Monitoring
• Pulse oximetry
• SaO2 90% or less in adults or 92% or less in children indicates severe airflow obstruction
• Oxygenation may decrease with β-agonist inhalant therapy due to increases in v/q mismatch5
• Spirometry/peak expiratory flow rate (PEFR)
• Serial measurements document response to therapy
• Normal values differ with size and age
• FEV1 preferred over peak expiratory flow (PEF) if available because a low PEF cannot differentiate between obstructive versus restrictive disorders versus poor effort6
• Electrocardiography/telemetry
• Not routinely obtained
• Indication: Severely symptomatic, age 50, coexistent heart disease or COPD
• Possible findings: sinus tachycardia, right heart strain, and supraventricular tachycardia (SVT) (consider theophylline toxicity); arrhythmias other than SVT are rare3,6
Laboratory Studies
• Complete blood count with fever, purulent sputum, or other signs of infection2,3
• Leukocytosis is common with asthma exacerbations, significant stress, corticosteroid or catecholamine use
• Arterial blood gas (ABG) with severe distress, PEF 25% predicted or less, or SaO2 <90% after initial treatment3,5
• PaCO2
![]() Initially decreased due to increased respiratory drive and hyperventilation.
Initially decreased due to increased respiratory drive and hyperventilation.
![]() Normal indicates severe airflow obstruction, respiratory muscle fatigue, and increased risk of respiratory failure.
Normal indicates severe airflow obstruction, respiratory muscle fatigue, and increased risk of respiratory failure.
![]() Elevated (>42 mmHg) indicates inadequate ventilation and impending respiratory failure.3
Elevated (>42 mmHg) indicates inadequate ventilation and impending respiratory failure.3
• Serum electrolytes with coexisting cardiovascular disease, diuretic or chronic steroid use3,5,6
• Low potassium, magnesium, and/or phosphate may be secondary to frequent β2-agonist or steroid use3,5,6
• Theophylline level with current treatment5,6
• Tests for viral or bacterial infections per clinical suspicion
Imaging
• Chest x-ray (CXR)
• Not routinely recommended
• Indications (suspected complicating cardiopulmonary process): fever, leukocytosis, elevated procalcitonin, unexplained chest pain, asymmetric breath sounds, hypoxemia, subcutaneous emphysema, peripheral edema, and high-risk comorbidities (intravenous drug use, immunosuppression, granulomatous disease, recent seizures, cancer, chest surgery, and congestive heart failure)3,5,6
Differential Diagnosis
• Extrathoracic upper airway obstruction
• Anaphylaxis, postnasal drip syndrome, vocal cord abnormalities or dysfunction, hypertrophied tonsils, epiglottitis, laryngeal edema, laryngostenosis, laryngocele, postextubation granulomas, retropharyngeal abscess, peritonsillar abscess, mobile supraglottic soft tissue, obesity, tumors, Wegener granulomatosis, cricoarytenoid arteritis, abnormal arytenoid movement, relapsing polychondritis, and klebsiella rhinoscleroma2,4–6
• Intrathoracic upper airway obstruction
• Tracheal stenosis, foreign body aspiration, airway tumors, intrathoracic goiter, tracheobronchomegaly, acquired tracheomalacia, herpetic tracheobronchitis, and right-sided aortic arch2,4–6
• Lower airway obstruction
• Asthma, COPD, emphysema, pulmonary edema, aspiration, pulmonary embolism, pneumonia, bronchiolitis, bronchitis, gastroesophageal reflux disease, cystic fibrosis, carcinoid syndrome, bronchiectasis, lymphangitic carcinomatosis, parasitic infections, α1-antitrypsin deficiency, and sarcoidosis2,4–6
• Other
• Panic disorder, hyperventilation syndrome, conversion disorder, and myasthenia gravis2,6
TREATMENT
Medications
• Oxygen: Maintain PO2 >90% to 92% and >95% with pregnancy and coexistent heart disease3
• Short-acting βχ2-agonist (albuterol)
• Nebulized
![]() Intermittent: Adult 2.5 to 5 mg or pediatric 0.15 mg per kg (minimum 2.5 mg) q 20 to 30 minutes × 3 doses, then q 1 to 4 hour prn
Intermittent: Adult 2.5 to 5 mg or pediatric 0.15 mg per kg (minimum 2.5 mg) q 20 to 30 minutes × 3 doses, then q 1 to 4 hour prn
![]() Continuous: If severely ill or PEFR <200, adults 10 to 15 mg per hour or pediatric 0.5 mg/kg/h
Continuous: If severely ill or PEFR <200, adults 10 to 15 mg per hour or pediatric 0.5 mg/kg/h
• Metered-dose inhaler (MDI) with spacer/holding chamber (four to eight puffs is equivalent to one nebulized treatment)
![]() Four to eight puffs q 20 to 30 minutes × 3, then q 1 to 4 hour prn
Four to eight puffs q 20 to 30 minutes × 3, then q 1 to 4 hour prn
• Parenteral: If seriously ill with no improvement after two to three inhaled treatments; No proven benefit compared to inhaled
![]() Epinephrine: 1:1000 (1 mg per mL) adult 0.3 to 0.5 mg sq or pediatric 0.01 mg per kg (up to 0.3 0.5 mg per kg) sq q 20 minutes × 3 doses
Epinephrine: 1:1000 (1 mg per mL) adult 0.3 to 0.5 mg sq or pediatric 0.01 mg per kg (up to 0.3 0.5 mg per kg) sq q 20 minutes × 3 doses
![]() Terbutaline (1 mg per mL) adult 0.25 mg or pediatric 0.01 mg per kg sq q 20 minutes × 3 doses, then q 2 to 6 hour prn3
Terbutaline (1 mg per mL) adult 0.25 mg or pediatric 0.01 mg per kg sq q 20 minutes × 3 doses, then q 2 to 6 hour prn3
• Anticholinergics: Add to albuterol if severe bronchospasm or slow response to initial β2-agonist therapy. It is recommended for initial use in the emergency room as it may decrease hospital admission rates, but it is not recommended for hospital use3,6
• Ipratropium bromide (Atrovent)
![]() Nebulized: Adult 0.5 mg or pediatric 0.25 to 0.5 mg q 20 to 30 minutes × 3 doses, then q 2 to 4 hour prn
Nebulized: Adult 0.5 mg or pediatric 0.25 to 0.5 mg q 20 to 30 minutes × 3 doses, then q 2 to 4 hour prn
![]() MDI: Adult eight puffs or pediatric four to eight puffs q 30 minutes × 3 doses, then q 2 to 4 hour prn3
MDI: Adult eight puffs or pediatric four to eight puffs q 30 minutes × 3 doses, then q 2 to 4 hour prn3
• Corticosteroids: Start as soon as insufficient improvement with β-agonist is identified (<10% improvement in PEFR after first dose β-agonist, PEFR <70% after initial hour of treatment); start immediately in all patients currently taking oral corticosteroids; start early in pediatric population3,5
• Parenteral
![]() Methylprednisolone (Solu-Medrol, Depo-Medrol) adult 40 to 80 mg per day IV in 1 to 2 divided doses or pediatric 1 to 2 mg/kg/day IV in 1 to 2 divided doses (max 60 mg)3
Methylprednisolone (Solu-Medrol, Depo-Medrol) adult 40 to 80 mg per day IV in 1 to 2 divided doses or pediatric 1 to 2 mg/kg/day IV in 1 to 2 divided doses (max 60 mg)3
• Oral: In the absence of vomiting, efficacy is comparable to IV3
![]() Prednisone: adult 40 to 80 mg per day in 1 to 2 divided doses or pediatric 1 to 2 mg/kg/day in 1 to 2 divided doses (max 60 mg) (until PEF reaches 70% predicted)1,3
Prednisone: adult 40 to 80 mg per day in 1 to 2 divided doses or pediatric 1 to 2 mg/kg/day in 1 to 2 divided doses (max 60 mg) (until PEF reaches 70% predicted)1,3
• Inhaled: Start at discharge; do not wait until after tapering oral steroid (causes confusion and medication noncompliance)
• Methylxanthines: Not recommended owing to the increased risk of toxicity, without added benefit3,5; may consider in refractory cases; check level with current treatment
• Theophylline (Aminophylline): Adult 5 mg per kg over 20 minutes followed by continuous infusion of 0.5 to 0.7 mg/kg/hour or pediatric (≥2 years old) 5 mg per kg IV over 20 minutes followed by continuous infusion of 1 mg/kg/hour
• Magnesium sulfate: Use is controversial, results of published trials are mixed5; may consider in refractory cases; 2 g IV over 30 minutes or pediatric 25 to 75 mg per kg IV up to 2 g over 10 to 20 minutes5
• Leukotriene receptor antagonist: Not recommended as use in acute setting is unclear; small studies indicate improvement in PEFR when given with acute bronchospasm,5,6 may consider in refractory cases
![]() Montelukast: Adolescent and adult 10 mg PO, pediatric 2 to 5 years old 4 mg, 6 to 14 years old 5 mg
Montelukast: Adolescent and adult 10 mg PO, pediatric 2 to 5 years old 4 mg, 6 to 14 years old 5 mg
• Antibiotics: Not recommended without signs of complicating bacterial infection (sinusitis, bronchitis, or pneumonia)3,6
• Heliox: Mixture of helium and oxygen; may improve oxygenation in refractory cases, but not proven consistently effective5; may consider in refractory cases
• IV fluids: Only to treat dehydration; young children and infants may become dehydrated owing to tachypnea and decreased oral intake3,5
• Sedatives: Not recommended owing to respiratory suppression unless intubated3
• Mucolytics: Not recommended; may worsen cough or bronchospasm3
Nonoperative
Endotracheal Intubation and Mechanical Ventilation
• Indications:
• Absolute: apnea, coma
• Other: Altered mental status, inability to speak, increasing or decreasing pulsus paradoxus, respiratory or cardiac arrest, diaphoresis in the recumbent position, acute barotrauma, severe lactic acidosis (especially in infants), silent chest despite respiratory effort, retractions, worsening fatigue, refractory hypoxemia (PaO2 <60 mmHg on max O2), increasing PaCO2 (50 mmHg and rising >5 mmHg per hour)6; see Table 3.2-1 above for findings associated with imminent respiratory arrest.
