CHAPTER 52 The Biomechanics of the Cervical Spine during Whiplash Injury
INTRODUCTION
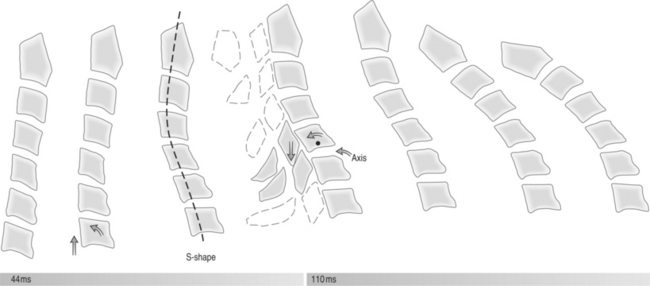
The injury mechanism associated with ‘whiplash-associated disorder’1 has been studied for over 40 years. Cervical spine injury associated with rear-end collision was first described in 1867 with railroad workers, the so-called ‘railroad spine.’ In 1928, Crowe described the cervical spine injury associated with rear-end automobile collisions.2 The theories hypothesizing the biomechanical injuries have evolved from early years when the mechanism of injury was thought to be simple cervical hyperextension.3–6 Cadaveric, anthropomorphic, and animal (including human) studies as well as mathematical models have all been used to further investigate the biomechanical events that occur during whiplash injuries. The majority of these studies focus on the association between motion and injury to the cervical spine that occurs during rear-end impact, simulating motor vehicle collisions. Factors that affect energy transfer are the basis for injury to the cervical spine in these collisions. It has become more apparent through these studies that the mechanism of injury to the cervical spine is not, in fact, simply cervical hyperextension or hyperflexion as was once thought.3–6 Investigators have shown through studies of segmental cervical spine motion that an ‘S-shaped’ cervical spine deformation occurs in the sagittal plane at approximately 50–75 ms after impact (Fig. 52.1), which includes abnormal lower cervical spine extension coupled with upper cervical spine flexion, as well as axial cervical spine compression.7–11 It is now felt that this abnormal curvature and compression of the cervical spine is the etiology of the injuries that occur during rear-end collision.
The Quebec Task Force defines whiplash as an ‘acceleration–deceleration mechanism of energy transfer to the neck. It may result from rear-end or side-impact motor vehicle collisions, but can occur during diving or other mishaps.’6 As the majority of published studies that investigate whiplash simulate rear-end collision motor vehicle accidents, this chapter focuses on the biomechanical forces and energy transfer that is associated with rear-end collision.
ANATOMIC CERVICAL SPINE
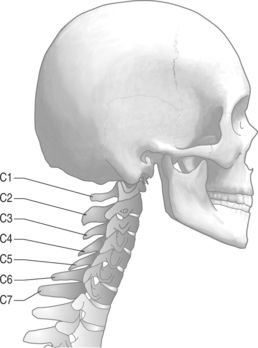
First, it is important to define the anatomic cervical spine. The cervical spine is the most mobile of any spinal section with the most physiologic lordosis.12 It is generally considered as two functional regions, the upper cervical spine, C0–2, and the lower cervical spine, C3–7 (Fig. 52.2).
As a functional unit, the upper cervical region can be broken down into two adjacent segments of motion: C0–1 and C1–2. Physiologic motion at the C0–1 level generally accommodates 25° of flexion–extension and 5° of lateral flexion. There are 3–8° of rotation that occurs about the instantaneous axis of rotation.12 Paradoxical extension at C0–1 is observed at end-range cervical spine flexion.13 The C1–2 level accommodates 20° of flexion–extension and 5° of lateral flexion. There is significantly more rotation about the instantaneous axis of rotation, approximately 40° to each side, which accounts for approximately half of the total rotation of the cervical spine.12
The middle and lower cervical spine encompasses the cervical levels C3–7. Physiologic anterior–posterior translation can be up to 2–2.7 mm from the anterior-inferior corner of the moving vertebral body.14 On flexion and extension plain films of the cervical spine, a maximum of 3.5 mm of anterior–posterior translation is accepted as normal (Fig. 52.3). This takes into account approximately 25% magnification due to radiographic technique.9 There is also physiologic coupling in the lower cervical spine between lateral flexion and rotation. Coupling occurs when motion about one axis is accompanied by simultaneous motion around another axis. In the cervical spine, lateral flexion of a vertebra is accompanied by rotation so that the spinous process moves toward the convexity of the developing curve. This coupling pattern changes from the C2 to C7 level, with the more cephalad segments having a higher ratio of rotation to lateral flexion and the more caudal segments having a lower ratio of rotation to lateral flexion.14
BIOMECHANICS OF THE REAR-END COLLISION
Researchers debated for many years as to the pathologic mechanism that leads to whiplash-associated disorder. The prevalent theories revolved around early stage hyperextension and late stage hyperflexion.3–6 These earlier studies investigated cervical spine motion as a whole during rear-end collision. As researchers began to look at individual segmental motion in the cervical spine, the abnormal posturing that occurs throughout the event was found. Grauer first described the abnormal S-shaped cervical spine curvature that occurs during rear-end collisions, with lower cervical spine flexion and upper cervical spine extension.15 The abnormal posture that occurs during this S-shaped curve is now implicated as the most likely etiology of injury in whiplash-associated disorder.9–12,16,17
The sequence of events that occur in rear-end collisions begins with the impact of the bullet vehicle, and ends with complete cervical spine flexion (Table 52.1). The energy transfer that occurs through this process causes the abnormal cervical spine curvature and compression which leads to the cervical spine injury.
Table 52.1 Typical sequence of events in rear-end collisions
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
