REFERENCES
1. Sturchler DA. Exposure—a guide to sources of infection. Chapter 4. Invertebrates. Herndon, VA: ASM Press; 2006:85.
2. Chapel TA, Katta R, Kuszmar T. Pediculosis pubis in clinic for treatment of sexually transmitted disease. Sex Transm Dis 1979;6:257.
3. Jones JG. Chiggers. Am Fam Physician 1987;36(2):149.
4. Dermatology: Antiparasitics (Topical), In: Tarascon Pocket Pharmacopoeia 2013 Edition. 14th ed. Burlington, MA: Jones & Bartlett; 2013:149–150.
5. Ivermectin (Sklice) topical lotion for head lice. Med Lett Drugs Ther 2012;54:61–63.
6. The Medical Letter. Drugs for parasitic infections. 3rd ed. New York: The Medical Letter; 2013:55.
7. Currie BJ, McCarthy JS. Permethrin and ivermectin for scabies. N Engl J Med 2010;362(8):717.
|
GENERAL PRINCIPLES
Definition
A very common follicular disorder, particularly in adolescents.
Anatomy
Blocked pilosebaceous unit that leads to retained sebum and distention (comedones), inflammation (papules and pustules), or hypertrophy of sebum glands (nodules and cysts).1
Epidemiology
Extremely common—found in about 85% of patients between 15 and 24 years old.
Classification
Mild (noninflammatory): primarily comedones; moderate (inflammatory): primarily papules and pustules; severe (nodulo-cystic): primarily nodules and cysts.1
Pathophysiology and Etiology
Hypercohesive keratinocytes block follicular opening of pilosebaceous unit. This may be idiopathic or aggravated by androgens. The organism Propionibacterium acnes may proliferate and lead to inflammation.2
DIAGNOSIS
Clinical Presentation
Patients may present with a wide range of severity, sometimes very distressed over minimally visible lesions and at other times with minimal distress over marked physical findings.
Physical Examination
Most commonly found on the face, but may include the back, shoulders, and anterior chest wall; these areas should be examined to determine the extent of the disorder.
Differential Diagnosis
Acne vulgaris starts with microcomedones that then develop into comedones, papules, and pustules. In the absence of comedones, one should consider acne mechanica, steroid acne, or rosacea. Pustules and/or nodules in the perioral and nasal area that are unresponsive to typical antibiotic treatment for acne should lead to the consideration of Gram-negative folliculitis. Bacterial cultures may be used in establishing this diagnosis.1
TREATMENT
Behavioral
Avoid excess scrubbing of the skin, which can aggravate the condition; acne is not due to poor hygiene. There is no good evidence that diet affects acne. Avoid “picking” or “popping” as these can increase the likelihood of scarring. There is also an association between smoking and acne severity.1
Medications
Choice of medication is based on several factors: (a) the predominant lesion and skin type, (b) the distribution of lesions, (c) the patient’s preferences that will affect compliance, and (d) some degree of trial and error.
• Benzoyl peroxide preparations (soaps, lotions, gels) used once or twice a day are an excellent starting point for all types of acne. There are many preparations available over the counter or as a prescription. The strengths range from 2.5% to 10%, with increased drying of the skin associated with higher concentrations (there is no increase in efficacy). The water-based preparations are also less drying. Benzoyl peroxide may also be used in conjunction with topical or oral antibiotics as it decreases bacterial resistance.1–3
• Mild or comedonal acne. This is best treated with a topical retinoid, such as tretinoin, adapalene, or tazarotene applied thinly at bedtime. Always start with the lowest dose and increase strength over several weeks or months as needed and as tolerated. Erythema and irritation are common at first and can be minimized by decreasing frequency to every other day or every third day as needed. The gel and alcohol forms are more dry, and stronger. They are best used in patients with relatively oily skin or when creams fail. Azelaic acid has keratolytic, antibacterial, and anti-inflammatory properties and has shown efficacy with both mild and moderate acne. It may lead to hypopigmentation, which can be advantageous in those prone to postinflammatory hyperpigmentation, but can be a problem in ethnic groups with more skin pigment. Azelaic acid is pregnancy category B and may be considered for selected use in pregnant women.2–5
• Moderate or inflammatory (papular and pustular) acne. This calls for the addition of antibiotics. Oral and topical agents can be used, depending on how widespread the lesions are and whether the patient prefers oral or topical therapy. Topical antibiotics are applied thinly bid after washing (with benzoyl peroxide agent) and drying the skin. Common preparations are available as solutions, gels, lotions, ointments, and creams, including erythromycin, clindamycin, and sulfacetamide. Choice of the vehicle should depend on the patient’s skin type. Those with oily skin may do better with the drying effects of gels and solutions, whereas those with dry skin may do better with the moisturizing effects of lotions, creams, and ointments. Topical erythromycin and clindamycin are most effective when used with benzoyl peroxide and there are commercial preparations that combine these into one. Topical dapsone has also been approved for use in acne; it has antimicrobial and anti-inflammatory effects.2–5
• Oral antibiotics are indicated when lesions are widespread (making topical application impractical) or severe. First-line agents include tetracycline or erythromycin at 1 g per day in divided doses. Tetracycline may cause photosensitivity, and qid dosing on an empty stomach makes compliance difficult. Gastrointestinal (GI) upset can be common with erythromycin, and increasing resistance is noted with this agent. Minocycline 50 to 100 mg qd-bid, or doxycycline 50 mg (occasionally 100 mg) qd-bid, and less commonly trimethoprim–sulfamethoxazole 160/800 mg bid can be helpful. Oral agents are generally stronger than topical agents and can be used when topicals fail.2,3,5
• Nodulocystic acne, the most severe form of acne vulgaris, can cause emotional and physical scarring. Treatment starts with judicious use of the agents above, but the condition can often be resistant to these therapies. When this happens, oral isotretinoin may be indicated; see special considerations below.
• Oral contraceptives (OCs) and other hormonal agents. Several combined OCs are FDA-approved for use in acne. These have low doses of estrogen and nonandrogenic progestins, such as norgestimate, levonorgestrel, or desogestrel. (Progestin only contraceptives may worsen acne.) Therapy must be used for 2 to 4 months to see effects.
The diuretic spironolactone has antiandrogenic properties and has been found to be useful in the treatment of acne as well.1,2,5
Counseling
The potential physical disfigurement from acne, whether temporary from the current lesions or from scarring, can be extremely distressing for the adolescent who is developing a self-image and who may be very self-conscious. The psychological trauma from acne for a developing adolescent should not be underestimated and general supportive counseling can be very helpful. This is also a valuable time to teach adolescents about self-care and responsibility for their own health.
Patient Education
Acne is controlled (not cured) with medications. The patient will need to continue to use treatments to prevent new lesions even after the current lesions have resolved. Treatments are designed to prevent new lesions far more than clearing existing lesions. Thus, topical treatments should be applied all over the affected area, not just on the lesions themselves. Some patients notice an initial worsening with treatment before it improves. They need to be warned of this, so they do not stop medications prematurely.
Follow-Up
Expect 4 to 8 weeks to see significant improvement with most treatments. Recommend follow-up about every 6 weeks until the optimal regimen has been determined, then every 2 to 3 months for maintenance and adjustments.
Results
Most acne can be well controlled with some combination of medications as listed above. It may take time to determine the ideal regimen, but patients should be reassured that there are extremely effective treatments to control this condition. Nevertheless, optimal treatment may never make the skin look “completely normal.”
Complications
Complications include scarring from deep lesions or from self-inflicted picking at lesions.
SPECIAL CONSIDERATIONS
Isotretinoin can be tremendously effective in cases of severe, recalcitrant, nodulocystic acne. This agent is also highly teratogenic, and has numerous side effects, including myalgias, arthralgias, epistaxis, xerosis, liver function elevation, hyperlipidemia, and leukopenia. Frequent monitoring of bloodwork is advised. In order to obtain isotretinoin, the prescriber, pharmacy, and patient must receive specific information through an FDA risk management program called iPLEDGE and become registered (www.ipledgeprogram.com). The numerous administrative burdens and potential complications with this medicine have led many family physicians to stop prescribing this medicine and refer these patients to a dermatologist.
REFERENCES
1. Strauss J, Kowchuk D. Guidelines of care for acne vulgaris management. J Am Acad Dermatol 2007;56:651–663.
2. Dawson A, Dellavale R. Acne vulgaris. BMJ 2013;346:f2634.
3. Williams H, Dellavalle R, Garner S. Acne vulgaris. Lancet 2012;379:361–372.
4. Titus S, Hodge J. Diagnosis and treatment of acne. Am Fam Physician 2012;86(8):734–740.
5. Olutunmbi Y, Paley K, English J. Adolescent female acne: etiology and management. J Pediatr Adolesc Gynecol 2008;21:171–176.
| Rhonda A. Sparks, Kalyanakrishnan Ramakrishnan, Brian R. Coleman |
Dermatologic problems are commonly encountered in the primary care setting. This chapter reviews the diagnosis and management of seven of the most common dermatoses encountered in clinical practice.
