Level III or IV retrospective studies looking at a comparison of IM nailing compared to ORIF. Some of these studies are of historic value, using implants (e.g. Rush Pin) which are no longer in vogue. There are two recent systematic reviews assessing the literature on operative intervention for forearm fractures [22, 23]. Baldwin et al. [22] conducted a systematic review and meta-analysis of 12 (525 patients); all were level III studies. Primary outcome was union rate. Patel et al. [23] conducted a systematic review of 8 studies; 446 participants (264 IMN and 182 plating). Primary outcome was the functional range of motion. The main summary of both demonstrates little difference in outcomes between ESIN and ORIF in paediatric patients. They also demonstrate that this genuine point of clinical equipoise now warrants randomised control trials to determine the better of the two methods.
Whilst there is no Level I and II evidence, there are a number of observational studies that must be noted [12, 13, 14, 24–28]. The studies most relevant to the management of forearm fractures vary in size from 31 to147 participants. The average age in each study also differed, as well as the average age between groups in each study. The average age of the ESIN groups (9.3–13.3) trended to be lower than the ORIF group (9.5–14.5) in all the studies (though not statistically significantly). None of these papers demonstrated any statistically significant differences in functional outcome between ORIF and ESIN. In addition differences with regards to complications between the two groups were not consistent between the studies. The systematic review with the largest number of studies found that non-union and delayed union was relatively uncommon in all series [22]. The incidence of non-unions requiring revision surgery in the meta-analysis was 1.7 % for ORIF vs. 2.4 % for ESIN. The incidence of delayed union in the IMN group was 5.5 % compared to 0.8 % in the ORIF group. However, this difference was not found to be statistically significant. This same review split complications into major and minor and found major complications to be 7.2 % in the ORIF group and 9 % in the IMN group with the complications being non-union, hardware failure, deep infection, compartment syndrome, unintended return to theatre in the immediate postoperative period, refracture, nerve injury, neuropathy, CRPS and arterial injury. All other complications (e.g. superficial infection, hypertrophic scar) were considered minor. As may be expected duration of surgery was significantly shorter in ESIN (or its equivalent) in the studies in which operating time was measured [27]. Cosmesis was significantly better in the ESIN group, though only measured in two studies [25, 27]. Compartment syndromes were reported in more than one study [14, 26] and in both groups. However, none of the papers indicated if the detected cases were of pre or postoperative compartment syndromes. Of note one paper that found compartment syndrome in their ESIN group did not have any cases of compartment syndrome in the ESIN group treated more than 24 h after the fracture was sustained [14].
A few authors published a small case series of using a single bone fixation [28–30]; however, their series probably included a recognised pattern of fractures where one of the bones is minimally displaced and relatively stable fracture (Fig. 36.3).

Fig. 36.3
Forearm bones fractures treated with a single elastic nail
An additional relevant factor is removal of metal work. In the author’s opinion, variation in the elective removal of implants is likely to reflect differences in the local healthcare economy. In the UK there is little appetite for the removal of all metal work routinely as this presents another burden of operative need on a publicly funded service. This may not be the case in nations where medical intervention has a financial incentive. Removal of metal work raises the concerns surrounding refracture. In the studies examined by the authors, practitioners tended to advocate routine removal of all nails in most studies. Three studies reported the effects of removal of metalwork [14, 26, 31]. Refractures were reported in both ESIN and ORIF groups. Operative decision making around removal of metal work needs to be better understood and studied.
Related posts:
 Evidence-Based Treatment of Flexible Flat Foot in Children
Evidence-Based Treatment of Glenohumeral Dysplasia Caused by Obstetric Brachial Plexus Injuries
Evidence-Based Treatment of Flexible Flat Foot in Children
Evidence-Based Treatment of Glenohumeral Dysplasia Caused by Obstetric Brachial Plexus Injuries
 Evidence-Based Treatment of Deformity in Multiple Osteochondromatosis
Evidence-Based Treatment of Deformity in Multiple Osteochondromatosis
 Evidence-Based Treatment for Slipped Upper Femoral Epiphysis
Evidence-Based Treatment for Slipped Upper Femoral Epiphysis
 Private: Physeal Injury, Epiphysiodesis and Guided Growth
Private: Physeal Injury, Epiphysiodesis and Guided Growth
 Femoro-Acetabular Impingement in Children
Femoro-Acetabular Impingement in Children
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