• Risks: Laryngeal damage, high pressures causing hypotension (auto-PEEP), barotrauma, pneumothorax, pneumomediastinum
• Guidelines:
• Do not delay intubation once it is deemed necessary
• Consult with or comanagement by physician expert in ventilatory management
• Best done semi-electively, before the crisis of respiratory arrest
• Perform in a controlled setting (intensive care unit or emergency room) by experienced physician
• Maintain or replace intravascular volume to prevent hypotension caused by PPV
• Permissive hypercapnia or controlled hypoventilation (adequate oxygenation and ventilation while minimizing high airway pressure and barotrauma)
![]() Highest FiO2 as necessary to maintain oxygenation
Highest FiO2 as necessary to maintain oxygenation
![]() Accept hypercapnia
Accept hypercapnia
![]() Treat respiratory acidosis with IV sodium bicarbonate
Treat respiratory acidosis with IV sodium bicarbonate
![]() Adjust tidal volume, rate, and I:E ratio to minimize airway pressures
Adjust tidal volume, rate, and I:E ratio to minimize airway pressures
![]() Continue other therapy3
Continue other therapy3
Referrals/Consultation
• Severe, refractory, or life-threatening symptoms with intensive care unit transfer or intubation with mechanical ventilation
• Recurrent emergency department visits or hospitalizations for bronchospasm
• Atypical signs and symptoms or difficult differential diagnosis
• Other complicating conditions
• Additional diagnostic testing indicated (allergy skin testing, rhinoscopy, pulmonary function tests [PFTs], bronchoscopy)
• Additional patient education is needed (problems with adherence or allergen avoidance)
• Confirmation of occupational or environmental exposure
• Pregnant patients with severe or recurrent symptoms
• Significant psychiatric, psychosocial, or family problems that interfere with care3
Risk Management
Failure to initiate steroid therapy or intubation, monitor electrolyte balance, admit a wheezing patient with normal PCO2, treat expediently, educate patients upon discharge, and identify other diagnoses (congestive heart failure, myocarditis, multiple pulmonary embolisms, surreptitious vocal cord dysfunction, panic disorder, hyperventilation, etc.)
Patient Education
Monitoring PEFR at home with written action plan, importance of taking medication, proper medication use, proper use of inhalants and spacers, trigger avoidance, oral rinsing after inhaled corticosteroids (ICS), significance of nocturnal exacerbations, and close follow-up.3,5,6
Follow-Up
After treatment
• PEFR ≥70% and minimal or absent symptoms: Discharge with education and close follow-up; increase frequency of short-acting β-agonist (SABA), possibly start oral steroids, consider ICS.
• PEFR 40% to 69% and mild-to-moderate symptoms
• Consider for discharge: Improving lung function, low risk (good self-care skills and supportive home environment) and can obtain medications; discharge with education and close follow-up; increase frequency of SABA, start oral steroids, consider ICS.
• Hospitalize: New-onset or labile asthma, multiple prior hospitalizations or emergency room visits, past intensive care unit admission or intubation, using >2 SABA canisters in 1 month, severe symptoms that preclude self-care, lack of plan, patient difficulty understanding severity of symptoms, other complicating conditions, psychiatric disease, drug use, or adverse socioeconomic conditions.
• PERF <40%: Hospitalize3
Complications
Medication side effects, pneumothorax, pneumomediastinum, secondary infection, respiratory distress/arrest, death.
Special Considerations
• Socioeconomic factors: Inability to obtain medications or medical care can lower the threshold for admission. Consider discharging patient with medications in hand or IM steroid to avoid possible nonadherence.6
• Pediatrics: May be more difficult to determine severity of illness. Treat as aggressively as adults in appropriate dosages, give corticosteroids early, more likely to become dehydrated due to increased work of respiration.3,5
• Pregnancy: Treat as aggressively as nonpregnant women to prevent maternal and fetal hypoxia. Hypoxia and respiratory acidosis can be detrimental to both the fetus and the mother. Continuous electronic fetal monitoring is recommended when fetus is potentially viable. Obstetrical and pulmonary consultation with severe or refractory symptoms.2,8,9
REFERENCES
1. Mosby’s Medical Dictionary. 8th ed. St. Louis, MO: Elsevier; 2009.
2. Morris MJ. Asthma. emedicine (Online serial). November 18, 2013
3. Busse WN. National Asthma Education and Prevention Program: Expert panel report III: guidelines for the diagnosis and management of asthma. Bethesda, MD: National Heart, Lung, and Blood Institute; 2007. (NIH publication no. 07–4051.)
4. Weiss LN. The diagnosis of wheezing in children. Am Fam Physician 2008;77(8):1109–1114.
5. Asthma Exacerbation in Children. Dynamed (Online serial). March 10, 2014.
6. Asthma Exacerbation in Adults and Adolescents. Dynamed (Online serial). June 7, 2013.
7. Irwin RS. Diagnosis of wheezing illnesses other than asthma in adults. UpToDate (Online serial). February 20, 2014; Version 10.0.
8. American College of Obstetricians and Gynecologists (ACOG). Asthma in pregnancy. Washington, DC. American College of Obstetricians and Gynecologists; 2008. (ACOG practice bulletin #90). Retrieved from www.guideline.gov/contents.aspx?id=12630. Accessed on March 19, 2014.
9. Busse WW, Alving B, et al. National Asthma Education and Prevention Program: Working group report on managing asthma during pregnancy: recommendations for pharmacologic treatment. Bethesda, MD: National Heart, Lung, and Blood Institute; 2004. (NIH publication no. 05–5236.)
|
GENERAL PRINCIPLES
• Drug overdose is the leading cause of injury-related death in the United States.1,2
• According to the National Safety Council (www.nsc.org), drug overdose was the leading cause of death in working-age adults in 2013.
• Rapid stabilization of any suspected overdose patient is the first priority.
• Quick determination of substances used from patient, family, friends, and ambulance staff is needed to prevent delay of therapy. The initial history often correlates poorly with the definitive diagnosis; therefore, patients should have their clothing, wallets, phones, and accessories checked for pills, prescriptions, and drug-related equipment. Further information can be obtained from toxicology screens. State prescription drug monitoring databases can also be checked when available.
• Gastric lavage, emesis, whole-bowel irrigation, activated charcoal, and use of cathartics should be considered to decrease gut absorption of toxic substances. Activated charcoal is often the preferred approach initially.
• Maintaining close contact with the US Poison Control Center (national toll-free number 1-800-222-1222) or area toxicologists will likely be needed. In some cases, patients may call this number and be treated from home with assistance from the poison control center—if they have been asymptomatic, ingested a known nontoxic quantity of medication, and felt to be reliable.3
• The care team should be alert for indications of intentional overdose for self-harm or malicious intent and involve psychiatry and/or the appropriate authorities.
• Analgesics, sedatives, antipsychotics, and antidepressants are the most common drugs found in overdoses,4 not a surprise as patients prescribed these drugs are the most likely to suffer from suicidal ideation.
• Suicide attempts, poisonings, pediatric accidental ingestion, and illicit drugs are the most commonly encountered drug overdoses. Ingestion of a toxic substance, either accidental or intentional, is the most prevalent, but has a fatality rate of <1%, with only 7% of cases requiring hospitalization.4 Today’s era of drug parties, especially among teens, is causing an increase in accidental overdoses. Experimentation with common substances and production of new illicit drugs will continue to confound clinicians. Furthermore, the number of opioid-related deaths in the United States has sharply risen over the past decade.
DIAGNOSIS
Initially assess for life-threatening complications. Treatment focuses on eliminating the drug and specific antidote and drug therapy. Look for patterns of the classic “toxidromes”: sympathomimetic, anticholinergic, hallucinogenic, opioid, sedative–hypnotic, cholinergic, neuroleptic malignant syndrome, and serotonin syndromes; distinguished by physical exam, EKG changes, and unique odors. Keep in mind other causes for the patient’s signs and symptoms such as infections and electrolyte disturbances.
History
Question the patient, family, friends, and the paramedics about
• Type and/or name of the drug(s)
• Time and amount of ingestion
• Any empty bottles or drug paraphernalia found at the site
• Past medical history of other significant diseases that may complicate the overdose
Physical Examination
• Vital signs (unstable vital signs demand prompt attention)
• Smell the breath for any distinctive odors; remembering other processes such as a diabetic ketoacidosis could also be occurring
• Eyes: pupil size and reactivity, extraocular movements, nystagmus
• Heart: murmurs may indicate infective endocarditis
• Lungs: Rales point to pneumonia or pulmonary edema
• Abdomen: liver size, peripheral stigmata of chronic liver disease
• Rectal exam can be helpful in the case of “body packers” (body packers place packages of illicit drugs in body cavities)
• Skin: look for sweating, a cold or clammy feeling, and needle marks
• Neurologic examination: consciousness, gag reflex, tremors, and deep tendon reflexes
Laboratory Tests and Imaging
• Bedside blood glucose: Do not delay in treating hypoglycemia
• EKG: QRS/QTc changes that may require urgent action
• CBC
• Electrolytes, BUN, creatinine, serum osmolality (osmolar gap may occur with alcohol ingestion)
• Complete urinalysis: may show rhabdomyolysis, crystals
• Chest x-ray and arterial blood gas if any respiratory impairment
• Some toxins or drug packets can be detected on radiology plain films
• Levels of suspected agents, for example, alcohol, acetaminophen, and salicylate
• Toxicology screens on the blood, urine, and gastric contents must be obtained rapidly; many substances metabolize quickly and are not detectable within a few hours of ingestion even though their affects may be longer lasting. Suspected false-negative or false-positive results will need confirmatory testing
TREATMENT
Stabilization
• In comatose or severely compromised drug overdose patients, establish an airway and ventilate the patient immediately. In lethargic or obtunded patients, check the gag reflex and, if it is not present, intubate the patient. If no blood pressure or pulse is present, begin cardiopulmonary resuscitation and also provide airway and circulatory support. Patients should be monitored for cardiac arrhythmias, and a large-diameter intravenous line should be placed. Decontamination should be considered as an additional “D” in the secondary ABCs of cardiac life support resuscitation. The preferred option is activated charcoal (1 to 2 g per kg, max 100 g), which can decrease absorption by 70% if given within 30 minutes of ingestion and by 30% if given within 30 to 60 minutes. Gastric lavage (performed with a size 36 to 40 French tube) can be helpful but only if started within 60 minutes of the drug ingestion; there is a risk of injury to the esophagus or aspiration with this procedure. Whole-bowel irrigation with bowel prep solutions such as potassium chloride (Go-Lytely) or polyethylene glycol at a rate of 1 to 2 L per hour can be used in cases of iron intoxication, lithium overdose, or a ruptured “body pack.” If nasogastric administration of the solution is required, the patients must lay at a 45 degrees incline to help prevent aspiration. Airway protection and management is paramount in this procedure. It may take more than 5 hours to clear the contaminant; samples of the effluent from the rectum can be tested to ensure clearing of the drug. Serial blood tests may be required.