PSORIASIS
General Principles
Definition
Psoriasis is a life-long papulosquamous dermatologic disorder that is transmitted genetically and characterized by chronic recurrent bouts of characteristic erythematous papules and scaling plaques.
Anatomy
Psoriasis can develop at sites of trauma (the so-called Koebner phenomenon) although it can affect any cutaneous surface. Areas that are common for psoriatic involvement include elbows, knees, scalp, gluteal cleft, and nails. In children under age 2, it may present as a diaper rash.1(pp264–334)
Epidemiology
Psoriasis affects between 1% and 3% of the population. It is found equally in men and women, and usually presents in the second or third decade of life, but may be seen initially in infants and elderly people. Psoriasis is much less common in African Americans, Native Americans, and Asians than in whites. Patients with psoriasis are at an increased risk for atherosclerotic cardiovascular disease and metabolic syndrome.2
Classification
Several forms of psoriasis are defined by morphology and area of cutaneous involvement.
• Chronic plaque psoriasis is the most common morphologic presentation typically involving the elbows, knees, and sometimes the scalp.
• Guttate psoriasis (multiple, small, droplike) usually develops prior to age 20, and is usually preceded by a streptococcal or viral upper respiratory tract infection.
• Generalized pustular psoriasis is a rare, serious, and sometimes fatal variant. Patients develop fever, malaise, diarrhea, and leukocytosis. This form of psoriasis may be precipitated by withdrawal from systemic steroids.
• Erythrodermic psoriasis is another rare and potentially fatal form of psoriasis, occurring in patients with previously stable, chronic psoriasis. Light-sensitive psoriasis is usually precipitated by solar exposure (in some patients hypersensitive to ultraviolet light).
• Psoriasis of the scalp presents with characteristic plaques and is more difficult to treat as plaques are anchored to the scalp by hair.
• Psoriasis of the palms and soles may be a distinct entity marked by exclusive involvement of the palms and soles or involvement (though uncommon) as part of a generalized eruption.
• Pustular psoriasis of the palms and soles cause deep pustules of the central palm and central sole of the foot.
• Keratoderma blennorrhagicum is a form of psoriasis that develops in patients with Reiter syndrome.
• Psoriasis inversus affects less common areas, including the axillae, groin, sub-mammary folds, and other intertriginous areas.
• HIV-induced psoriasis may have an atypical clinical presentation, and an unusually severe course.1(pp267–275)
Pathophysiology
Typical psoriatic plaques show characteristic changes, including hyperproliferation of epidermal keratinocytes and hyperkeratosis, and infiltration of immunocytes along with angiogenesis, with resultant thickening and scaling of the erythematous skin. Mitotic activity of keratinocytes is greatly increased.
Etiology
A genetic predisposition to psoriasis is postulated, although the exact pattern of inheritance is unclear. It appears that genetic predilection in combination with environmental factors precipitates the disease. Symptoms of psoriasis usually improve during summer, which may reflect the presumed positive effect of sunlight. Of patients with childhood psoriasis, 71% have a positive family history.3
Diagnosis
Clinical Presentation
Characteristic dermatologic lesions of psoriasis are red, scaling papules that coalesce into larger plaques. The classic scale of psoriasis is silvery white. There may be small, pinpoint areas of bleeding known as Auspitz sign. The plaques of psoriasis may become thick, especially on the scalp. Psoriasis without scaling is most common in the intertriginous areas, where it can appear as smooth, red, or macerated plaques. Psoriasis affects the extensor surfaces more commonly than the flexures and, in its most common form, spares the palm, soles, and face. Severe psoriasis may be a presenting finding in HIV infection. Psoriatic nail changes and psoriatic arthritis are the most common extracutaneous manifestations of psoriasis, and occur in 5% to 20% of patients with psoriasis.3 Scalp lesions are seen in approximately 50% of patients with psoriasis.
History
Approximately 30% of patients with psoriasis have their first episode before age 20.1(pp264–334) In many cases, the initial presentation is that of guttate psoriasis—psoriatic rash developing after a streptococcal or viral upper respiratory infection. Guttate psoriasis may resolve spontaneously, with recurrence of chronic plaque psoriasis being common. Pruritis is variable. Response to treatment is often temporary. Exacerbations and remissions are usual. Psoriatic arthritis is more common in patients with severe dermatologic disease. Medications may also precipitate or exacerbate the disease. These include lithium, quinidine, clonidine, iodine, indomethacin, some β-blockers, terfenadine, nonsteroidal anti-inflammatory drugs, angiotensin-converting enzyme inhibitors, interferon-α, interleukin-2, isotretinoin, and antimalarial agents.
Physical Examination
Psoriasis most commonly presents with noninflammatory, well-defined, localized plaques involving the extensor surfaces of the elbows, the scalp, the gluteal cleft, and the nails of both the hands and feet. If these occur in intertriginous areas, they may appear inflamed (i.e., bright red and shiny). If a plaque resolves, the skin demonstrates a temporary brown or white macule. The joints may exhibit asymmetric arthritis of one or more joints of the fingers and toes, most often the proximal interphalangeal, distal interphalangeal, metatarsophalangeal, or metacarpophalangeal joints. The joint may be red, warm, painful, and exhibit soft tissue swelling known as “sausage finger.” Range of motion may be decreased. Nail changes, including pitting, yellowing, and severe nail dystrophy, are most commonly seen among patients with joint involvement. Ocular involvement occurs in some patients with psoriatic arthritis. Uveitis, which is the most common manifestation, may present with insidious visual impairment or with acute, painful red eye.
Laboratory Studies
Laboratory tests are of limited value in this disease. If guttate psoriasis is suspected, throat cultures may be obtained to rule out streptococcal infection. There is a high incidence of positive, antistreptolysin O (ASO) titers in this group.1(pp264–334) If psoriatic arthritis is suspected, other rheumatologic causes of arthritis should be ruled out. Rheumatoid factor levels are usually normal, although a small percentage of patients with psoriatic arthritis will have mild elevations.1(pp264–334) Erythrocyte sedimentation rate (ESR), white blood cell counts, and uric acid levels may show mild elevation but have limited predictive value in the diagnosis of psoriatic arthritis.
Imaging
The most severe form of psoriatic arthritis is arthritis mutilans, which classically presents with marked deformity and destruction of the digits on radiograph.
Monitoring
The ESR is the best laboratory test to monitor disease activity.
Surgical Diagnostic Procedures
In rare instances, when the diagnosis is not apparent on clinical presentation, punch biopsy of skin lesions may be diagnostic.
Classification
Diagnostic classification is based on morphology and location of psoriatic lesions (see above). For treatment options, patients are classified according to percentage of body surface affected by psoriasis. Patients with less than 20% of body surface involvement can be managed with topical therapy. Patients with greater cutaneous involvement require more aggressive therapy.
Differential Diagnosis
Seborrheic dermatitis (SD) is commonly confused with psoriasis. Chronic eczema with lichenification may present with thickened plaques, and should be included in the differential diagnosis. Other considerations include superficial fungal infections, lichen planus, pityriasis rosea, squamous cell carcinoma, and cutaneous T-cell lymphoma.
Treatment
Behavioral
A positive correlation between the severity of psoriatic symptoms and psychologic stress has been demonstrated. Stress reduction techniques are therefore useful in some patients.
Medications
Treatment occurs via four basic modalities: topical applications, phototherapy, systemic treatments, and immunobiologics. Other experimental approaches will also be briefly discussed. Disease control, including decreasing frequency of exacerbations, should be the goal of therapy. The mainstay of treatment in mild and localized psoriasis (75% of patients) is topical therapy, with or without phototherapy.4 The second group (25%) with moderate to severe psoriasis is usually treated with systemic treatment. Most common topical treatments include emollients, topical corticosteroids, vitamin D analogs (calcipotriene), vitamin A analog (tazarotene), anthralin, and tars. Topical steroids provide rapid response and control itching and inflammation. Disadvantages include tolerance and skin atrophy. Efficacy may be increased by using occlusive dressings. Calcipotriene produces long remissions but may cause severe irritation and burning. Tazarotene (a retinoid) can also be very irritating to the skin. Efficacy of these medications may be enhanced, and irritation decreased, by concomitant topical steroid use. Anthralin can be used in short bursts, and is effective for scalp psoriasis. It is most effective on chronic, noninflamed plaques, and when used with ultraviolet light (UVB) therapy. Tar solutions are effective in only a small percentage of patients and are best combined with UVB light.4 Regimens including ultraviolet therapy require major commitment of time and money, making them less accessible.
