CHAPTER 127 Epidemiology of Injuries
INTRODUCTION
Back pain is one of the most common reasons patients seek medical care. Low back pain is the second leading cause for primary care office visits, with an estimated lifetime prevalence of 60–90% and an annual incidence of 2–5%.1,2 In the general population, back pain is the number one cause of disability in patients younger than 45 years of age, and the number three cause for those older than age 45. Although there has been recent debate as to whether athletes are protected from back pain or more susceptible to back pain, it remains a common complaint in the athletic population. Back pain etiology in the athlete varies from mild lumbar muscle strain to traumatic fracture dislocation of the cervical spine with associated cord compromise. However, the most common etiology of athletic back injury mirrors that of the general population – injury to soft tissue structures including muscle, ligaments/capsule, and fascia. Past studies have reported the inability to identify a specific pain generator in up to 85% of cases of low back pain. Despite these historical findings, correct identification and treatment of biomechanical deficits leading to back pain can prevent injury from recurring and progressing to a chronic phase. From a radiographic standpoint, degenerative disc disease and spondylolysis are the most commonly associated structural abnormalities seen in athletes. In fact, numerous studies have shown an increased prevalence for degenerative spine changes in athletes when compared to nonathletes.3,4
GENERAL ETIOLOGIC FACTORS
The degenerative cascade model as an etiologic predictor of back pain
Virtually all athletes are subjected to repetitive end range forces on the spine, grueling competitive schedules, rigorous training routines and, depending on the sport, significant contact forces with other players. The result is an accelerated progression through the degenerative cascade of spinal motion segments. The degenerative cascade model based upon the work of Kirkaldy-Willis5a is currently a comprehensive model of back pain (Fig. 127.1). It describes three basic stages of degeneration found in spinal motion segments due to the effects of trauma and repetitive stress. At each stage, the classification system outlines the pathoanatomical and pathophysiologic changes that occur throughout the motion segment, which can be used to predict etiology of spine-related pain. It is an important process to understand when examining etiology and epidemiology of back pain in athletes.
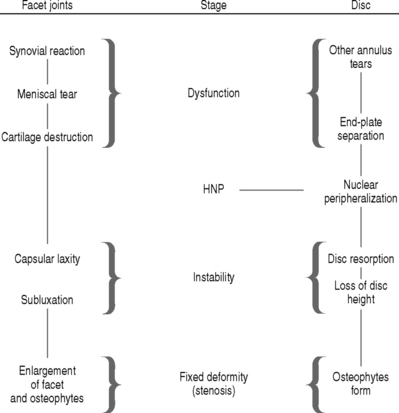
Fig. 127.1 Overview of the degenerative cascade.
(Adapted from Selby D, Saal JS: Degenerative Series. CAMP Healthcare, with permission.5)
A basic overview of the degenerative cascade is as follows:
THE EFFECT OF AGE ON ETIOLOGIC DISTRIBUTION OF BACK PAIN
Pediatric and adolescent athletes
Back pain and back injury occurs in 10–15% of all young athletes.6 The prevalence of specific injury types is related to sport played as well as position within that sport. When compared to their adult counterparts, pediatric and adolescent populations have fewer secondary gain issues and are more likely to have a pathologic etiology for their pain. Therefore, a high index of suspicion and a low threshold for the utilization of diagnostic imaging and evaluation techniques should be applied to this population.7 Red flag signs and symptoms such as night pain, constitutional symptoms, non-specific onset, failure of pain remittance with rest, weight change, skin rash, and multiple joint or organ involvement should prompt further investigation and appropriate referral. This young population also deserves special attention because some causes of back pain may be related to the growth process itself. The distribution of spine-related causes for back pain in sports can be organized by anterior element, posterior element, and soft tissue etiologies.
Anterior element
Disc disease accounts for 10% of back pain in athletes under the age of 21, and 2% of all disc herniations are attributable to this age population. The most commonly involved sports include: weight lifting, rowing, football, and wrestling.8 Scheuermann’s disease, a progressive thoracic kyphosis due to anterior wedging of at least 5° in three or more consecutive vertebral bodies, occurs in 0.4–8.3% of the population. The most common age group is 13–17 years, and increased prevalence has been noted in sports such as waterskiing.9 Thoracolumbar Scheuermann’s has been reported in weightlifting, football, gymnastics, and wrestling.10,11 Infection presenting as idiopathic infectious discitis is more common in younger patients with an average age of 6 years; however, reports span the entire pediatric and adolescent age group. Vertebral osteomyelitis, benign and malignant tumors, scoliosis, and rheumatologic disease are also more prevalent in this younger population than in adults.
Posterior element
Posterior element injuries are more common in sports requiring repetitive hyperextension such as gymnastics, football, figure skating, diving, and dance.4,6,12 Spondylolysis has been reported to account for up to 47% of low back pain in adolescent athletes.13 Spondylolisthesis is usually associated with a pars interarticularis defect or elongation, and most slip progression tends to occur during the growth spurt in preadolescence.6,14 Incidence is reported from 11% in gymnastics to 63% in diving.15,16 Lumbar facet syndrome (Z-joint synovitis) is also reported in this population, and is associated with the first stage of the degenerative cascade.
