Fig. 35.1
EHE. Radiograph showing a lytic lesion involving phalanges of the hallux, with cortical permeation and no reactive sclerosis
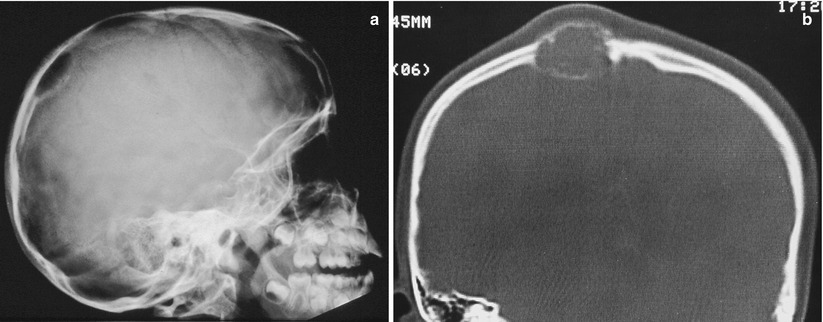
Fig. 35.2
(a) EHE. Radiograph demonstrating lytic lesions over the cranial vault. (b) EHE. Same case as (a). CT demonstrating an expansive lytic lesion involving and expanding the skull bones. There is a thin cortical shell of reactive periosteal bone
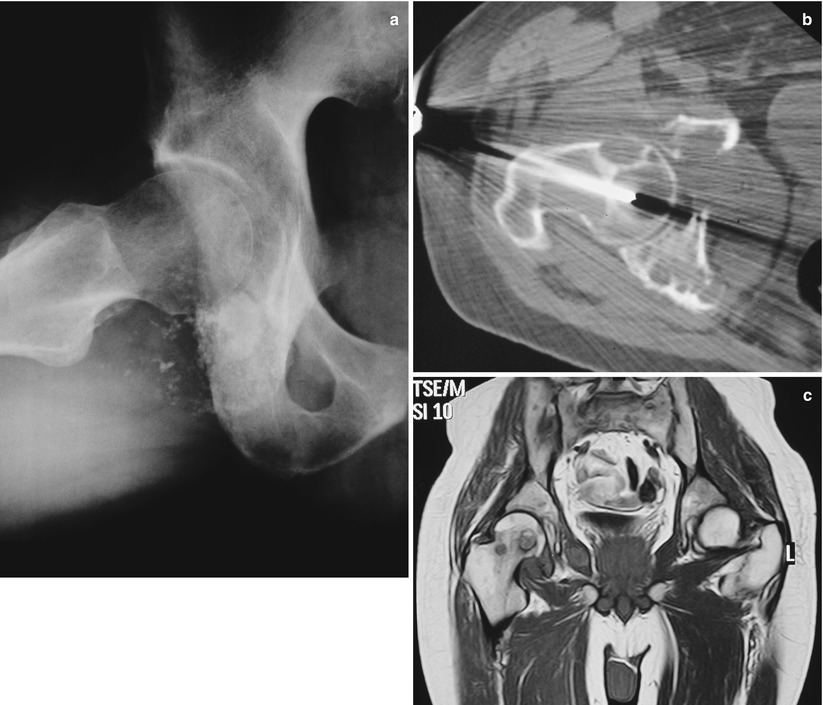
Fig. 35.3
(a) Multicentric EHE. Radiograph showing lytic lesions involving the femoral head and the iliac bone around the acetabulum. (b) Same case as a. CT shows a needle biopsy being undertaken in one of several lytic nodular lesions in the femoral head and iliac bone. There is some reactive sclerosis around some lesions. (c) MRI shows that the lesions seen in (a, b) present intermediate-intensity signal in TSE-weighted image
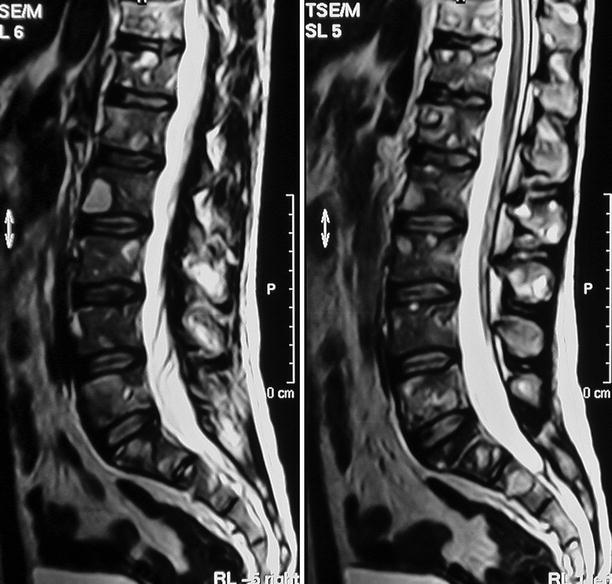
Fig. 35.4
Multicentric EHE. MRI of the lower spine demonstrates several lesions with a high-intensity signal in TSE-weighted images, involving lumbar and sacral vertebrae