Therapeutic options for severe psoriasis (involving greater than 20% of the cutaneous surface) include ultraviolet light (UVB), the use of psoralens, along with exposure to long-wave ultraviolet light (PUVA). PUVA therapy is effective for symptomatic control of severe and disabling plaque psoriasis, but requires significant time commitment, and is not effective for scalp lesions. Because of concerns with long-term exposure and toxicity, PUVA is most appropriate for patients older than 50 years. Other treatment options for severe psoriasis include methotrexate, acitretin, and cyclosporin. Methotrexate and cyclosporin are effective in psoriatic arthritis but are of limited value secondary to hepatotoxicity and nephrotoxicity, respectively.1(pp264–334) Combining PUVA with UVB, calcipotriene, tazarotene, acitretin, or methotrexate improves efficacy, and decreases cost and adverse effects of treatment. Frequent monitoring of renal, hepatic, and hematologic function is required with several of these agents.
Recent advances in psoriasis research have provided biologic agents that target key mechanisms in the pathogenesis of psoriasis. TNT-α inhibitors are the most commonly prescribed biologic agents and include adalimumab and atanercept.1(pp264–334)
Referrals
Treatment of severe psoriasis and frequent exacerbations and medications used in their management require frequent monitoring, best accomplished through specialized dermatologic care. If psoriatic arthritis is suspected, rheumatologic referral is recommended.
Patient Education
Patients should be informed of the chronic nature of this disease. Environmental factors, medications, and stress exacerbating psoriasis should be avoided.
Follow-Up
Frequent follow-up is important to determine effectiveness of treatment. Some systemic therapeutic agents require special testing to avoid medication side effects.
ACNE ROSACEA
General Principles
Definition
Rosacea is a chronic acneiform dermatologic disorder characterized by erythema, edema, papules and pustules, and telangiectasia, usually affecting middle-aged individuals. It is characterized by periods of remission and exacerbation.5
Anatomy
Rosacea commonly involves the central face, including the nose, forehead, cheeks, and periorbital and eyelid areas. Hyperplasia of the soft tissue of the nose (rhinophyma) may occur in long-standing rosacea.
Epidemiology
Rosacea most commonly occurs between the ages of 30 and 60 years, although it has rarely been reported in younger individuals. It is relatively common among individuals with light hair and eye color, fair skin, and those with a history of blushing or flushing.
Classification
Rosacea disorders are divided into four broad subtypes to guide diagnosis and treatment:
1. Erythematotelangiectatic (vascular) characterized by flushing, telangiectasia, and possibly edema
2. Inflammatory characterized by a spectrum from small papules and pustules to deep nodules
3. Phymatous characterized by marked skin thickening and surface nodularities
4. Ocular characterized by blepharitis and conjunctivitis
Other variants include granulomatous, pyoderma faciale, and perioral dermatitis.6
Pathophysiology
The cardinal features include erythema, edema, papules and pustules, and telangiectasia.3
Etiology
The cause of rosacea is unknown. It is clear that individuals with rosacea have a defective skin barrier and are hyperirritable. Infection with the hair mites Demodex folliculorum has historically been linked to rosacea, but without evidence. One study found an increased frequency of Helicobacter pylori infection, but current literature does not support this to be a causative factor.6
Diagnosis
Clinical Presentation
The earliest manifestations include facial erythema and fine telangiectasia typically involving the cheek. This may progress to a papular or cystic rash involving the cheeks, nose, or forehead. Patients may also present with ocular symptoms.
History
Patients with rosacea usually have a history of recurrent flushing, precipitated by hot or spicy foods, alcohol consumption, temperature changes (including ingested liquids) and extremes, or emotional stimulus. Symptoms may also be brought on or aggravated by sun exposure, but solar skin damage is not a prerequisite for the development of rosacea.5 Later in the disease process, patients may develop hyperplasia of sebaceous glands with accompanying papules, pustules, and nodules resembling acne vulgaris. Ocular symptoms may develop alone or in association with skin lesions, and may include burning, foreign body sensation, meibomian gland dysfunction, blepharitis, conjunctivitis, or episcleritis. Cystic lesions of the nose can occur late in the disease, mostly in middle-aged men.
Physical Examination
Classic skin findings include erythema of the forehead, cheeks, and nose. Close inspection may reveal telangiectasias. These may be accompanied by papules, pustules, nodules, and cysts. Comedones are not characteristic of rosacea. Granuloma formation, characterized by hard papules or nodules, may be severe and most apparent on the nose, representing rhinophyma. Ocular involvement may present with mild conjunctivitis, conjunctival hyperemia, telangiectasia of the lid, blepharitis, and chalazion. The National Rosacea Society Expert Committee recommends the presence of one or more of the following primary features for diagnosis:
• Flushing (transient erythema)
• Nontransient erythema
• Papules and pustules
• Telangiectasia
The following secondary features may appear with primary features:
• Burning or stinging
• Plaque
• Dry appearance
• Edema
• Ocular manifestations
• Peripheral location
• Phymatous changes7
Laboratory Studies
Laboratory studies are not helpful in diagnosis.
Surgical Diagnostic Procedures
Diagnosis of rosacea is clinical. Punch biopsy may be helpful if diagnostic uncertainty is present.
Differential Diagnosis
Differential diagnosis includes acne vulgaris, keratosis pilaris, SD, basal cell carcinoma, systemic lupus erythematosus (SLE), and chronic topical steroid use.6 Rosacea is differentiated from acne vulgaris by the absence of comedones, and from SLE by the presence of papules and pustules. SD usually has prominent scales. Carcinoid syndrome is rare and may cause brief flushing. The cutaneous effects of chronic topical steroids can be indistinguishable from rosacea but resolves with its discontinuation.
Treatment
Behavioral
Control of symptoms is the goal of therapy.
Medications
The three topical medications approved by the Food and Drug Administration for rosacea include topical solutions of metronidazole, several brands of sodium sulfacetamide with sulfur, and azelaic acid gel. Metronidazole, either alone or combined with oral antibiotics, is frequently used for initial therapy to decrease inflammation and erythema. The azelaic acid gel is as effective as metronidazole, although its use is limited by skin irritation. Sodium sulfacetamide is less effective than metronidazole and azelaic acid gel. Topical agents should be used for at least 4 weeks before assessing effectiveness. If symptoms persist after initial topical therapy, tretinoin cream may be useful in papular or pustular lesions, and may be combined with topical antibiotics. Oral antibiotics may be necessary for nodular rosacea or in patients with ocular involvement. Oral antibiotics that have been shown to be effective include tetracycline, metronidazole, erythromycin, and azithromycin. Maintaining remission with topical metronidazole is required after initial therapy. Isotretinoin has been used effectively in the treatment of rosacea, including rhinophyma.8
Surgery
Vascular laser therapy and light therapy may be useful in telangiectasias.
Special Therapy
Minimizing sun exposure is important. Broad-spectrum sunscreen should be applied daily. Some sunscreens can cause irritation and trigger rosacea. Silicon-based preparations are the best. Cosmetic sensitivity is a common feature of rosacea and therefore cosmetic use should be minimized. Astringents and camphor-containing products should also be avoided.
Referrals
Referral to a dermatologist is indicated if response to topical and oral therapy is inadequate. Referral to an ophthalmologist is recommended if ocular rosacea is suspected.
Patient Education
See Special Therapy.
Follow-Up
After initial treatment, follow-up is required in 6 to 8 weeks to determine treatment efficacy.
Complications
Patients with rosacea can develop ocular symptoms that include subnormal tear production, corneal vascularization, and infiltration. Visual acuity may be affected.
ATOPIC DERMATITIS
General Principles
Definition
Atopic dermatitis (AD) is a chronic, inflammatory skin condition commonly seen in people with a personal or family history of allergic rhinitis or asthma. It is commonly referred to as “eczema.” In modern usage, AD and atopic eczema are used interchangeably, and both are acceptable.
Anatomy
AD occurring in infants usually involves the cheeks and spares the perioral and perinasal areas. In childhood (2 to 12 years), it most commonly affects the flexure surfaces including the antecubital fossae, neck, wrists, and ankles. In adults (older than 12 years), AD involves the flexures but also may involve the hands and periorbital area.9
Epidemiology
The prevalence of AD has steadily increased over the past 50 years, and now affects more than 10% of children and 17.8 million people in the United States. More than 60% of patients present before the first year of life. It is rare in adults.10
Classification
Classification is based on age—infant phase (0 to 2 years), childhood phase (2 to 12 years), and adult phase (12 years and older).