Spinal cord injury
It is noteworthy to mention the high risk of cervical spine injury in the pediatric population associated with trampoline use and diving accidents. In 1998, more than 6500 trampoline-associated cervical spine injuries occurred in pediatric patients. Although most were minor injuries, there were reports of death and quadriplegia. This represented a fivefold increase over a 10-year period at the time of report.17 Increased risk for serious spinal trauma due to diving in uncontrolled environments is also prevalent in this population.
Young adult athlete
The repetitive multiplanar nature of sport-specific training regimens (rotation, flexion–extension, and axial loading of the spine), high number of hours spent in training, and the general use of weight training for overall strength and conditioning may lead to earlier evidence of stage I (dysfunction) and stage II (instability) degenerative change in the spine compared to nonathletes. This is supported by radiographic evidence as well as the types of injury commonly encountered in this population.3,4
Older adult athlete
As the general population ages, the number and age of those participating in sporting activities continues to increase. There will be approximately 70 million people age 65 or older in the United States by the year 2030.18 The spinal motion segments in this subset of the population are more likely to be further along in the degenerative cascade (instability and stabilization phases of degeneration). In addition, medical comorbidity and age-related changes including diminished bone density, general loss of strength and muscle mass, changes to the vestibular, visual, and somatosensory systems, as well as decreased joint flexibility may play a role in back injury.19
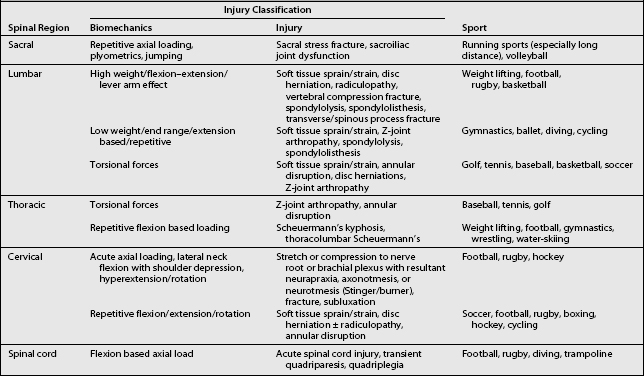
EPIDEMIOLOGIC DATA AND BIOMECHANICAL FACTORS FOR SELECTED SPORTS
Table 127.1 summarizes the basic biomechanical etiologic factors associated with common spine injuries in sports.
Baseball/softball
Overview
Between 1995 and 1999, back injuries accounted for approximately 5% of all disabled list (DL) days in major league baseball. Overall, back pain accounted for the fifth highest number of injuries per anatomic region reported. In 1999, the number of DL days attributable to back injury reached 1490 days, which even outnumbered the 1348 days for wrist and hand injury.20
Severe injury to the cervical spine, while uncommon, is typically associated with head-first sliding. These neck hyperextension injuries range from ligamentous disruption to vertebral fracture and quadriplegia. The mechanism involves rapid deceleration against a stationary base or opposing player. However, the incidence of cervical spine injury has decreased since the advent and widespread use of breakaway bases.21 Other cervical spine injuries, which may be observed in pitchers, include those to the Z-joints and cervical discs.
Lumbar spine injury in baseball and softball is commonly attributed to hitting. Frequent participation in batting practice produces repetitive rotational movement that accelerates the progression of degenerative changes in spinal motion segments. The most common etiology of pain in this population is soft tissue in nature, while less common injuries include disc herniation, Z-joint arthropathy, spondylolysis, and spondylolisthesis.22,23
Fast-pitch softball
According to the NCAA Injury Surveillance System data from 1997/1998, 5–15% of all traumas in fast-pitch softball were due to injury to the thoracic, back, and abdominal regions. Low back injury accounted for 7% of these injuries. Back injury is most commonly associated with overuse injuries and contusions.24
Functional considerations
Frequent batting practice subjects the lumbar spine to repetitive stress injury. Watkins recorded surface EMG data from 18 professional baseball players to evaluate hitting mechanics and determined that the erector spinae and abdominal oblique were the most important muscles involved in trunk stabilization and rotation for smooth power transfer throughout the kinetic chain. They also noted that hamstring and lower gluteus maximus contributed most to the ‘stable base’ and ‘power-of-the-thrust’ form that the torso ‘uncoils’ during the swing.22 As predicted by the kinetic chain model of biomechanics, coordinated transfer of muscle activity occurs from the lower extremities to the trunk to the upper extremities. Any isolated weakness along the kinetic chain places undue stress on isolated functional segments and may eventually lead to overuse injury.