Fig. 35.5
Malignant EHE. (a) Radiograph shows a large lytic lesion in the distal metaphysis of the femur with epiphyseal and cortical permeation. Medullary limits are partially indistinct and partially sclerotic. Absence of discernible periosteal bone reaction. (b) MPR CT does not show any bone or mineral deposits in this solid lesion. Medullary limits are well defined and mostly with reactive sclerosis. Cortex is destroyed and the lesion is seen involving adjacent soft parts as well as the femoral epiphysis. (c) MRI coronal view, T1-weighted image. Solid lesion with iso-intensity to muscle. Involvement of adjacent soft tissues. (d) MRI coronal view, T1-weighted image with contrast and fat saturation. Enhancement of the peripheral areas of the lesion and low-signal intensity in the center, possible necrotic area
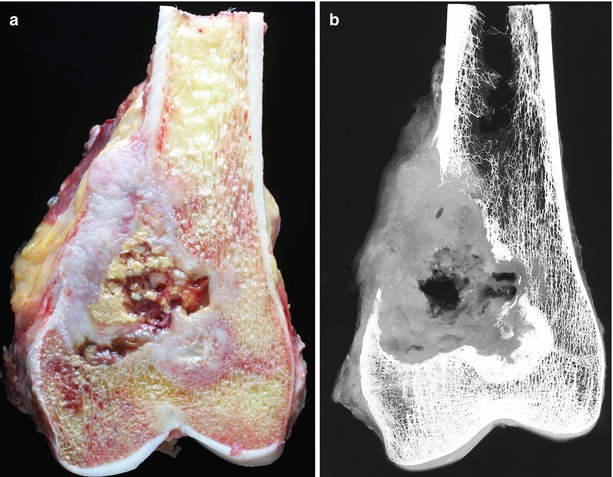
Fig. 35.6
(a) Macrophotography of the same case as previous figure. Peripheral areas of the lesion are whitish, solid, and soft, viable areas of the tumor, while the center is fragmented, yellowish red, and friable, degenerative and necrotic areas. (b) Specimen radiograph emphasizing CT findings

Fig. 35.7
Thoracic CT of the same case as previous figures. Metastatic spread to pleura and lungs
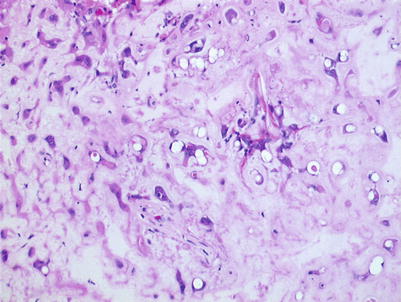
Fig. 35.8
EHE. Medium-power microphotography. Loose proliferation of endothelial cells either isolated or in chords over a bluish, myxochondroid matrix. Intracytoplasmic vacuoles, sometimes containing red cells or their fragments, are evident
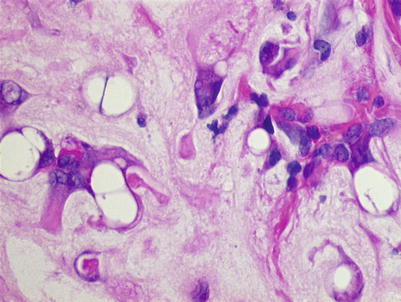
Fig. 35.9




EHE. Higher-power view of previous figure. Small nests of endothelial cells with intracytoplasmic vacuoles are demonstrated
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