Medication
• During the initial treatment of drug overdose patients, empirically treat unconscious patients for possible hypoglycemia with 50 mL of 50% dextrose intravenous (IV). Administration of 100 mg of IV thiamine may help prevent an acute Wernicke syndrome in alcoholics; however, the myth that it “must” be given prior to the administration of dextrose has been debunked in the literature.5 For potential narcotic overdoses, give naloxone (Narcan) to any patient with respiratory depression, 0.4 mg IV; if there is no response in 1 to 2 minutes, you can give 2 mg IV, and keep repeating the dose to a maximum of 10 to 20 mg IV. A helpful mnemonic to remember for the unconscious patient is “DONT” (D=Dextrose; O=Oxygen; N=Naloxone; T=Thiamine).
Referrals/Counseling
• Local poison control centers and toxicologists are good resources throughout the treatment process and especially helpful in uncommon overdoses. Psychiatrists and psychologists should be consulted in intentional overdoses after the patient has been stabilized and cleared medically. Close monitoring, usually one-on-one supervision, may be needed after the patient has regained consciousness until they are discharged or transferred. Many emergency departments and primary care centers train staff to perform the Screening, Brief Intervention, and Referral to Treatment (SBIRT).6
Prevention
• Physicians play a critical role in preventing prescription drug overdoses. Evaluate all patients for their overdose potential. Give low-toxicity drugs to patients with a history of depression, substance abuse, previous suicide attempts, or overdoses and to those who may be more sensitive to drugs, such as elderly, young, pregnant patients, and patients on other drugs. Female patients are more likely to overdose than male patients. Give high-risk patients smaller amounts of the drug with more frequent refills. This is especially true in patients with seizure disorders requiring barbiturates, which are up to 10 times as toxic as benzodiazepines.
SPECIFIC DRUG OVERDOSE TREATMENT
Cocaine and Amphetamines
Diagnosis
• Stimulant drug overdoses present with chest pain, cardiac arrhythmias, hypertension, stroke, paranoia, seizure, severe agitation, and asthma attacks. Hyponatremia due to excess sweating may also be present. Severe cocaine intoxication may present as bradycardia and hypotension due to cardiovascular toxicity. Death is caused by cardiac arrhythmias, status epilepticus, cerebral hemorrhage, myocardial infarction, or hyperthermia. Simultaneous alcohol use increases the production of active metabolites, causing prolonged drug toxicity.7 Smugglers may swallow large bags of cocaine to prevent detection, a practice known as body packing. Rupture of the bags causes severe cocaine intoxication.
Treatment
• Treat hypertension with diazepam (Valium), 5 to 10 mg IV no faster than 5 mg per minute. If severe hypertension persists, start a sodium nitroprusside infusion, 0.5 to 10 mg/kg/minute. Hyperthermia needs to be aggressively treated with rapid cooling to prevent rhabdomyolysis and subsequent renal failure. Treat myocardial ischemia with nitroglycerin and aspirin. Consider using nitrates and calcium-channel blockers for the management of uncontrolled hypertension. β-Blockers should be used with caution for cocaine-induced chest pain or myocardial ischemia, although the theoretical risk of unopposed α-adrenergic stimulation is not supported in the literature.8 Consider thrombolytic therapy and coronary catheterization in acute myocardial infarctions.
• Treat body packers with activated charcoal (50 to 100 g in adults) and consider whole-body irrigation.
• Amphetamine psychosis, seen after “speed runs,” can be managed with diazepam, 0.1 to 0.2 mg per kg IV or, in severe cases, haloperidol (Haldol), 5 to 10 mg IM or PO (but this may cause hyperthermia and a reduced seizure threshold).
Tricyclic Antidepressants
Diagnosis
• Tricyclic antidepressants (TCAs) are frequently used in suicide attempts. Patients present often with tachycardia and hypotension, and it can be lethal due to cardiac toxicity. The classic “anticholinergic toxidrome” can be present: dilated pupils (“blind as a bat”), flushing with vasodilation (“red as a beet”), elevated temperature (“hot as hades”), confusion and delirium (“mad as a hatter”), thirst and decreased salivation (“dry as a bone”). Other symptoms include decreased gastrointestinal motility and hyperreflexia. Patients presenting with arrhythmias, altered mental status, seizures, respiratory depression, or hypotension are at high risk, requiring close monitoring and hospital admission. Think of tricyclic antidepressant overdose if the patient has a QRS interval longer than 0.12 seconds with right axis deviation on the electrocardiogram. Ventricular tachycardias should be treated with IV sodium bicarbonate. Remember that many drug overdoses involve multiple drugs and some potential causes of the “anticholinergic toxidrome” include some antihistamines, antiemetics (phenothiazines), antispasmodics, and antipsychotics.
Treatment
• Because antidepressant overdoses decrease gastrointestinal motility, do gastric lavage and give activated charcoal every 4 hours. Treat cardiac toxicity and hypotension with sodium bicarbonate, 1 to 2 mEq per kg IV bolus, until the arterial pH is 7.45 to 7.55, and if this does not control arrhythmias then give lidocaine.7 Manage seizures with benzodiazepines.
• Antidepressants such as selective serotonin-reuptake inhibitors (SSRIs) or serotonin–noradrenalin reuptake inhibitors (SNRIs) should be used in high-risk patients.
• A good suicide prevention strategy, including a crisis line to call and improved social supports, is an essential part of postdischarge care.
Ethanol and Benzodiazepines
Diagnosis
• In addition to recreational use, patients frequently use alcohol to “get the courage” to attempt suicide with other drugs. Symptoms include nystagmus, ataxia, hypoglycemia, vomiting, and coma. A blood level of 300 mg per dL causes coma in a “novice” drinker. In patients with severe coma and respiratory depression or arrest, consider the possibility of concomitant γ-hydroxybutyrate (GHB, one of the “date rape” drugs) ingestion.
Treatment
• Do a urine toxicology screen to determine whether other drugs have been ingested. Time and supportive care (which may include intubation and blood pressure support) are all that is needed for the majority of alcohol overdoses. Replenish intravascular volume depletion with good hydration and IV fluids. Benzodiazepines should be used to control agitation and systemic affects (such as seizures, hypertension and tachycardia) in alcohol withdrawal. Clonidine may also be used for autonomic symptoms. Flumazenil (Romazicon), 0.2 mg IV over 30 seconds, and repeated if needed in 1 to 2 minutes, can reverse the sedation and respiratory depressant effects in benzodiazepine overdoses, but it is rarely needed and can cause serious side effects (seizures if the patient is taking concomitant tricyclic antidepressants, and severe withdrawal effects and seizures if the patient is dependent on benzodiazepines). Temporary intubation and ventilatory support may be necessary in GHB overdoses or to prevent aspiration in sedative to hypnotic overdoses.
Opiates
Diagnosis
• Opiate overdose is an ever-increasing problem of endemic proportions in the United States. Overdose is characterized by respiratory depression, pupil constriction (which may not be seen with meperidine or diphenoxylate overdose), central nervous system depression, hypotension, and bradycardia. In severe overdose patients, apnea and pulmonary edema may occur. If alcohol has been ingested, opiate toxicity is increased. Synthetic opioids (such as Fentanyl, Tramadol, Methadone, and Oxycodone) are often not detected in standard urine toxicology screens and require confirmatory testing.
Treatment
Naloxone should be given as soon as possible. This can be effectively delivered via the intranasal (IN) (1 to 2 mg), subcutaneous (0.4 mg), intramuscular (0.4 mg), and intravenous (0.4 mg) routes. The IN route is equally effective and also a faster and safer method of delivery,8 so it is becoming part of the public health and harm reduction strategies to prevent deaths due to opioid overdose.9 It can be prescribed at the same time as prescription opioids and is being dispensed by an ever-increasing number of pharmacies. In severe overdose, symptoms may recur owing to naloxone’s half-life of 60 to 90 minutes, which is shorter than that of most opiates, requiring treatment of patients with repeated doses every 2 hours; daily maximum of 10 to 20 mg IV. There is no clearly established daily maximum dose for naloxone, but adverse effects have been noted with doses of 2 mg per kg.
Hallucinogens
Diagnosis
• Lysergic acid diethylamide (LSD), the most commonly abused hallucinogen, causes sympathetic stimulation with tachycardia, hallucinations, paranoia, fear, dilated pupils, sweating, and fever. Hallucinogen intoxication can be difficult to differentiate from acute schizophrenic symptoms. Patients taking hallucinogens usually have no history of mental illness, know that the symptoms are drug related, and have visual instead of auditory hallucinations. Patients who have been at a “rave” dance club commonly ingest LSD, methylene dioxymethamphetamine (ecstasy or MDMA), or methylenedioxyamphetamine (Eve or MDA).
Treatment
• Hallucinogens are rapidly absorbed into the bloodstream, and lavage and activated charcoal only increase agitation. Quiet reassurance helps patients to “come down.” In severe cases, diazepam or lorazepam helps to quiet patients. MDMA can cause hyperthermia and muscle rigidity that can lead to rhabdomyolysis if untreated (cool the patient, hydrate him or her, and use benzodiazepines for rigidity).
Phencyclidine
Diagnosis
• Phencyclidine (PCP) overdose patients can be challenging to manage. Patients’ behavior ranges widely, from quiet sedation to severe violence. PCP is frequently used as an adulterant in other illicit drugs, and patients may not know that they have ingested PCP. In mild intoxication, patients are lethargic, euphoric, and have hallucinations. In more severe intoxication, patients have hypertension, muscle rigidity, sweating, seizures, and coma. PCP intoxication can be suspected in any patient with nystagmus and rapidly changing behavior.