Pathophysiology
Two models exist for possible causes of AD. First is thought to be a defect in filaggrin protein, which disrupts the epidermis. This leads to contact between the immune cells and antigens in the external environment. This process effectively modulates an inflammatory response to outside environmental factors.10 The other mechanism thought to cause AD is an impaired epidermal function secondary to abnormalities in the skin.
Etiology
The precise immunologic mechanism involved in the development of AD is unclear. Allergic triggers such as some foods, dust mites, and animal dander have been implicated. AD-associated food allergies are more common in childhood, while airborne allergens are more commonly associated with AD in adults. Other triggers may include temperature change and sweating, excessive washing, contact with irritating substances, and decreased humidity.11
Diagnosis
Clinical Presentation
In infants, typical skin lesions include scaling on erythematous papules involving cheeks. These lesions may also affect the extremities or trunk, sparing the diaper area. In children, intensely pruritic patches more commonly affect the flexure surfaces of the arms and legs. Adults present with a distribution of lesions similar to children but may also have lesions on the hands and eyelids.
History
Patients with AD usually have symptoms from childhood. Many patients with AD also exhibit symptoms of allergic rhinitis and/or asthma. Lesions are intensely pruritic. Patients may have history of recurrent bacterial, fungal, and viral skin infections. Food allergies in children and airborne allergens in adults may trigger AD flares.
Physical Examination
Acute lesions of AD are usually vesicles and may have exudate. More chronic lesions usually demonstrate thickened skin, increased skin markings (lichenification), and excoriated papules and plaques. The flexure areas most commonly involved include antecubital and popliteal fossae, wrists, and forearms. Severe cases may affect any skin surface, although lesions of the axillae, gluteal, or groin area are uncommon. Scratching, leading to destruction of melanocytes, results in areas of hypopigmentation. Associated clinical findings may include severe xerosis, development of ichthyosis, keratosis pilaris, hyperlinear palmar creases, and atopic pleats (appearance of an extra line on the lower eyelid, also known as Dennie–Morgan infraorbital fold).12
Laboratory Studies
Allergy testing may be of benefit to identify triggers causing AD flares.
Surgical Diagnostic Procedures
Punch biopsy may be indicated if clinical diagnosis is unclear.
Differential Diagnosis
Differential diagnosis of AD includes contact dermatitis, SD, drug reactions, psoriasis, and scabies. In infants, the rare disorders Wiskott–Aldrich syndrome and hyperimmunoglobulin E syndrome should be considered.
Treatment
Behavioral
Management of AD requires a comprehensive approach that addresses skin inflammation as well as elimination of exacerbating factors. Contact with wool, excessive heat, and other irritants should be minimized. Airborne allergens and allergenic foods must be identified and avoided. Skin hydration is key and skin must be moisturized by the application of nonirritating, hydrophobic lubricating agents.13
Medications
Acute flares of AD may require potent topical corticosteroid preparations for 7 to 10 days. Tar preparations can help control pruritus and resolve inflammation, decreasing the need for topical corticosteroids. Nonsedating antihistamines may have some anti-inflammatory effects but have not been shown to reduce pruritis significantly. Immunomodulators such as topical calcineurin inhibitors are now considered second-line therapy. The immunomodulators are recommended for short time periods due to potential side effects.13 Oral immunosuppressants such as methotrexate or azathioprine may be considered in severe AD but should be avoided in children. Phototherapy (UVA + UVB) and oral immunosuppressants may be used for severe or resistant AD.13
Referrals
Referral to a dermatologist is appropriate if the diagnosis is uncertain, in patients failing to respond to conventional therapy, or if systemic immunosuppressive agents are considered necessary.
Protocol
Disease management should be considered in three phases: (a) induction of remission, (b) maintenance, and (c) rescue from flares. Induction of remission usually requires steroids while emollients are critical for maintenance therapy. Rescue from flares may involve treatment of secondary infections with oral antibiotics and avoiding exposure to triggers.
Follow-Up
Patients should be followed regularly to assess treatment efficacy.
Complications
Complications of chronic steroid use include skin atrophy, telangiectasia, striae, steroid rosacea, acne, hypopigmentation, and delayed wound healing.13
Special Considerations
Dealing with this chronic disease may result in emotional sequelae, but AD is not an emotional disorder as previously thought.
ALLERGIC AND IRRITANT CONTACT DERMATITIS
General Principles
Definition
Allergic contact dermatitis (ACD) is an inflammatory skin reaction that follows absorption of some antigen applied to the skin and recruitment of previously sensitized antigen-specific T lymphocytes. Irritant contact dermatitis (ICD) is an inflammatory skin reaction that results from direct epidermal damage produced by contact with an irritant and is not immunologic. ICD can affect any person at any time if the irritant and exposure are sufficient, while ACD requires a susceptible individual with prior sensitization by the allergen. Systemic contact dermatitis (SCD) is an inflammatory skin reaction that occurs in a previously sensitized person, following exposure to the allergen by ingestion, inhalation, or injection (e.g., patients allergic to poison ivy may develop a diffuse inflammatory skin reaction following ingestion of raw cashew nuts, which are chemically related to the specific allergen of poison ivy).14,15
Anatomy
Site of exposure of the suspected allergen is usually congruent with the distribution of the rash (under a watchband, elastic waistband, or shoe). Plants usually produce linear lesions at the site of contact. Half of all ACD involves the hands.12 ACD usually affects the dorsum of the hand, where the skin is thinner. ACD secondary to allergens applied to the head will usually involve the hairline or ears, and spares the scalp, where the skin is thick. Airborne allergens, which can be transferred from the hands to the eyes and face, and cosmetics may cause facial involvement. The torso and groin are affected in the area of application of the allergen. Involvement of the oral mucosa is rare, but may occur with dental implants. Genitalia is commonly involved secondary to transfer of the allergens from hands.16
Epidemiology
ICD constitutes 80% of contact dermatitis. Industrial workers are at high risk for occupational skin exposure. The hands are the most commonly affected areas.15
Classification
Contact dermatitis is classified as ICD (irritant), ACD (allergic), or SCD (systemic) (see definition).
Pathophysiology
Unlike most clinical allergic diseases, which involve an immediate hypersensitivity response, ACD is a delayed (cell-mediated) hypersensitivity reaction that depends on previous sensitization in susceptible individuals. ICD results from direct epidermal damage. SCD involves systemic reexposure following previous sensitization to an allergen applied topically.
Etiology
ACD is caused by exposure to common contact allergens, including poison ivy, poison oak, poison sumac, nickel (the most common metal allergen), topical medications (neomycin and bacitracin), latex and rubber chemicals, formaldehyde, and fragrances.17
Diagnosis
Clinical Presentation
ACD presents as an acute pruritic eruption.
History
History should be directed at uncovering contact allergens—specifically work-related exposure, plant exposure, household products, jewelry, clothing, and cosmetics. The timing of an eruption may be as brief as 8 hours (common with plant exposure) and as remote as 1 week after exposure. Pruritus is uniformly present in CD.16
Physical Examination
The acute phase of ACD involves erythema, edema, and vesicles. Vesicles may coalesce to form bullae. Vesicles contain clear fluid and rupture spontaneously during the subacute stage (most common presentation). Vesicles are then replaced by papules, which develop crusting and scaling. Secondary bacterial infection may occur. As the papulovesicular lesions resolve, the chronic stage involving lichenification and scaling occurs.14
Laboratory Studies
Laboratory testing is not routinely recommended; however, patch testing may be used for patients with persistent eruptions and may be helpful to identify allergens.15
Staging
Lesions may present in acute, subacute, or chronic stages (see Physical Examination).
Differential Diagnosis
The differential diagnosis includes AD, SD, nummular eczema, dishydrotic eczema, photocontact dermatitis, psoriasis, T-cell lymphoma, scabies, tinea pedis, and bacterial, fungal, or viral skin infections.
Treatment
Behavioral
Central to ACD prevention and treatment is identifying specific allergens and avoiding contact with them. If the allergen cannot be avoided, wearing a protective barrier is recommended.
Medications
Initial treatment of vesicles and erythema includes cold compresses, which should be used for 15 to 30 minutes initially during the acute stage. Erythema may respond to topical corticosteroids. Hydroxyzine and diphenhydramine control itching. If dermatitis is severe or widespread, involves mucous membranes, or is unresponsive to initial therapy, systemic corticosteroids should be used. ACD due to plant allergens requires 10 to 21 days of treatment with topical or oral corticosteroids to prevent rebound dermatitis.18
Referrals
Referral to a dermatologist is warranted if the diagnosis is unclear or if the patient is unresponsive to conventional therapy.
Patient Education
See Behavioral.
Follow-Up
Patients should be instructed to follow up if rash does not resolve or worsens, as rebound dermatitis is possible and may be more severe than the initial eruption.