Kinetic chain dysfunction is also observed in injuries sustained by pitching. According to Casazza and Rossner, the baseball pitch may be the most dynamic motion executed in sports. Acceleration of the upper extremity is driven by an initial anteroposteriorly directed ground force that is transformed into a rotational force at the hip that continues through the spine to the shoulder, culminating in forceful internal rotation to accelerate the arm. The spine also plays a crucial role in the attenuation of forces during the deceleration phase of throwing. Overload of the Z-joints and the intervertebral discs may occur if the thoracolumbar fascia is unable to dissipate the forces from the spinal motion segments.25 Restricted or excessive range of motion and poor coordination at specific segments along the chain may be as important, or more important, than relative weakness of isolated segmental musculature.
Basketball
Overview
In basketball players, thoracic and lumbar spine injuries are more common than those to the cervical spine. Overall, the most common injuries to the spine are lumbosacral soft tissue strains and sprains, as opposed to discogenic or bony abnormalities. Traditional ‘weekend warrior’ athletic injuries commonly arise as a consequence of diminished physical condition combined with participation in intensely competitive pick-up games. These injuries are usually soft tissue in nature; however, a predisposing spinal abnormality such as degenerative disc disease or spondylolisthesis may complicate the diagnostic picture. Competitive athletes at the high school, college, and professional levels are usually well conditioned but may ignore core strengthening and therefore also tend to suffer from soft tissue injuries to the low back.26
Meeuwisse et al. analyzed collegiate varsity basketball injuries as reported through the Canadian Intercollegiate Sports Injury Registry (CISIR) over a 2-year period. A total of 215 injuries accounted for 1508 sessions of time loss. Injury to the lumbar spine and pelvis accounted for 4.7% of injuries with 50.5 total sessions lost and average time loss of 5.05 days per injury. Injury to the thoracic spine and ribs accounted for only 1.9% of injuries with 7 total sessions lost and an average time loss of 1.75 days per injury.27 Other studies have reported a higher incidence of lumbar/hip-directed injuries. Hickey et al. reviewed injuries among female basketball players at the Australian Institute of Sport. Of the 49 elite female players followed, a total of 223 injuries over the time period of 1990 to 1995 were reported. Injury to the lumbar spine was the third most frequently injured region of the body with an incidence of 11.7%, with the most frequent diagnosis being mechanical low back pain (4.5%).28 Henry et al.28a retrospectively reviewed injuries in professional men’s basketball players over a period of 7 years, and found that back and hip injuries accounted for 11.5% of all injuries. The majority of these injuries were diagnosed as contusions. Only 1% of injuries occurred to the neck, and all were described as contusions or strained muscles.
Although less common, discogenic injury, spondylolisthesis, and fractures of the spine have been reported in basketball players. Fracture types include vertebral body compression, spondylolysis, spinous process fractures, and transverse process fractures. The prevalence of spondylolysis is reported to be as high as 9%.26,29,30
Functional considerations
Discogenic back pain may present as localized pain occurring in the dysfunction and instability phases. Nerve root irritation may eventually arise in the stabilization phase of the degenerative cascade. Spinal stenosis may occur more frequently in taller athletes than in the general population26 and may play a contributing factor. Older players with existing degenerative disc disease presenting in the stabilization phase may develop nerve root irritation and radicular symptoms.
Common fractures at the lumbar spine include transverse and spinous process, pars interarticularis, and vertebral endplate. Vertebral body compression fractures are rare in basketball, but may occur due to supramaximal axial loading of the spine.26 Spondylolysis, spondylolisthesis, and pars interarticularis injury represent a spectrum of pathologic dysfunction as described by the degenerative cascade. High-grade spondylolisthesis is rare in high-level athletes. Low-grade spondylolisthesis can occur as a consequence of pars stress fracture, which is usually isthmic in origin, but may also be traumatic or rarely pathologic in nature. These injuries are frequently accompanied by lumbar spine pain and associated with tight hamstrings and the functional adaptation complex of loss of the lumbar lordosis. Degenerative forms of this injury are more common in women and elderly populations. Slip rarely progresses beyond 33%.31
Diving
Overview
Recreational diving accidents are the fourth most common cause of spinal cord injury following motor vehicle accidents, gunshot wounds, and falls. They have caused more cases of quadriplegia than all other sports combined.32,33 In comparison, there are only two reports of fatalities in international competition in the literature, both of which occurred during platform diving. In the United States, there has been no reported fatality or catastrophic injury during supervised training or competition in over 80 years. Factors related to catastrophic injury in diving include lack of formal training, insufficient water depth, lack of supervision, and alcohol consumption.
Cervical strains and sprains, as well as brachial plexus stretch injuries can occur but are thought to be uncommon due to the protective effect of arm position during entry to the water.34 Low back pain is common in competitive divers, and in many cases may be related to spondylolysis, spondylolisthesis, or Z-joint arthropathy. Rossi performed a radiographic study of 1430 athletes, including 30 divers, and found a 63% incidence of spondylolysis in divers compared to an overall incidence of 16.7% for all athletes. This was the highest incidence of all sports in the study.16 Within the sport of diving, a higher incidence of lumbar spondylosis has been noted in platform diving when compared to springboard diving.35

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