Treatment
• Because enterohepatic recirculation slows elimination, the effects of PCP last up to 24 hours. Decrease sensory input and administer activated charcoal to decrease reabsorption. Avoid the use of restraints, which can increase the risk of rhabdomyolysis. Treat violent behavior with benzodiazepines. Haloperidol may be used cautiously but it may increase muscle rigidity. Increased diuresis is advocated by some experts.5,10
Acetaminophen
Diagnosis
• This is based mostly on history but should be suspected in cases of elevated liver function tests in suspected drug overdose/intoxications. Acetaminophen is widely available and is frequently used for suicidal gestures. Many over-the-counter and prescription analgesics can contain acetaminophen and thus unintentional overdoses can also occur, so it is important to educate adults to not take more than 4 g per day from ALL sources. The toxic dose is approximately 150 mg per kg. A serum acetaminophen level should be drawn 4 hours after ingestion. Nomograms are available to help determine total ingested dose and whether a toxic and/or lethal dose was consumed, with “toxicity” progressing through four phases over a 2-week course.11 Prompt recognition of the problem and instituting appropriate therapy is necessary to prevent liver failure.
Treatment
• Activated charcoal can help if given within an hour of ingestion. N-Acetylcysteine (NAC) is the antidote of choice for acute overdose where the serum level is in the toxic range on the nomogram. It should also be given in paracetamol and N-acetyl-p-aminophenol (APAP) overdose with elevated liver enzymes and undetectable serum APAP levels as these patients are still in the toxic phase of APAP poisoning. Intravenous NAC should be considered in severe and chronic overdose situations, especially when the AST and ALT are significantly elevated.
Referrals
• Severe acute or chronic overdose may require transfer to an intensive care unit with consultation of a liver transplant team.
Ethylene Glycol and Methanol
Diagnosis
• Both ethylene glycol and methanol are used in industrial and automotive fluids (e.g., antifreeze, brake fluid, etc.). Ingestions can be either intentional or accidental. Typical symptoms are nausea, vomiting, abdominal pain, pulmonary edema, hypotension, central nervous system depression, seizures, ataxia, and coma. Visual disturbances (blurred vision, blindness, optic disc hyperemia) are hallmarks of methanol toxicity. An anion gap metabolic acidosis with osmolar gap is present with both intoxications. Calcium oxalate crystals in the urine are suggestive of ethylene glycol intoxication.
Treatment
• Aggressive supportive care is required for both substances. Stabilization and airway management must be closely monitored. Thiamine, folate, and multivitamin supplements should be used for both. Folinic acid (1 mg per kg up to 50 mg every 4 to 6 hour for 24 hours) should be used in methanol poisoning. Ethanol can be used, either orally or intravenously, to prevent metabolism of the substances to their toxic metabolites. Maintain a blood concentration of 100 to 150 mg per dL. Fomepizole (4-methylpyrazole), an inhibitor of alcohol dehydrogenase, can be used instead, with the advantage of not exacerbating the intoxicated state. Give a loading dose of 15 mg per kg IV followed by 10 mg per kg IV bolus every 12 hours; after 48 hours, the dose is increased to 15 mg per kg IV bolus every 12 hours.9 In either treatment, the therapy is continued until the concentration of methanol or ethylene glycol falls below 20 mg per dL. Hemodialysis can also be used in cases with significant or refractory acidosis, visual impairment, renal failure, and pulmonary edema. It is continued until the acidosis resolves.
Serotonin Syndrome
Diagnosis
• Serotonin syndrome is a potentially life-threatening condition, and early recognition is of paramount importance. It can result from intentional overdose with a single agent, drug interactions involving multiple agents, or recreational drug use. It often involves SSRIs or monoamine oxidase inhibitors, in overdoses or when they are combined with SNRIs, triptans, cocaine, amphetamines, psychedelics, dopaminergic agents, dextromethorphan, specific herbs, certain antiemetics, and some opioids. Serotonin syndrome is a clinical diagnosis involving a disturbance in three domains: autonomic instability (tachycardia, hyperthermia, elevated BP, diaphoresis, diarrhea, nausea); altered mental status (agitation, anxiety, sedation, delirium, seizures); and somatic effects (tremor, hyperreflexia, dysarthria, ataxia, myoclonic jerks, restlessness). Autonomic instability, in particular high fevers, can cause rhabdomyolysis, metabolic acidosis, renal failure, and disseminated intravascular coagulation.12
Treatment
• This condition requires aggressive support, including airway management, circulatory support, and seizure prophylaxis with benzodiazepines. Activated charcoal can be helpful in the setting of medication overdose. Agitation and somatic effects can be managed with benzodiazepines. Treatment with Cyproheptadine, an antiserotonergic agent, at a dose of 4 to 8 mg orally TID has been shown in case reports to reduce symptom severity.12
• Prevention of future events involves patient and provider education about drug interactions (including over-the-counter products) and avoidance of polypharmacy. Although symptoms typically resolve within 24 hours of discontinuation, drugs with long half-lives are known to interact for several weeks, requiring more aggressive or ongoing management.
REFERENCES
1. Warner M, Chen LH, Makuc DM, et al. Drug poisoning deaths in the United States, 1980–2008. NCHS data brief, no. 81. Hyattsville, MD: National Center for Health Statistics; 2011.
2. Centers for Disease Control and Prevention. Vital signs: overdoses of prescription opioid pain relievers—United States, 1999–2008. MMWR Morb Mortal Wkly Rep 2011;60:1487.
3. Frithsen IL, Simpson WM. Recognition and management of acute medication poisoning. Am Fam Physician 2010;81(3):316–323.
4. Bronstein AC, Spyker DA, Cantilena LR, et al. 2011 Annual report of the American Association of Poison Control Centers’ National Poison Data System: 29th Annual Report. Clin Toxicol (Phila) 2012;50:911.
5. Schabelman E, Kuo E. Glucose before thiamine for Wernicke encephalopathy: a literature review. J Emerg Med 2012;42:488.
6. Substance Abuse & Mental Health Services Administration. Screening, Brief Intervention, and Referral to Treatment (SBIRT). http://www.samhsa.gov/prevention/SBIRT/index.aspx. Accessed April 17, 2014.
7. Mokhlesi B, Leikin JB, Murray P, et al. Adult toxicology in critical care: part II: specific poisonings. Chest 2003;123(3):897–922.
8. Ibrahim M, Maselli DJ, Hasan R, et al. Safety of beta-blockers in the acute management of cocaine-associated chest pain. Am J Emerg Med 2013;31(3):613–616.
9. Wermeling DP. A response to the opioid overdose epidemic: naloxone nasal spray. Drug Deliv Transl Res 2013;3(1):63–74.
10. Alapat PM, Zimmerman JL. Toxicology in the critical care unit. Chest 2008;133:1006–1013.
11. Rowden AK, Norvell J, Eldridge DL, et al. Acetaminophen poisoning. Clin Lab Med 2006;26(1):49–65.
12. Frank C. Recognition and treatment of serotonin syndrome. Can Fam Physician 2008;54(7):988–992.
|
GENERAL PRINCIPLES
Definition
• Epistaxis is simply defined as bleeding from the nose.
Anatomy
• The vascular supply to the nose is through branches of both the internal and the external carotid arteries. Epistaxis is described as anterior or posterior based on the location of bleeding. About 90% of cases occur in the region of the Kiesselbach plexus along the anterior septum. The usual location of posterior bleeding is the posterior septum.
Epidemiology
• Epistaxis is the most common bleeding disorder of the head and neck region and is estimated to occur in about 60% of the population.1 Only 6% to 10% will seek medical attention and account for 0.5% of emergency department visits. Epistaxis occurs in a bimodal distribution with peaks at <10 and >50 years old.1
Etiology
• Common causes of both anterior and posterior epistaxis are divided into local and systemic factors:
• Local:
• Trauma/nose-picking
• Irritants/dry nasal mucosa (oxygen administration via nasal cannula, continuous positive-airway pressure machine use)
• Tumors
• Medications (nasal steroids, illicit medications)
• Foreign body
• Allergic rhinitis/sinusitis
• Anatomic deformities
• Vascular malformation or telangiectasia
• Systemic:
• Coagulopathies
• Blood dyscrasias (hemophilia, thrombocytopenia)
• Medications (anticoagulants/anti-inflammatories/herbals/illicit)
• Vasculitis (Wegener granulomatosis)
• Liver disease (cirrhosis)
DIAGNOSIS
Clinical Presentation
• Patients present with a range of symptoms from visible nasal bleeding to nausea, hemoptysis, and melena. Assessment of hemodynamic stability is a critical first step as some patients may require resuscitation prior to taking a history or performing a physical exam.
History
• In the stable patient, key historical questions include duration of current episode, amount of bleeding, prior history and treatment, chronic medical conditions, medications (prescription, recreational, nonprescription and herbal), recent illnesses, prior surgeries, known bleeding disorders, and recent trauma.
Physical Examination
• Unstable patients, such as patients with hypotension, tachycardia, or large amount of visible blood loss, should have intravenous catheters and fluids started and cardiopulmonary monitor placed prior to the physical exam. Instruments necessary for adequate visualization include nasal speculum, light source, suction, and irrigator. Determining location of bleeding is critical, and a thorough inspection of the turbinates and septum is mandatory.
Laboratory Studies
• Further evaluation and testing are directed by the history and physical exam. Patients with significant bleeding, known liver disease, and elderly, family history of bleeding disorder or patients on anticoagulation therapy should be evaluated with a complete blood count and prothrombin/partial thromboplastin time.2 Patients with recurrent, unexplained epistaxis should be evaluated for a hereditary bleeding disorder; von Willebrand disease is the most commonly discovered bleeding disorder.
Monitoring
• The type and amount of monitoring for patient safety is based on the resuscitation required, extent or persistence of bleeding, and comorbid conditions. Patients may require hospital admission for ongoing monitoring and treatment.
TREATMENT
• Behavioral, especially in children such as no nose-picking or foreign objects in the nose.
• Sustained compression of the nose, with the patient leaning forward for 5 to 20 minutes, is the first step to control bleeding.
Medications
• For bleeding unresponsive to compression, the next step is to achieve vasoconstriction using either oxymetazoline 0.05% or phenylephrine solution 0.5% to 1% applied directly to the mucosa or with soaked cotton/gauze. If no response, the next step is to apply topical anesthetic such as lidocaine or 4% cocaine. Chemical cautery may also be performed on easily visualized bleeding vessels. Silver nitrate sticks should be applied to the area for no more than 5 seconds to prevent destruction of healthy tissue. This procedure has limited efficacy if bleeding is profuse, and can be associated with complications such as septal perforation if applied aggressively, extensively, or on both sides of the septal wall.