Special Considerations
The appearance of new lesions remote from the initial eruption, seen in plant contact dermatitis (Rhus dermatitis), may be confused with active spread of the disease. Contrary to popular belief, vesicle fluid does not contain allergen and cannot spread the inflammation.
SEBORRHEIC DERMATITIS
General Principles
Definition
SD is a chronic, inflammatory papulosquamous skin disease, characterized by erythema and scaling.
Anatomy
The term “seborrhea” suggests the anatomic distribution of this disorder, which is predominant in areas where sebaceous glands are abundant—the scalp, face, upper trunk, and intertriginous areas. Seborrhea also tends to present under areas of facial hair (mustache, beard, eyebrow), and nasolabial folds. In infants, seborrhea commonly affects the scalp and is termed “cradle cap.”19
Epidemiology
In infants, seborrhea usually presents in the first 3 months of life. In adults, seborrhea is most commonly seen between 30 and 60 years of age.
Classification
Seborrhea is classified by age as adolescent and adult SD and infant SD. Infant SD may have a classic scalp distribution, or may be generalized.
Etiology
The etiology of SD is unknown. Malassezia furfur (formerly Pityrosporum ovale) has been implicated, but both genetic and environmental factors seem to influence the onset and course of the disease.1(pp312–315) Other possible stimulants include hormones, nutritional deficiencies, and a neurogenic cause (based on its association with parkinsonism and other neurologic syndromes).20 It also appears to be triggered by stress and is both more prevalent and more intense in patients with the HIV syndrome.19
Diagnosis
Clinical Presentation
Patients with SD typically present with erythema and mild epidermal hyperproliferation leading to scaliness. SD in infants is not usually pruritic, whereas adult SD has varying degrees of pruritus.
History
The onset of seborrhea in infants is usually in the first 3 months of life with scalp involvement. Adults present with an itchy red rash. Patients may have a history of “dandruff” (mild seborrhea), with progression and worsening of symptoms. Symptoms may be worse in winter because of dry indoor environments. Sunlight may cause some patients to flare while promoting improvement in others. SD may have a chronic course in adults, with periods of remissions and exacerbations.
Physical Examination
SD of the scalp presents as mildly greasy scaling and erythema. Blepharoconjunctivitis may coexist. On the chest, SD presents with follicular and para-follicular papules with scales. In infants, SD presents with thick scales and erythema over the vertex of the scalp.20 Application of lotions or oils to the scalp may cause SD to appear intensely erythematous without scaliness.
Laboratory Studies
Fungal cultures and potassium hydroxide (KOH) preparations may be indicated in resistant cases of SD.
Pathologic Findings
Histologically, SD reveals focal parakeratosis, with few neutrophils, moderate acanthosis, spongiosis, and nonspecific inflammation of the dermis. The most characteristic histological finding is neutrophils at the tips of dilated follicular openings.
Differential Diagnosis
SD of the scalp and face should be differentiated from tinea capitis, psoriasis, AD, contact dermatitis, erythrasma, and rosacea.19 SD involving the trunk should be differentiated from pityriasis versicolor and pityriasis rosea. Underlying immunodeficiency should be suspected in generalized SD in infants, especially if associated with diarrhea and weight loss.20 Immunodeficiency should also be suspected in adults who present with severe, recalcitrant cases of SD.
Treatment
Behavioral
Emotional stress has been linked to SD flares.
Medications
Effective treatment options include keratolytics, antifungals, and anti-inflammatory agents. Keratolytics induce sloughing of cornified epithelium. Salicylic acid, zinc pyrithione, and tar shampoos are effective for lesions involving the scalp and face. Treatment of infantile SD requires milder formulations. Shampoos may be used two to three times per week. Anti-inflammatory topical agents and shampoos such as fluocinolone shampoo and cream are also effective, especially in patients with SD involving the scalp. Patients may apply a topical steroid once or twice a day with a shampoo. Topical calcineurin inhibitors (Tacrolimus, Pimecrolimus) have anti-inflammatory and antifungal properties and are recommended for SD over facial skin.20 Most antifungal agents are effective against Malassezia species associated with SD. Ketoconazole and selenium sulfide shampoos are commonly used. Ketoconazole preparations should be avoided in infants.20 Phototherapy utilizing ultraviolet B light is an alternative in patients with extensive SD unresponsive to other measures.19
Special Therapy
Seborrheic blepharitis may respond to cleansing of the eyelashes with baby shampoo and cotton-tipped applicators. The use of ketoconazole in this area is controversial.
Referrals
Referral to dermatology is typically required only in recalcitrant or very severe cases.
Patient Education
Patients should be educated that this is a chronic disorder that may require continued maintenance therapy.
Special Considerations
SD is the most common cutaneous manifestation of AIDS.1(pp312–315) Severe intractable or extensive seborrhea should prompt evaluation for HIV infection. Infants with widespread SD, diarrhea, and inadequate weight gain and physical growth (failure to thrive) should be evaluated for immunodeficiency states.20
PITYRIASIS ROSEA
General Principles
Definition
Pityriasis rosea (PR) is an acute, self-limiting papulosquamous skin eruption, preceded by a viral illness in nearly three-fourths of patients.1(pp316–318)
Anatomy
PR typically involves the trunk and proximal extremities, but in rare cases may involve the arms, legs, and face. A reverse presentation, involving the extremities, is rarely seen.
Epidemiology
The average age of patients affected with PR is 23, with most cases occurring between 10 and 35 years of age. PR occurs most often in the spring and fall.
Classification
The initial phase involves appearance of the “herald patch,” followed 7 to 14 days later by a generalized eruption—the “eruptive phase.”
Etiology
The etiology of PR is unclear, although an infectious agent (Human Herpes Virus 6 and 7) is likely.21 This is supported by the fact that PR occurs in clusters, rarely recurs (2%), and is preceded commonly by a prodromal illness.
Diagnosis
Clinical Presentation
Typical presentation is a prodromal viral illness (headache, malaise, pharyngitis), followed by the herald patch and subsequent smaller salmon-colored lesions during the eruptive phase.
History
Many patients will report an upper respiratory illness a few weeks prior to the rash. The herald patch is typically seen on the torso or proximal arm. Then, 7 to 14 days later, similar smaller oval lesions appear on the trunk and proximal extremities. The majority of patients (over 75%) will also report pruritus. The rash of PR resolves spontaneously in 5 to 8 weeks.22
Physical Examination
The herald patch is a 2- to 10-cm ovoid erythematous, raised patch with a peripheral collarette of fine scales. Subsequent eruption involves similar 5- to 10-mm salmon-colored lesions (hyperpigmented in African Americans) with a characteristic distribution following lines of cleavage (Christmas tree pattern). Lesions may show excoriation.
Laboratory Studies
Physicians may perform KOH testing to rule out tinea. Serologic testing for syphilis is a consideration in appropriate clinical settings.
Pathologic Findings
Histologically, PR demonstrates parakeratosis with or without acanthosis, spongiosis, and a perivascular infiltrate of lymphocytes and histiocytes.
Differential Diagnosis
Psoriasis, secondary syphilis, tinea corporis, Lyme disease, HIV seroconversion illness, and drug eruptions (e.g., hepatitis B vaccine, interferon, captopril, and clonidine) should all be considered.16 Pityriasis Lichenoides Chronica is a variant of PR with similar morphology and distribution but has no herald patch and lasts longer than PR.21
Treatment
Behavioral
Patients should be counseled that PR is a self-limited illness.
Medications
PR, being self-limited, requires only symptomatic treatment in most patients. Oral antihistamines and topical agents (steroids and calamine lotion) may be used for relief of pruritus. Systemic steroids may be used in extensive lesions with severe pruritus, but may lengthen the course of the illness. Some studies show efficacy of antiviral agents (acyclovir, ganciclovir, foscarnet) in hastening resolution of lesions, especially if treated soon after their expression.1(pp316–318)
Special Therapy
PR may be alleviated by UVB phototherapy or natural sunlight exposure if started in the first week of symptoms.
Referrals
Consider referral to dermatology for variable lesion morphology, or if lesions are more extensive or last longer than expected.
Patient Education
Educate patients about etiology (unknown), infectivity (very low), relapse (uncommon), and complications (rare).
Follow-Up
Patients should be instructed to follow up if rash persists longer than 3 months.
Complications
Complications are rare, but postinflammatory hyperpigmentation or hypopigmentation may occur.20 PD during pregnancy may result in miscarriage, preterm labor, and fetal demise; these patients should be counseled and referred for high-risk maternity care.21
REFERENCES
1. Habif TH. Psoriasis and other papulosquamous diseases. In: Habif TP, ed. Clinical dermatology. 5th ed. Philadelphia, PA: Mosby; 2010.
2. Armstrong AM, Harskamp CT, Armstrong EJ. Psoriasis and metabolic syndrome: a systematic review and meta-analysis of observational studies. J Am Acad Dermatol 2013;68(4):654–662.
3. Schon MP, Boehncke W-H. Medical progress: psoriasis. N Engl J Med 2005;18:1899–1912.
4. Levine D, Gottlieb A. Evaluation and management of psoriasis: an internist’s guide. Med Clin North Am 2009;93:108–114.
5. Habif TH. Acne rosacea. In: Habif TH, ed. Clinical dermatology. 5th ed. Philadelphia, PA: Mosby; 2010:256–259.
6. Webster GF. Rosacea. Med Clin North Am 2009;93:1016–1027.
7. Wilkins J, Dahl M, Detmar M, et al. Standard grading system for rosacea: report of the National Rosacea Society Expert Committee on the classification and staging of rosacea. J Am Acad Dermatol 2004;50:907–912.
8. Goldgar C, Keahey D, Houchins J. Treatment options for acne rosacea. Am Fam Physician 2009;80:461–468.
9. Weston WL, Howe W. Epidemiology, clinical manifestations, and diagnosis of atopic dermatitis (eczema). In: Dellavalle RP, ed. UpToDate. Waltham, MA: UpToDate. http://www.uptodate.com/contents/epidemiology-clinical-manifestations-and-diagnosis-of-atopic-dermatitis-eczema Accessed March 31, 2014.
10. Berke R, Singh A, Guralnick M. Atopic dermatitis: an overview. Am Fam Physician 2012;86(1):35–42.
11. Spergel JM. Role of allergy in atopic dermatitis (eczema). In: Sicherer SH, ed. UpToDate. Waltham, MA: UpToDate. http://www.uptodate.com/contents/role-of-allergy-in-atopic-dermatitis-eczema?source=search_result&search=Role+of+allergy+in+atopic+dermatitis+%28eczema&selectedTitle=1%7E150. Accessed March 31, 2014.
12. Habif TH. Atopic dermatitis. In: Habif TH, ed. Clinical dermatology. 5th ed. Philadelphia, PA: Mosby; 2010:154–180.
13. Weston WL, Howe W. Treatment of atopic dermatitis (eczema). In: Dellavalle RP, ed. UpToDate. Waltham, MA: UpToDate. http://www.uptodate.com/contents/treatment-of-atopic-dermatitis-eczema?source=search_result&search=Treatment+of+atopic+dermatitis+%28eczema%29.&selectedTitle=1%7E150. Accessed March 31, 2014.
14. Habif TH. Contact dermatitis and patch testing. In: Habif TH, ed. Clinical dermatology. 5th ed. Philadelphia, PA: Mosby; 2010:130–153.
15. Usatine RP, Riojas M. Diagnosis and management of contact dermatitis. Am Fam Physician 2010;82(3):249–255.
16. Yiannias J. Clinical features and diagnosis of allergic contact dermatitis. In: Fowler J, ed. UpToDate. Waltham, MA: UpToDate. http://www.uptodate.com/contents/clinical-features-and-diagnosis-of-allergic-contact-dermatitis?source=search_result&search=Clinical+features+and+diagnosis+of+allergic+contact+dermatitis&selectedTitle=1%7E136. Accessed March 31, 2014.
17. Goldner R, Tuchinda P. Irritant contact dermatitis in adults. In: Fowler J, ed. UpToDate. Waltham, MA: UpToDate. http://www.uptodate.com/contents/irritant-contact-dermatitis-in-adults?source=search_result&search=Irritant+contact+dermatitis+in+adults&selectedTitle=1%7E33. Accessed March 31, 2014.
18. Brod B. Management of allergic contact dermatitis. In: Fowler J, ed. UpToDate. Waltham, MA: UpToDate. http://www.uptodate.com/contents/management-of-allergic-contact-dermatitis?source=search_result&search=Management+of+allergic+contact+dermatitis.&selectedTitle=1%7E136. Accessed March 31, 2014.
19. Naldi L, Rebora A. Seborrheic dermatitis. N Engl J Med 2009;360:387–396.
20. Schwartz RA, Janusz CA, Janniger CK. Seborrheic dermatitis: an overview. Am Fam Physician 2006;74:125–130.
21. Browning JC. An update on pityriasis rosea and other similar childhood exanthems. Curr Opin Pediatr 2009;21:481–485.
22. Stulberg DL, Wolfrey J. Pityriasis rosea. Am Fam Physician 2004;69:87–91.
|
GENERAL PRINCIPLES
Definitions
• Urticaria is a common and reversible skin eruption characterized by multiple, palpable, circumscribed, erythematous, blanchable, pruritic papules (wheals) and plaques ranging in size from 2 mm to 30 cm.
• Angioedema occurs abruptly on the skin and mucous membranes, may or may not be erythematous, is seldom pruritic but may be painful.
• They are classified by their time course as acute or chronic (lasting more than 6 weeks) and by the presumed inciting agent or mechanism.
Pathophysiology
• Urticaria involves the superficial dermis.
• Angioedema involves the deep dermis and subcutaneous tissue.
• They result from vasodilation and increased vascular permeability caused by the release of mast cell mediators of inflammation, such as histamine and other vasoactive substances.
• Mechanisms are autoimmune, immune complement, and nonimmune mediated.
Epidemiology
• Acute urticaria affects up to 20% of individuals at some point during their life. Chronic urticaria has a prevalence of less than 1%, while angioedema affects about 40% of those with chronic urticaria.1
DIAGNOSIS
Clinical Presentation
• Acute urticaria (urticarial wheals) develop rapidly over 15 minutes and dissipate within 60 minutes to 24 hours. As lesions resolve new crops appear, and the patient may mistakenly report that the individual “hives” have been present for days or weeks.
• Physical urticarias are provoked by skin stimulation resulting in mast cell degranulation. Duration is brief, lasting only 30 to 60 minutes.
• Angioedema has indistinct borders, typically involves the mouth, lips, larynx, tongue, the genitalia, and mucosa of the gastrointestinal tract, and lasts 2 to 3 days.
• Angiotensin-converting enzyme (ACE) inhibitor angioedema does not have associated urticaria.
History
• A careful history often identifies the cause.
• Gastrointestinal angioedema causes abdominal pain.
• Oral angioedema may result in airway obstruction.
Physical Examination
• Physical urticarias can be identified by application of the offending agent or force.
• Urticarial vasculitis is an indicator of underlying disease and must be differentiated from the acute and chronic urticarial wheals. Urticarial vasculitis is suggested by the presence of painful wheals lasting more than 24 hours, wheals with underlying purpura, or those with residual hyperpigmentation.
• Angioedema frequently accompanies the urticarial wheals of chronic, cold, or solar urticaria.
Laboratory Studies
• The American Academy of Allergy, Asthma and Immunology recommends against routine diagnostic testing of patients with chronic urticaria.2
• Antithyroid antibodies may be found in chronic urticaria with an associated thyroiditis.
• Complement assays are used to diagnose hereditary angioedema.
• Surgical diagnostic procedures: Suspected urticarial vasculitis merits a biopsy.
Classification
• Allergic urticaria is immunoglobulin E (IgE) mediated (type 1 hypersensitivity).
• Direct contact, ingestion, or inhalation of an allergen causes hives.
• Typical allergens include grasses, pollens, insect toxins, drugs, foods, or simultaneous infections.
• Medications commonly associated with urticaria include penicillin, cephalosporins, sulfonamides, aspirin, nonsteroidal anti-inflammatory drugs, and vaccines.
• Foods frequently linked with transient urticaria are eggs, nuts, shellfish, strawberries, chocolate, and tomatoes.
• Infectious agents include hepatitis and Epstein–Barr virus, bacteria, and intestinal parasites.
• Children with atopic dermatitis are more likely to have urticaria.
• Physical urticarias comprise 20% to 30% of chronic urticarias.
• Dermatographism is the most common physical urticaria.
• Cholinergic urticaria is characterized by small (1 to 3 mm) pruritic papules with blanched centers. Physical exercise, hot showers, fever, and anxiety are antecedent stimuli.
• Uncommon (cold) and rare (solar, localized heat, delayed pressure, vibratory, and aquagenic) causes of urticaria can be identified by application of the offending agent or force.
• Delayed-pressure urticaria has a 4- to 6-hour lag time between the stimulus and the appearance of a wheal, which may last several hours.
• Chemical or contact urticarias do not involve IgE release.
• Drugs can cause the direct release of histamine in susceptible individuals: aspirin, amphotericin B, dextromethorphan, opiates, buproprion, selective serotonin-reuptake inhibitors (SSRIs), polymyxin B, scopolamine, and radiographic contrast-containing iodine.