Nonoperative
• For persistent anterior bleeding, the next step is nasal packing. This may be accomplished with Bayonet forceps and nonadherent gauze or expandable nasal tampons. There are many commercial packing materials available to ease insertion. Packing material is directed in a posterior to anterior manner, and folded in layers until the superior aspect of the cavity is filled. All packing material should be coated with topical antibiotic to help reduce the risk of infections such as toxin-producing Group A Staphylococcus. Other types of packing available include 3% bismuth tribromophenate (Xeroform), oxidized cellulose (Surgicell), and absorbable gelatin foam (Gelfoam). Packing may be left in place for 3 to 5 days for adequate clot formation, and moistened with normal saline frequently while in place and prior to removal.
Referrals
• All posterior bleeding and persistent anterior bleeding unresponsive to the above interventions should be referred for specialty care. Further options include posterior packing and/or vascular intervention (embolization and vessel ligation). Both methods have a high success rate between 75% and 100%.3,5
Patient Education
• Patients should be advised to return for care with any of the following: persistent bleeding, fever, hematemesis/vomiting, dizziness, dyspnea, or any concerns. Patients should also be educated on steps to help prevent future occurrences: keeping the mucosa moist with petrolatum jelly or nasal saline, avoid forceful nose blowing, no nose-picking, environmental changes (increase humidity of home/work, lower heat in sleeping areas), and avoidance of heavy lifting or straining.
Complications
• Complications include infection (localized or spread into surrounding tissues), necrosis of septum, septal hematoma, abscess formation, or septal perforation. Embolization incurs a 6% risk of complications, including cerebrovascular accident.3
Follow-Up
• Follow-up is based on the interventions performed. Packing removal should occur 3 to 5 days after placement. Consideration should also be given to repeating any abnormal lab work and following anticoagulation status for patients on warfarin.
Special Considerations
• Posterior bleeding: Posterior bleeding that does not respond to anterior nasal cavity packing occurs with 9% of cases is considered an otolaryngologic emergency, and patients are at risk for significant complications.5 Posterior packing requires special training, and is generally performed by an otolaryngologist. Foley bulb catheters or double balloon catheters are placed in combination with gauze packs to tamponade the posterior pharynx. Patients receiving posterior packing require hospitalization observation.
REFERENCES
1. Kucik CJ, Clenny T. Management of epistaxis. Am Fam Physician 2005;71:305–311.
2. Tjio E, Creagh D, Smith I. A four point questionnaire: aiding discrimination with coagulation screening in epistaxis. Emerg Med J 2013;30(5):428.
3. Barnes M, Spielmann P, White P. Epistaxis: a contemporary evidence based approach. Otolaryngol Clin North Am 2012;45:1005–1017.
4. Morgan D, Kellerman R. Epistaxis: evaluation and treatment. Primary Care Clin Office Pract 2014;41:63–73.
5. Spielmann R, Barnes M, White P. Controversies in the specialist management of adult epistaxis: an evidence-based review. Clin Otolaryngol 2012;37:382–389.
|
GENERAL PRINCIPLES
Syncope is the transient loss of consciousness accompanied by loss of postural tone, with rapid onset and spontaneous recovery caused by a brief and abrupt cessation of global cerebral blood flow.1 It should be distinguished from other conditions that cause altered consciousness, such as seizure, transient ischemic attack (TIA), stroke, vertigo, amnesia, concussion, migraine, hypoglycemia, drug or alcohol intoxication, or narcolepsy. These conditions either are associated with other distinctive symptoms or do not cause an abrupt loss of consciousness followed by spontaneous recovery.
Syncope is a symptom of one or more underlying causes. The most common cause of syncope is neurocardiogenic,2 but cardiac causes, including structural heart disease and cardiac arrhythmias, are associated with up to three times the risk of death compared with other causes of syncope.1
The evaluation of syncope in the emergency department or other outpatient setting is directed at identifying or ruling out life-threatening causes, determining which patients require emergent hospital admission and which patients need further nonemergent evaluation.3 Clinical decision rules, such as the San Francisco Syncope Rule, may help reinforce the decision to admit, but have not yet been shown sensitive enough to reduce the number of patients requiring admission.4,5
Up to 50% of patients presenting to the emergency room with syncope have no identifiable cause following their initial evaluation.5 Similar to the evaluation of chest pain, the goal of the initial evaluation of syncope is not to determine a specific cause, but rather to stratify risk.3
CAUSES OF SYNCOPE
Neurocardiogenic syncope, which is also called reflex- or neurally-mediated syncope, is caused by abnormal cardiovascular reflexes that disrupt or reverse the normal compensatory autonomic response to standing or any other situation that reduces venous return to the heart.6 Parasympathetic activity causes vasodilatation and bradycardia and overrides the normal increase in sympathetic output of the heart and blood vessels, resulting in peripheral blood pooling and right-sided heart underfilling. Vasovagal attacks are caused by stimuli such as emotional distress, the sight of blood, venipuncture, or prolonged standing. Situational syncope refers to vagal stimulation due to the Valsalva maneuver associated with coughing, sneezing, swallowing, micturition, or defecation. Carotid sinus syncope is caused by maneuvers that increase carotid sinus pressure such as head-turning, shaving, or wearing a tight collar. It is more common in the elderly and in men.7
Orthostatic syncope occurs because of a failure of the autonomic nervous system to respond appropriately to a decrease in blood pressure or to volume depletion. Causes of volume depletion include excessive sweating, vomiting or diarrhea, inadequate intake, or diuretic therapy. Autonomic dysfunction may be caused by medications, for example, β-blockers or vasodilators, chronic alcohol use, Parkinson disease, diabetes mellitus, loss of skeletal muscle tone in the elderly, and spinal cord injuries.7
Structural cardiac causes2,7 include valvular heart disease, such as severe aortic or mitral stenosis, myocardial infarction or ischemia, nonischemic dilated cardiomyopathy, hypertrophic cardiomyopathy, arrhythmogenic right ventricular dysplasia/cardiomyopathy, cardiac masses such as atrial myxoma, pericardial disease, congenital anomalies of coronary arteries, and prosthetic valve dysfunction.
Cardiovascular7 causes include pulmonary embolus, pulmonary hypertension, and acute aortic dissection.
Arrhythmogenic causes7 of syncope may cause bradycardia (sinus node dysfunction, atrioventricular system disease, implanted device malfunction) or tachycardia (atrial fibrillation, Wolff–Parkinson–White syndrome, idiopathic ventricular tachycardia, and inherited cardiac ion channel abnormalities such as Long QT or Brugada syndrome, which predispose patients to polymorphic ventricular tachycardia). Syncope due to ventricular tachyarrhythmias is associated with increased mortality and may be an ominous sign.2 Arrhythmogenic causes should be suspected if syncope occurs with preceding palpitations, if there are electrocardiogram (ECG) abnormalities, or if there is evidence of structural heart disease on physical exam or a family history of sudden cardiac death.8
Cerebrovascular disease can rarely cause syncope.9 Vertebrobasilar artery disease is more likely to cause dizziness or drop attacks (falls without loss of consciousness) and should be associated with brain stem or focal neurologic deficits, including vertigo, dysarthria, diplopia, or ataxia. Seizures can cause loss of consciousness, and seizure-like movements can be seen following a syncopal episode due to cerebral hypoperfusion. These two conditions can be difficult to distinguish and may require both neurologic and cardiovascular evaluation.1
Psychogenic pseudosyncope is also called pseudoseizure because the presentation may mimic both conditions but episodes of pseudosyncope typically occur multiple times per day, which is unlikely in the case of true syncope,7 and are associated with an underlying psychiatric disorder.
INITIAL EVALUATION
The initial evaluation of syncope should include a history and physical examination directed at ruling out other causes of altered consciousness not related to syncope (seizure, TIA, stroke, vertigo, migraine, alcohol intoxication, etc.) and looking for the above-listed causes of syncope. It should also include a 12-lead ECG.3
The history should include (a) a description of the event by the patient; (b) a description of the event by any witnesses, if available; (c) any relationship of the event to emotional distress, venipuncture, immediate or prolonged standing, exercise, cough, sneeze, swallowing, micturition, defecation, head-turning, shaving, increased neck pressure, fluid loss, inadequate intake, vomiting, diarrhea, alcohol or drug use, head injury, or other trauma; (d) any preceding symptoms such as dizziness, nausea, abdominal pain, shortness of breath, diaphoresis, chest pain, heart palpitations, blurred or double vision, visual field changes, slurred speech, limb weakness, migraine-associated auras, headache, seizure-related auras, or tonic–clonic movements; and (e) any residual symptoms such as a postictal states associated with seizures, neurologic deficits associated with cerebrovascular events or fatigue, and generalized weakness following neurocardiogenic syncope.1–3
Medications, which may cause syncope, especially if they have been added recently, include nitrates, diuretics, vasodilators, α-adrenergic and β-blockers, antipsychotic medications, tricyclic antidepressants, antibiotics that cause QT prolongation including macrolides and quinolones, and Class 1A (e.g., procainamide, quinidine) and Class 1C (e.g. encainide, flecanide) antiarrhythmics, which have proarrhythmic properties.2,3
Other important elements of the history are a past medical history of myocardial infarction/ischemia, especially with left ventricular dysfunction, congenital heart disease, and valvular heart disease, congestive heart failure, previous cardiac arrhythmia and pacemaker or defibrillator placement. A family history of sudden cardiac death raises the possibility of congenital conduction abnormalities such as long QT or Brugada syndrome.2,3
The physical examination should include (a) orthostatic blood pressure measurements to look for evidence of orthostatic hypotension, defined as a decrease in systolic blood pressure with standing of 20 mmHg or greater3; (b) differences in blood pressure or pulse between right and left arms, which can suggest subclavian steal syndrome or aortic dissection; (c) a cardiovascular examination looking for carotid bruits, the murmurs of aortic stenosis, mitral stenosis or hypertrophic cardiomyopathy, signs of left ventricular dysfunction, or irregular heart rhythms. For patients suspected of carotid sinus syncope, carotid sinus massage can be attempted for 5 seconds in a supine patient, with cardiac monitoring and intravenous access, to detect a cardiac pause of 3 seconds or a 50-mmHg decrease in systolic blood pressure and symptoms of syncope. It should not be attempted in patients with a carotid bruit or ventricular arrhythmia, or in those who have had a myocardial infarction, TIA, or stroke within the preceding 3 months.10
Other relevant parts of the physical exam are (d) the oral examination looking for tongue-biting, which might suggest seizures; (e) the abdominal examination looking for evidence of gastrointestinal bleeding; and (f) the neurologic examination looking for focal neurologic findings.2,3
A 12-lead ECG provides an assessment of cardiac rhythm, atrioventricular conduction, and previous ischemic events.2,8 Bradycardia, prolonged PR segment, or bundle branch block may signal sick sinus syndrome or heart block. Delta waves may suggest Wolff Parkinson–White syndrome. A prolonged QT segment (QTc >450 ms) may suggest long QT syndrome. ST segment elevation in leads V1 and V2 may suggest Brugada syndrome. A previous history of ischemic heart disease or evidence of such on ECG coupled with ventricular ectopy suggests arrhythmogenic causes of syncope.
FURTHER TESTING
If the initial evaluation suggests the patient is at low risk of serious outcomes and therefore does not require hospital admission, and the initial evaluation has not revealed the cause of syncope, then the goal of further evaluation becomes identification of underlying causes of syncope in order to prevent recurrences.2 Recurrences are associated with physical injuries and lower quality of life due to fear of dying and difficulty returning to activities such as driving or employment.1 Echocardiography can identify valvular heart disease, pulmonary hypertension, right ventricular hypertrophy, hypertrophic cardiomyopathy, or anomalous coronary arteries.
Exercise testing may be indicated if the event was exercise-related.
ECG monitoring is indicated if the initial evaluation suggests any underlying cardiac cause but may also be necessary in any case of unexplained syncope because an undetected arrhythmogenic cause could be life-threatening. The type and duration of ECG monitoring depend on the frequency of symptoms. Holter monitoring can record 24 to 48 hours of ECG data and may be used if syncope is occurring daily. Cardiac event monitors depend on patient triggering to record 1 to 4 minutes of ECG data before the trigger and 30 to 60 seconds of data after the trigger. They can be used for 30 to 60 days, but their dependence on patient triggering complicates interpretation.
Implantable loop recorders (ILRs) are inserted subcutaneously and record ECG data for up to 14 months. They combine patient-activated recordings of cardiac rhythm prompted by symptoms as well as device-triggered recordings of brady- and tachy-arrhythmias. Early use of ILRs in the evaluation of syncope has led to earlier identification and treatment of arrhythmogenic causes of syncope and to reduction of recurrent episodes.11
Tilt-table testing has been used to confirm neurocardiogenic syncope, but its usefulness in most cases is limited. Patients with normal initial evaluations are still most likely to have neurocardiogenic syncope whether their tilt-table test is positive or not. In patients at risk for serious injury due to recurrent syncope, further investigation of arrhythmogenic causes via ECG monitoring is warranted regardless of tilt-table results.2
Electrophysiologic testing is of low yield without a history of or evidence of heart disease on initial evaluation. It is indicated in patients with ischemic heart disease to look for inducible ventricular tachycardia.2
REFERENCES
1. Rosanio S, Schwarz ER, Ware DL, et al. Syncope in adults: systematic review and proposal of a diagnostic and therapeutic algorithm. Int J Cardiol 2013;162(3):149–157.
2. Strickberger SA, Benson DW, Biaggioni I, et al. AHA/ACCF scientific statement on the evaluation of syncope. Circulation 2006;113(2):316–327.
3. Huff JS, Decker WW, Quinn JV, et al. American College of Emergency Physicians. Clnical policy: critical issues in the evaluation and management of adult patients presenting to the emergency department with syncope. Ann Emerg Med 2007;49:431–444.
4. Saccilotto RT, Nickel CH, Bucher HC, et al. San Francisco Syncope Rule to predict short-term serious outcomes: a systematic review. CMAJ 2011;183(15):E1116–E1126.
5. Kessler C, Tristano JM, De Lorenzo R. The emergency department approach to syncope: evidence-based guidelines and prediction rules. Emerg Med Clin North Am 2010;28(3):487–500.
6. Kapoor W. Syncope. N Engl J Med 2000;343:1856–1862.
7. Puppala VK, Dickinson O, Benditt DG. Syncope: classification and risk stratification. J Cardiol 2014;63(3):171–177.
8. Ruwald MH, Zareba W. ECG monitoring in syncope. Prog Cardiovasc Dis 2013;56(2):203–210.
9. Arthur W, Kaye GC. The pathophysiology of common causes of syncope. Postgrad Med J 2000;76:750–753.
10. Puggioni E, Guiducci V, Brignote M, et al. Results and complications of the carotid sinus massage performed according to the method of symptoms. Am J Cardiol 2002;89:599–601.
11. Hong P, Sulke N. Implantable diagnostic monitors in the early assessment of syncope and collapse. Prog Cardiovasc Dis 2013;55(4):410–417.
|
GENERAL PRINCIPLES
Definition
As defined by the Zurich Consensus Statement in 2012:1
Concussion is a brain injury defined as a complex pathophysiological process affecting the brain, induced by biomechanical forces. Several common features that incorporate clinical, pathologic, and biomechanical injury constructs may be utilized in defining the nature of a concussive head injury including:
1. Concussion may be caused by a direct blow to the head, face, neck, or elsewhere on the body with an “impulsive” force transmitted to the head.
2. Concussion typically results in the rapid onset of short-lived impairment of neurological function that resolves spontaneously. However, in some cases, symptoms and signs may evolve over a number of minutes to hours.
3. Concussion may result in neuropathological changes, but the acute clinical symptoms largely reflect a functional disturbance rather than a structural injury and, as such, no abnormality is seen on standard structural neuroimaging studies.
4. Concussion results in a graded set of clinical symptoms that may or may not involve loss of consciousness. Resolution of the clinical and cognitive symptoms typically follows a sequential course. However, it is important to note that in some cases symptoms may be prolonged.
Epidemiology
Approximately 1.7 million people sustain a traumatic brain injury in the United States every year.2 The majority of these are mild and may occur from simple falls, automobile accidents, as well as in both competitive and recreational sports.
Classification
There is no classification schema as the older grading scales have been abandoned.
DIAGNOSIS
History and Physical
Ascertain the details of the fall or sudden trauma to the head or body, usually of low velocity, resulting in onset of clinical symptoms. Symptoms may include lightheadedness, gait or balance disturbances, dizziness, headache, nausea, or feeling like in a fog.
Physical Examination
A complete neurological examination (including gait and balance testing), mental status examination, and testing of cognitive functioning should be performed and repeated as clinically indicated. You should be specifically looking for any alteration of consciousness, inability to focus, amnesia, slowed reaction time, incoordination, slurred speech, delayed responses, disorientation, and memory deficits.
Seizures may have occurred and, although frightening to bystanders, are usually benign and seldom indicative of structural intracranial pathology.1,3
Imaging
The Canadian CT Head Rule recommends that a head CT is required only for patients with minor head injuries (defined as witnessed loss of consciousness, definite amnesia, or witnessed disorientation in a patients with a Glasgow Coma Scale [GCS] score of 13 to 15) with one of the following:
• GCS <15 at 2 hours postinjury
• Suspected open or depressed skull fracture
• Any sign of basilar skull fracture (hemotympanum, raccoon eyes, battle’s sign, CSF oto-/rhinorrhea)
• ≥2 episodes of vomiting
• Age ≥65
• Retrograde amnesia to the event ≥30 minutes or involves a “dangerous mechanism” (pedestrian struck by motor vehicle, occupant ejected from motor vehicle, or fall from >3 feet or >5 stairs.)
Neuropsychological (NP) Testing
This has been shown to have clinical value and provides significant information helpful in the management of a concussed individual, particularly adults. However, although it is a useful instrument, NP testing should not be relied upon solely to make management decisions. This would be useful particularly in patients who have a history of multiple or frequent concussions, and/or prolonged symptoms.1,4 There are several such instruments, including ImPACT, a computerized neurocognitive assessment useful in assisting medical professionals in determining an athlete’s ability to return to play (RTP). ImPACT is widely used in college and professional sports.5
Sport Concussion Assessment Tool—3rd Edition
The SCAT3 is a standardized tool useful in the evaluation of a concussed athlete and may be used for athletes over the age of 13 years.6 There is also a version for those 5 to 12 years of age, the Child-SCAT3.7
Differential Diagnosis
Heat illness, migraine headache, muscle contraction headache, sickle-cell crisis related to exertion (particularly in hot, humid conditions or at altitude), and acute anxiety can be diagnosed.
TREATMENT
Modifiers
Certain factors may signal a more prolonged course and suggest taking a more conservative approach, including the frequency, number, and severity of previous concussions; loss of consciousness >1 minute; seizure activity; age under 18 years; high-risk sports; concussions occurring from lesser force than the previous ones (e.g., simply tapping someone’s helmet in a huddle); duration of symptoms >10 days; dangerous style of play; requirement of medications; and history of recent previous concussion.
Cognitive and Physical Rest
Important in the management of concussion is allowing time for the brain to recover.1,8 This should begin immediately following the concussive event and continue with slow return to activity over 7-day period. This includes avoiding reading, watching television, video games, and even school work. When the student returns to school, adjustments should be made, such as giving frequent breaks, reducing brightness at computer screens, allowing more quiet time, and allowing extra time to complete academic tasks. A useful reference created by the CDC may be found at http://www.cdc.gov/concussion/pdf/TBI_Returning_to_School-a.pdf.
Return to Play
Recent consensus1 recommends a gradual RTP. Unlike in the past, a player who has suffered a concussion is never recommended to RTP on the day of the injury.
Returning to competitive or recreational sport activity requires medical clearance and full restoration of both cognitive and functional abilities. A phased return to activity can start when the patient is asymptomatic, has no academic restrictions, and has been cleared by a healthcare provider. Each phase should occur over a 24-hour period with progress to the next level if the patient remains asymptomatic: (a) no activity, (b) light aerobic exercise, (c) sport-specific exercise, (d) noncontact training drills, (e) full-contact practice and (f) RTP. If symptoms recur during any phase, the player should return to the previous asymptomatic phase and try to progress again only after a further 24-hour period of rest.
In an individual with repeated concussions, management should be similar, but a more conservative approach to return to activity is warranted.
Medications
Any medications or substances (e.g., alcohol, drugs) affecting the nervous system should be avoided. Acetaminophen and over-the-counter nonsteroidal anti-inflammatory drugs may be considered as they are fairly effective and safe.
Parental Education
The concussed individual should remain in the presence of a responsible adult for 6 to 8 hours, following the event to monitor for any signs of neurological deterioration.