• Nonimmunologic urticaria does not require prior exposure to the offending agent. It has a gradual onset over hours and makes up 90% of drug-associated urticaria.
• Certain foods, including spoiled mackerel and tuna, may cause urticaria because of their high histamine content (scombroid poisoning).
• Chronic urticaria is often attributed to an autoimmune etiology, but this remains unproven.
• Focal infections, candidiasis, and undiagnosed malignancy are rarely, if ever, the causes of chronic urticaria.
• Angioedema is most commonly an adverse reaction to drug therapy.
• ACE inhibitors cause angioedema without hives (Kinin pathway). One half of patients present during the first week on the medication.
• Hereditary autosomal dominant angioedema is rare (less than 0.4%). Penetrance is variable, and acquired cases occur, so that a family history may not be helpful. If the fourth component of complement (C4) is low, then the diagnosis should be confirmed with an assay of C1 esterase inhibitor, which is also low.
Differential Diagnosis
• Erythema multiforme (EM) may be confused with large urticarial wheals. EM has an acute onset and typically evolving target lesions that last at least 7 days and fade by 4 weeks.
• Insect bites may occasionally resemble urticaria. The patient’s history and location of the lesions will help clarify the etiology.
• Mastocytosis (urticaria pigmentosa, solitary mastocytoma, systemic disease, and mastocytosis with associated hematologic disorders) is characterized by histamine and other vasoactive substances released from overabundant mast cells. Urticaria and flushing are common symptoms.
• Dermatitis herpetiformis and bullous pemphigoid can occasionally resemble urticaria. They are longer lasting.
• Pruritic urticarial papules and plaques of pregnancy is a fixed rash.
• Angioedema could be confused with facial cellulitis or the edema of superior vena cava syndrome.
TREATMENT
• A thorough history coupled with knowledge of frequently-implicated triggers can help prevent further attacks.
• Local therapies such as topical anti-pruritics, doxepin cream, and 1% menthol in aqueous cream are not very effective.3
• Antihistamine therapy with H1 receptor blockers is more effective for acute urticarias. Regular dosing around the clock offers better control. Nonsedating antihistamines are first-line therapy.3 Desloratadine and levocetirizine at up to four times normal dosing are effective in children and non-pregnant adults.4,5 Loratadine is pregnancy category B at standard doses. Drug interactions should be considered at higher dosages.
• Older antihistamines are effective but not well tolerated at higher doses except at bedtime. They should be avoided in children less than 2 years of age.
• Histamine H2 blockers have been used in conjunction with H1 blockers, but there is insufficient evidence as to their effectiveness.6
• Leukotriene antagonists can be added for symptoms persisting beyond 6 weeks.5
• Corticosteroids given orally for 3 to 7 days can be used as a third-line agent.
• Severe orfractory chronic urticaria must be individualized and may ultimately necessitate immunosuppressive therapy with corticosteroids, cyclosporine, methotrexate, or tacrolimus. There is less evidence to support intravenous immunoglobulins, azathioprine, mycophenolate mofetil, cyclophosphamide, and anti-IgE. Evaluation and treatment are usually coordinated by dermatologists and allergists.
• Patients should be advised to avoid aspirin, other nonsteroidal anti-inflammatory agents, and opioid narcotics.
• Angioedema patients may require intubation. Epinephrine, first-generation antihistamines, and corticosteroids are used.
REFERENCES
1. Sánchez-Borges M, Asero R, Ansotequi IJ, et al. Diagnosis and treatment of urticaria and angioedema: a worldwide perspective. World Allergy Organ J 2012;11:125–147.
2. American Academy of Allergy, Asthma & Immunology. Choosing Wisely. http://www.choosingwisely.org/doctor-patient-lists/american-academy-of-allergy-asthma-immunology/. Accessed March 15, 2014.
3. Zuberbier T, Asero R, Bindslev-Jensen C, et al. EAACI/GA2LEN/EDF/WAO Guideline: management of urticaria. Allergy 2009;64:1427–1443.
4. Zuberbier T, Asero R, Bindslev-Jensen C, et al. EAACI/GA2LEN/EDF/WAO Guideline: definition, classification and diagnosis of urticaria. Allergy 2009;64:1417–1426.
5. Kavosh ER, Khan DA. Second-generation H1-antihistamines in chronic urticaria: an evidence-based review. Am J Clin Dermatol 2011;6:361–376.
6. Fedorowicz Z, van Zuuren EJ. Histamine H2-receptor blockers for urticaria. The Cochrane Library http://www.ncbi.nlm.nih.gov/pubmed/22419335. Accessed March 15, 2014.
| Stasis Dermatitis, Venous (Stasis) Ulcers, and Pressure Ulcers |
STASIS DERMATITIS
General
Definition
Stasis dermatitis (SD) is an eczematous skin condition associated with erythema hyperpigmentation, pruritis, erosions, edema, and lipodermatosclerosis.1
Classification
SD is a clinical indicator of chronic venous insufficiency (CVI). CVI is graded by CEAP (Clinical, Etiologic, Anatomic, Pathologic) classification system. The clinical classes are C0: no signs or symptoms of venous disease; C1: telangiectasias; C2: varicose veins; C3: edema; C4: SD changes (pigmentation, eczema, etc.); C5: healed venous stasis ulcer; and C6: active venous stasis ulcer. Etiology is categorized as primary (degeneration of veins and valves), secondary (damage to vein from deep vein thrombosis (DVT) or inflammatory conditions), or congenital. The anatomic classes are superficial or deep. The Pathologic category is divided into reflux or obstruction.2
Pathophysiology
The venous system of the lower extremity is composed of superficial, perforating, and deep veins. All veins have one-way valves that allow one-way flow of blood from the superficial veins to the deep veins. The valves prevent reflux of blood. Dysfunction of the venous system causes pooling of blood. This triggers a cascade of inflammatory changes and capillary damage that develops CVI. Older age, family history of venous insufficiency, standing occupation, injury, and history of phlebitis or clot are recognized risk factors for CVI.3
Diagnosis
History
SD typically has acute, subacute, chronic, and recurrent presentations. Common complaints are skin color changes, edema, itching, and drainage.
Physical Examination
SD is found on the lower extremities. Acute changes include red, itchy plaques that develop abruptly. Subacute and chronic eczematous changes (dry, flaking, peeling, or erythematous skin) may be seen. Hemosiderin deposition results in reddish brown pigmentation and fibrosis of the subcutaneous tissue. Lipodermatosclerosis refers to necrosis of fat with advanced SD that leads to narrowing of legs distally with an “inverted champagne bottle” appearance.4 SD is first diagnosed with a presentation of a stasis ulcer.
Laboratory/Imaging
Venous duplex ultrasonography and ankle/brachial index (ABI) testing commonly may be ordered to rule out other conditions.
Differential Diagnosis
Cellulitis, contact dermatitis, and tinea corporis are common conditions that may mimic SD. The chronic nature of this condition will help in the diagnosis. Venous ulcers often coexist with SD.
Treatment
Behavioral
Treatment of SD requires significant lifestyle changes. Control of the edema associated with SD is essential. Elevation of the legs whenever possible and avoidance of prolonged standing can improve dependent edema. Compression stockings can be used to treat underlying venous insufficiency. Gradient compression stocking provide the greatest pressure (20 to 40 mmHg) around the ankle and gradually decrease proximally. Multilayered compression bandages are more expensive than single-layer bandages, but they provide faster healing. In severe cases, intermittent pneumatic compression pumps may be considered.5
Medications and Immunizations
The acute eczematous changes should be managed with topical steroids and lubricating creams. Oral antibiotics may be required if secondary cellulitis is suspected.
Patient Education
Patients should be educated on importance of regular exercise, avoidance of prolonged periods of sitting or standing, and need for frequent elevation of the legs.
VENOUS (STASIS) ULCER
General
Definition
A venous (stasis) ulcer (VU) is an ulcer commonly located on the lower leg and is associated with CVI.
Epidemiology
Older age, obesity, previous leg injuries, tobacco use, deep venous thrombosis, and phlebitis are risk factors for VU.6,7
Classification
See the CEAP classification above.
Diagnosis
History
Venous ulcers are often chronic and recurrent. Swelling and aching of lower legs are common. Mild trauma may precede VU development.
Physical Examination
Venous ulcers are shallow, painful, irregular shape, below the knee, and commonly on the medial aspect of the leg. VUs are commonly located in the “gaiter area” from mid-calf to the ankle. Dependent edema, varicose veins, purpura, and changes associated with SD may be present. It is important to assess pulses, sensation, and capillary refill time during the clinical examination.