In the past, sleeping was prohibited, which obviously interferes with cognitive and physical rest. However, observations should be made every few hours for signs of deterioration, such as labored breathing, increasing pulse, worsening headache, focal signs, balance problems, visual disturbance, or pupillary changes.
Prevention
Although mouth guards have been shown to prevent orofacial and dental injuries, there is no good evidence demonstrating that protective equipment, including helmets, will prevent concussions.1 Athletes, parents, and coaches should be well informed concerning the significance of concussions and promote proper sporting techniques and avoidance of risky and/or hazardous play.
Recovery
The vast majority of those affected (80% to 90%) recover within a 7- to 10-day period of time. Children and adolescents may take longer to reach complete resolution.1 Those symptomatic concussions falling outside of this 10-day period should be managed in a multidisciplinary fashion by clinicians with knowledge and experience in this area.
REFERENCES
1. McCrory P, Meeuwisse WH, Aubry M, et al. Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br J Sports Med 2013;47:250–258.
2. Centers for Disease Control and Prevention. Injury Prevention & Control: Traumatic Brain Injury. http://www.cdc.gov/TraumaticBrainInjury/index.html. Accessed February 24, 2014.
3. Lee ST, Lui TN. Early seizures after mild closed head injury. J Neurosurg 1992;76:435.
4. Echemendia R, Iverson GL, McCrea M, et al. Advances in neuropsychological assessment of sport-related concussion. Br J Sports Med 2013;47:294–298.
5. The Impact Test. http://www.impacttest.com. Accessed May 13, 2014.
6. Sport Concussion Assessment Tool—3rd edition. http://bjsm.bmj.com/content/47/5/259. Accessed May 13, 2014.
7. Child—Sport Concussion Assessment Tool—3rd edition. http://bjsm.bmj.com/content/47/5/263. Accessed May 13, 2014.
8. Schneider KJ, Iverson GL, Emery CA, et al. The effects of rest and treatment following sport-related concussion: a systematic review of the literature. Br J Sports Med 2013;47:304–307.
9. Stiell IG, Wells GA, Vandemheen K, et al. The Canadian Head CT Rule for patients with minor head injury. Lancet 2001;357:1391–1396.
| Fractures Requiring Special Consideration |
FRACTURE BASICS
Classification of Fractures
It is important to classify fractures accurately in order to properly communicate with consultants. They are described by fracture location, type, and amount of the displacement. Fracture location is usually related to anatomical landmarks or is described as involving the proximal, middle, or distal thirds of long bones. Closed (simple) fractures have no skin disruption that communicates with the bone, whereas open (compound) fractures do disrupt the skin. Complicated fractures are those with associated soft-tissue injuries. Avulsion fractures occur when a tendon or ligament pulls away from the bone with an attached fragment. Alignment refers to the relationship of the longitudinal axis to the fracture fragments. Abnormal alignment is described by degrees of angulation. Position describes the relationship of the fragments to their normal location. Displacement describes the abnormal position of the fracture fragments. Impacted fracture fragments are pushed together, whereas distracted fracture fragments are pulled apart. Direction of fracture lines is indicated by the terms transverse, oblique, comminuted, and spiral. Transverse fracture lines are perpendicular to the axis of the bone, and oblique fracture lines cross the axis of the bone at an angle. Comminuted fractures have more than two fragments. Spiral fractures result from a torsional force.
Clinical Diagnosis of Fracture
The diagnosis of fracture should be considered any time there is a history of significant acute or chronic injury to a bone, resulting in the complaint of pain. Signs of fractures include localized pain, tenderness, ecchymosis, or edema. Gross deformity, decreased function, abnormal mobility, and crepitus may also be present. Do not dismiss the possibility of a fracture because it cannot be immediately visualized on a radiograph. A careful examination for associated injuries to viscera, tendons, nerves, and blood vessels should always be included. Always suspect domestic violence if the mechanism of injury does fit the clinical presentation.
Imaging Techniques
Most fractures can be adequately visualized on plain radiographs, but some fractures require special imaging techniques. Radionuclide bone scanning is a very sensitive but nonspecific tool in the evaluation of fractures. Ultrasound is a newer tool for point-of-care testing in diagnosing fractures.1 Computed tomography (CT) and magnetic resonance imaging (MRI) are used to evaluate suspected fractures in bones that are frequently obscured by overlying structures. CT scanning is helpful particularly in confirming fractures of the pelvic and facial bones. MRI is now considered the most sensitive modality used to diagnose occult fractures or injuries to cartilage, ligaments, and tendons.
Treatment Generalities
Stability
Stable fractures are those that maintain their position and alignment. Unstable fractures are those that tend to displace and require early immobilization. If there is any doubt about the stability of a particular fracture, it should be treated as unstable until definitive diagnosis is obtained.
Associated injuries must also be considered in the evaluation of any fracture. A detailed examination for damage to nearby viscera, nerves, blood vessels, tendons, and overlying skin must be performed. The management of traumatized viscera may take precedence over fracture management. Neurovascular injuries should be recognized early and referred for repair. Most tendon ruptures also require surgical treatment. Open fractures require special consideration because even a small skin defect that communicates with the fracture greatly increases the patient’s chances of developing osteomyelitis. These wounds should generally be debrided in the operating room and the patients given prophylactic antibiotics.
Reduction is the procedure that returns displaced fracture fragments to acceptable position and alignment. What constitutes acceptable position and alignment varies with the fracture location and type, patient age, and the functional demands placed on the bone. A neurovascular examination should always be repeated after reduction.
Immobilization of fractures is initially achieved by splinting to provide pain relief and to prevent further displacement, associated injuries, and risk of fat emboli. Definitive immobilization can be achieved through internal or external fixation. Internal fixation requires a surgical procedure. External fixation is provided by splinting or casting. Choosing the correct type and length of immobilization is critical for optimal healing. Inadequate immobilization can result in displacement, delayed union, or nonunion of fracture fragments. Prolonged or improper immobilization can result in stiffness and functional impairment. Consultation should be obtained if there is doubt about the appropriate type and length of immobilization.
SKULL FRACTURES
General Principles
Definition
Fracture to any of the eight cranial bones: parietal, temporal, occipital, frontal, sphenoid, and ethmoid bones. Skull fractures are categorized by location (basilar vs. the skull convexity), pattern (linear, depressed, or comminuted), and whether they are open or closed. Complicated skull fractures are those that are open or depressed, those that involve a sinus, and those that cause intracranial air.
Diagnosis
Physical Examination
Basilar skull fractures are fractures of the base of the skull and may be manifested by a cerebrospinal otorrhea or rhinorrhea, mastoid ecchymosis (Battle sign), periorbital ecchymosis (raccoon eyes), hemotympanum, vertigo, hearing deficit, and seventh nerve palsy. Nasal discharge that is positive for glucose indicates a basilar skull fracture with cerebrospinal fluid (CSF) leak. A CSF leak can create a “ring sign” when bloody fluid is placed on a tissue or filter paper. If there is CSF mixed with the blood, it will move by capillary action further away from the center than the blood creating a halo or the “ring sign.” Intracranial injury should always be suspected, and a careful assessment of the patient’s neurologic status should be performed, including the use of the Glasgow Coma Scale.
Imaging
Skull radiographs should be obtained, but if they are negative and a fracture is strongly suspected, a CT scan should be obtained immediately. CT scan should also be obtained if the patient exhibits altered mental status, focal neurologic deficits, signs of a basilar skull fracture, seizures, or a palpable depression of the skull.
Treatment
Scalp lacerations may hemorrhage and should be controlled as rapidly as possible, as the rich blood supply to the scalp can result in massive blood loss. Direct pressure can be used, as well as lidocaine with epinephrine infiltrated locally. Vessels can be clamped or ligated if necessary. Open fractures should be carefully cleaned and repaired. Gentle wound exploration should be performed, with care taken not to drive bone fragments into the brain. Use of prophylactic antibiotics following an open skull fracture is controversial. In the case of a basilar skull fracture with a CSF leak, prophylactic antibiotics have not been shown to prevent meningitis and therefore are not indicated.2 Fractures depressed beyond the thickness of the skull require operative repair. Closure of an open fracture should be undertaken only in consult with a neurosurgeon if a CT scan has not been obtained. Fractures that cross the middle meningeal artery or a major venous sinus may require neurosurgery expertise. Occipital fractures have a higher rate of subarachnoid hemorrhage, and neurosurgery should be involved. Patients with a basilar skull fractures or altered mental status should be hospitalized. Periorbital and mastoid ecchymosis are often absent initially but may develop over the course of a few hours. Most CSF leaks resolve within a week. Complications from skull fractures include intracranial injury, infections, and seizures.
MAXILLOFACIAL FRACTURES
General Principles
• Anatomy: Facial bones include the zygoma, maxilla, lacrimal bone, nasal bone, mandible, sphenoid, frontal, ethmoid, and palatine. Cranial nerves II, III, and VI, and branches of V course through the orbital foramina and may be compromised in orbit fractures.
Diagnosis
History and Physical Examination
Ask the patient whether he or she is having symptoms of abnormal vision, facial numbness, or abnormal alignment of the teeth. Pain on eye movement suggests injury to the orbit or globe. Inspection should evaluate facial alignment and cranial nerve VII function, which may present with unilateral facial weakness. Palpate the face looking for any tenderness or crepitus.
Imaging
Plain films or CT scan may be helpful, but should only be completed after management of head, chest, and abdominal trauma.
Treatment
• Airway: Always secure the airway first with maneuvers such as chin lift, jaw thrust, and oropharyngeal suctioning. With severe mandible fractures, the tongue may obstruct the airway and may need to be pulled forward. If the C-spine has been cleared, the patient with tongue obstruction from a flail mandible may need to sit upright and lean forward in order to breathe. Be careful not to get distracted from the routine trauma protocol by gross facial injuries. Avoid nasotracheal intubation as an injured cribriform plate may penetrate into the brain. Rapid sequence intubation (involving anesthesia) is risky in facial trauma because bag-valve mask may be insufficient if intubation fails, so awake intubation may be necessary. You should be prepared for cricothyroidotomy should intubation fail.
• Nasal fractures: In all cases involving nasal trauma, inspect the septum for a hematoma. If present, anesthetize with a topical anesthetic, incise the inferior portion of the hematoma and allow it to drain, then pack the nose with Vaseline gauze to prevent reaccumulation of blood. Nasal films are optional; however, a referral to an ear, nose, and throat (ENT) specialist is needed only if there is significant deformity or difficulty breathing through the nose requiring reduction of the nasal fracture. The best time for reduction may be within the first 3 hours immediately following injury. If not, waiting 7 days to allow reduction of edema and swelling is preferable. If reduction is not possible within the first 7 to 10 days, then the fracture starts to heal, making reduction difficult.3
• Orbital fractures: Blowout fractures typically occur after blunt trauma to the eye or eyelids that is transferred to the weak floor of the orbit. This allows for the contents of the orbit to herniate through the floor, which may cause limitations in eye motion. Damage to the infraorbital nerve may cause anesthesia of the upper lip, nasal mucosa at the vestibule, lower eyelid, and maxillary teeth. If subcutaneous emphysema is found, suspect a sinus or facial fracture and consider starting antibiotics appropriate to sinus pathogens. Patients should avoid blowing their nose to prevent accumulation of subcutaneous air. An orbital series, which includes a Waters view, is generally no longer used; however, a CT evaluation is generally diagnostic for orbital fractures, and if positive, ENT referral should be made. Examine pupils for reactivity and whether the pupils line up in the horizontal plane. A teardrop-shaped pupil indicates a penetrated globe. Extraocular motions should be evaluated for restriction or pain. Visual acuity should be assessed using the Snellen chart, finger counting, and light perception. The swinging flashlight test may indicate optic nerve or retinal injury if the pupil initially dilates rather than constricts. If traumatic optic neuropathy is suspected, emergency ophthalmic consultation should be made in an effort to prevent blindness. Subconjunctival hemorrhage is often present with periorbital fractures. Widening of the distance between the medial canthi or pupils portends serious orbital injury.
• Naso-ethmoidal-orbital fractures (NEO): Suspect NEO injuries in those with trauma to the bridge of the nose or medial orbital wall. These fractures may involve lacrimal disruption and dural tears. A maxillofacial or ENT surgeon should be consulted if physical exam or CT scan suggests an NEO injury.
• Zygomatic fractures: Lateral subconjunctival hemorrhage often accompanies zygomatic fractures. Arch fractures are common and may be seen on arch view radiographs; these can be managed on an outpatient basis. Tripod fractures involve the infraorbital rim, diastasis of the zygomatic-frontal suture, and disruption of the zygomatic–temporal junction and are more serious. The eye may tilt when the fragment is displaced inferiorly. Tripod fractures can be seen on Waters view, and require admission for open reduction and internal fixation.
• Mandibular fractures: Fractures are often multiple because of the ring shape of the mandible. Malocclusion and pain on jaw movement indicate fracture. Lower lip and lower dental anesthesia occurs with mandibular fractures. Intraoral lacerations should be examined to determine whether the fracture is open or closed. Intravenous antibiotics should be started with open fractures, whereas closed fractures may be managed on an outpatient basis after consultation with an oral surgeon. If the patient has normal occlusion and a negative tongue-blade test, panoramic radiographs may be unnecessary. The tongue-blade test consists of having the patient bite down forcefully on a tongue blade. The physician then twists the tongue blade in an attempt to break the blade. Patients with an intact mandible will break the blade, whereas patients with a broken jaw will reflexively open their mouth.4
• Maxillary fractures: Fractures of the maxilla require high impact and are usually associated with multisystem trauma. Facial stability can be assessed by rocking the maxillary arch and simultaneously feeling the central face for movement with the opposite hand. Fractures of the midface may require manual reduction of the face to stem bleeding; the hard palate can be grasped at the maxillary arch and fragments realigned.
Special Circumstances
• Penetrating facial trauma: Gunshot wounds to the face may injure the oral cavity, and intravenous antibiotics should be given against oral flora.
• Children: Suspect nonaccidental trauma in cases of pediatric maxillofacial injury. Young children have a higher incidence of frontal bone injury due to its prominence, whereas adolescents have more midface fractures as their sinuses form. Cricothyroidotomy should be avoided in children younger than 12 as they are at higher risk for subglottic stenosis and tracheomalacia. Early fracture follow-up is important in all pediatric facial fractures as a child’s facial skeleton heals quickly and can make delayed reduction difficult.
NECK FRACTURES
Cervical spine immobilization should always be performed when neck injury is suspected. Clinical exam of the cervical spine should involve palpation of the vertebrae and assessment of range of motion (ROM). In order to clear the C-spine, use validated clinical criteria such as the Canadian C-Spine Rule.5 Obtain C-spine films if any the following are present: age >65 years, dangerous mechanism (fall from elevation ≥3 feet/5 stairs, axial load to head, MVC high speed [>100 km per hour], rollover, ejection, motorized recreational vehicles, bicycle struck, or collision), or parasthesia in extremities. If the patient is at low risk (simple rear-end MVC, sitting position in ED, ambulatory at any time, delayed onset of neck pain, and absence of midline C-spine tenderness), then assess clinically with ROM testing. If the patient does not fit these low risks or patient unable to rotate neck 45 degrees, then radiographs are mandatory. Views should include anteroposterior (AP), odontoid, and a lateral cervical radiograph that adequately demonstrates all seven cervical vertebra. To interpret films comfortably, remember the normal curves of the cervical spine (Figure 3.7-1): anterior and posterior vertebral body lines should form a smooth, continuous, lordotic curve, and the posterior cervical line should be a straight line connecting the bases of C1, C2, and C3. If the bases miss the line by more than 2 mm in either direction, suspect a pathologic process. Careful observation of these lines, along with the odontoid, can help the clinician rule out cervical fractures. If there is any doubt about the possibility of a significant cervical injury after viewing the cervical films, proceed with neurosurgical consultation while maintaining immobilization.
THORACOLUMBAR FRACTURES
Isolated, stable fractures that do not typically involve neurologic deficits include transverse process fractures, spinous process fractures, and pars interarticularis fractures. More serious fractures include wedge compression fractures, Chance fractures (involves the spinous process, lamina, transverse process, pedicles, and vertebral body), burst fractures, flexion distraction injuries (loss of height in the anterior portion of the vertebra with increased interspinous spaces posteriorly), and translational injuries (translation of vertebral segment on subsequent segments). Plain radiographs are generally adequate to make the diagnosis, although a CT scan may be required. Patients found to have unstable acute spine fractures or a fracture with a spondylolisthesis, generally require hospital admission for further evaluation, treatment, and control of pain. They will benefit from bed rest (for at least 24 hours, longer in more significant fractures), analgesics (often liberal use of narcotics is necessary to control pain), and careful and serial neurologic reassessment. In the presence of neurologic deficit, emergent neurosurgery or orthopedic consultation is necessary.
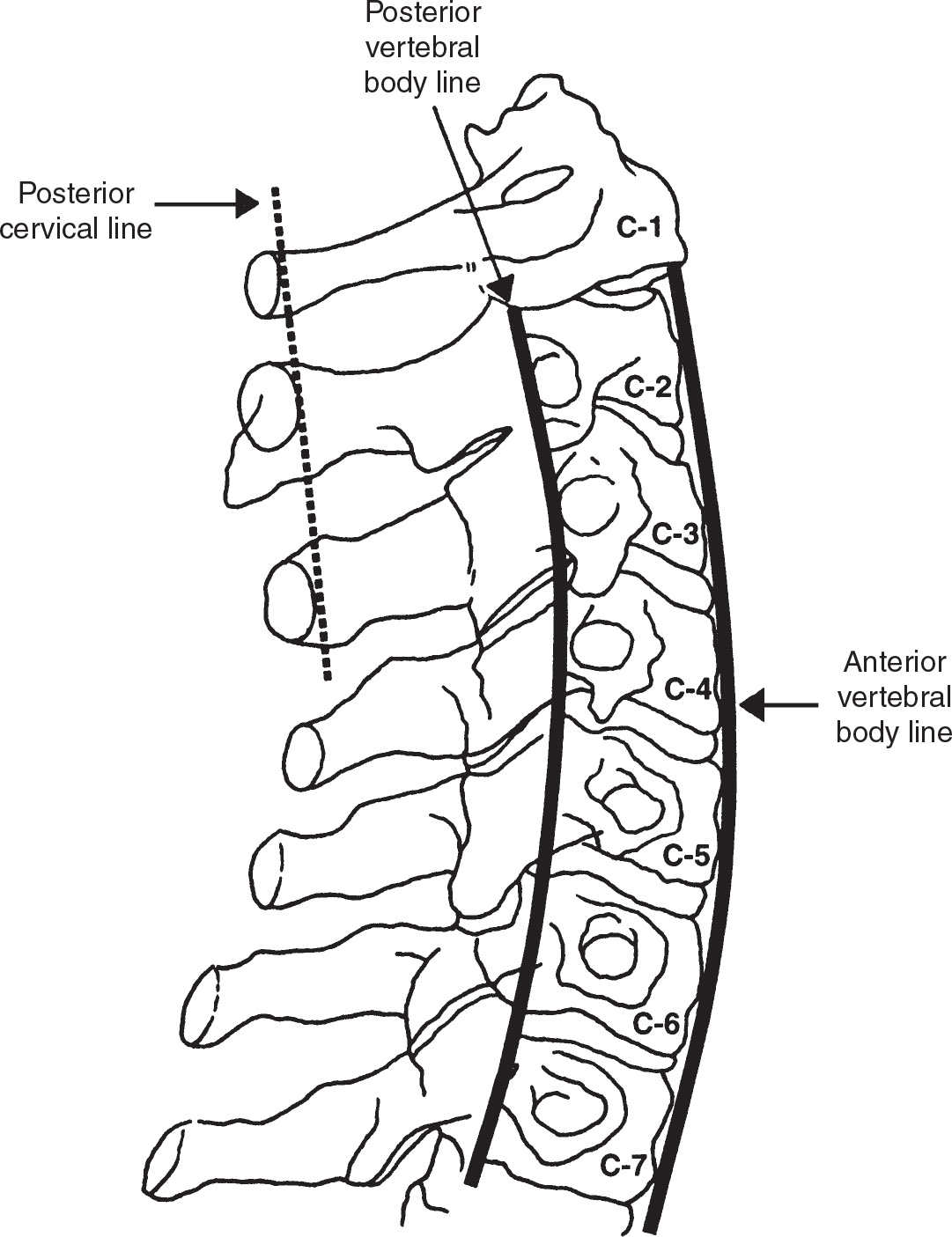
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