Laboratory/Imaging
Venous ulcers are typically diagnosed clinically. Venous duplex ultrasonography and ABI testing are commonly ordered to rule out other conditions. Nonhealing ulcers may require tissue culture or biopsy if not responding to therapy.
Differential Diagnosis
Ulcers of the lower leg are typically arterial, venous, diabetic/neuropathic, or pressure related. Ulcers of the lower extremity are often caused by more than one etiology. Arterial ulcers are associated with pain, decreased pulses, and cool extremities. Neuropathic ulcers are often associated with diabetes and loss of sensation in the lower extremities. Pressure ulcers occur over pressure points and are surrounded by a thick callous. Infection, neoplasm, and vasculitis are less common causes of lower extremity ulceration.5
Treatment
Behavioral
Leg elevation and compression therapy is crucial for healing of VU.
Medications and Immunizations
Medium to high potency topical steroids should be used for surrounding eczema/dermatitis. Wet compresses with saline or silver nitrate can aid in the control of the inflammation. Systemic antibiotics should be used only in VUs that have a suspected secondary bacterial infection.
Referral
Vascular or general surgery referral is needed for ulcer debridement if necrosis is present or if the ulcer is not responding to medical therapy. A multidisciplinary team, which includes a dermatologist, vascular surgeon, and wound care expert, may be needed for difficult cases.
Patient Education
Patients should be educated on the importance of regular exercise, avoidance of prolonged periods of sitting or standing, and the need for frequent elevation of the legs.
PRESSURE ULCER
General
Definition
Pressure ulcers (PUs) are localized areas of tissue destruction caused by prolonged pressure usually over a bony prominence. Decubitus ulcers (DUs) are a type of pressure ulcer that occurs in bed-bound patients.
Epidemiology
PUs typically occur in elderly individuals, but can occur in any patient with known risk factors. Immobility, incontinence, poor nutrition, poor circulation, smoking, alcoholism, and diabetes have been found to increase the risk of PU.6 Major contributing factors resulting in DUs are pressure, shear, friction, and moisture.
Classification
PUs are classified using a staging system. They are staged as follows:
• Stage 1: Nonblanchable erythema seen over intact skin
• Stage 2: Ulceration of epidermis, dermis, or both
• Stage 3: Ulceration extending to the subcutaneous layer
• Stage 4: Ulceration extending to muscle, bone, and/or supporting tissues7
Diagnosis
Physical Examination
PUs typically occur over bony prominences such as sacrum, ischial tuberosity, greater trochanter, medial and lateral malleoli, and calcaneous. Callus tissue may surround ulcers due to chronic pressure.
Laboratory/Imaging
PUs are typically diagnosed clinically. Venous duplex ultrasonography and ABI testing are commonly ordered to rule out other conditions. Nonhealing ulcers may require tissue culture or biopsy if not responding to therapy.
Differential Diagnosis
• Venous, arterial, and neuropathic ulcers are at times difficult to differentiate from PU.
• Neoplasm, vasculitis, or infection may present similar to PU.
Treatment
Behavioral
Frequent position changes are a cornerstone of management of PU. Many patients cannot control their immobility or other risk factors. Care takers need to implement positioning and protective care for PU. Good nutrition is also key for adequate protein and other nutrient to ensure healing. A dietician is often incorporated to assist in guiding nutrition therapy plan.
Medication/Immunizations
Topical cleansers and saline wound rinses may be beneficial.
Referral
Assessing and correcting risk factors is the goal of treatment in stage 1 ulcers. Stage 2 ulcers are typically treated using an occlusive dressing and avoiding all pressure to the area. Stage 3 and 4 ulcers are treated based on the degree and severity of the ulcer. Negative pressure therapy (wound vacuum) is a common modality for encouraging wound healing. Presence of necrotic tissue, exudates, or evidence of infection usually requires debridement. This can be performed using enzymatic, mechanical, or surgical techniques. Surgical referral and wound care consult may be necessary for stage 3 and stage 4 ulcers. Complicated reconstruction may be needed for wounds that require significant debridement.8
Prevention
Prevention is the key for high-risk patients. Patients with known risk factors should be identified to allow early initiation of preventive measures. Minimizing pressure with pressure-relieving devices and repositioning schedules as well as maintaining good nutrition and decreasing moisture can help prevent DU.
REFERENCES
1. Habif TP. Stasis dermatitis and venous ulceration: postphlebitic syndromes. In: Habif TP, ed. Clinical dermatology. 5th ed. 2009; Philadelphia, PA: Mosby, Elsevier.
2. Rabe E, Pannier F. Clinical, aetiological, anatomical and pathological classification (CEAP): gold standard and limits. Phelbology 2012;27 (Suppl 1):114–118.
3. Beebe-Dimmer JL, Pfeifer JR, Engle JS, et al. The epidemiology of chronic venous insufficiency and varicose veins. Ann Epidemiol 2005;15:175–184.
4. Kirsner RS, Pardes JB, Eaglestein WH, et al. The clinical spectrum of lipodermatosclerosis. J Am Acad Dermatol 1993;28:623–627.
5. deAraujo T, Valencia I, Federman DG, et al. Managing the patient with venous ulcers. Ann Intern Med 2003;138:326–334.
6. Cakmak S, Gul U. Risk factors for pressure ulcers. Adv Skin Wound Care 2009;22:412–415.
7. Resnick NM. Geriatric medicine. In: Fauci AS, Kasper DL, Longo DL, et al., eds. Principles of internal medicine. New York, NY: McGraw-Hill; 1998:42–43.
8. Levine SM, Sinno S, Levine JP, et al. An evidence-based approach to the surgical management of pressure ulcers. Ann Plast Surg 2012;69(4):482–484.
|
INTRODUCTION
Non-melanoma skin cancers are the most commonly diagnosed cancer in the United States—more than 1 million cases are diagnosed annually. Basal cell carcinoma (BCC) accounts for 80% of cases, and squamous cell carcinoma (SCC) accounts for 20%. Malignant melanoma (MM) was diagnosed in >76,000 people in the United States in 2012 and is an important cause of morbidity and mortality.1 Prevention, early diagnosis, definitive treatment, and surveillance for recurrence are mainstays of treatment for each of these cancers and provide an opportunity for those in primary care settings to improve outcomes. Most definitive treatment is well within the scope of practice for general family medicine and office-based primary care. Familiarity with common presentations, differential diagnosis, risk stratification, and treatment options for BCC, SCC, and MM will be reviewed subsequently. This chapter provides the tools to approach diagnosis and treatment of skin cancer with confidence and evidence-based practice. In the event of diagnostic uncertainty, simple office biopsy can be invaluable for definitive diagnosis and treatment discussions.
Patient education should include methods to reduce the risk of skin cancer. Minimizing cumulative and high-intensity sun exposure is important for skin cancer prevention. Preventive measures include educating patients about use of sunscreen, use of protective clothing, and reduction of exposure to UVA and UVB rays. Following a diagnosis of skin cancer, routine skin examination and skin surveillance is an important step in early identification of subsequent cancers. Risk of UVA and UVB damage is increased in individuals with light skin, eyes, and hair. Fitzpatrick skin type is a continuum of risk graded I to VI with the highest risk individuals (Type I—blue eyes and red hair) burning easily/never tanning, and lowest risk individuals (Type VI—dark eyes and hair) who rarely burn and are deeply pigmented.2,3
BASAL CELL CARCINOMA
General Principles
Definition
BCC is a neoplasm arising from basal keratinocytes of the epidermis and adnexal structures. BCCs cause damage primarily by local growth and destruction; metastasis is very rare. Exposure to UVB light damages the cellular DNA repair system, leading to atypical cells.
Epidemiology
Those at highest risk for BCC are fair skinned, with light hair/eyes and poor tanning ability. The lifetime risk for development of BCC in the Caucasian U.S. population is 30%, and is more common in men than in women. Up to 85% of BCC occur on the head and neck, although not always in areas of maximal sun exposure. Intense UVB light exposure places patients at higher risk than continuous exposure. Transplant patients are at marked increased risk of developing BCC. New BCC is common in the 3 years following an index diagnosis.2,4
Classification
There are five histologic subtypes of BCC and a number of clinical subtypes that vary in presentation and progression. Clinical presentation, cell type, tumor size, and location are important in planning treatment. Histologic types include nodular, superficial, micronodular, infiltrative, and morpheaform; a mixed pattern is one that includes multiple cell types. The three main clinical types are:
• Nodular: This is the most common type of BCC, often described as a pearly white or pink papule that ulcerates. These lesions can remain flat and can appear anywhere on the body. Nodular BCC, which is one of the less aggressive BCC clinical types, can also be pigmented or cystic in appearance.
• Superficial: This is the least aggressive of the BCC clinical subtypes, slow growing, round/oval, or scaling plaque, typically with a characteristic pearly border. The trunk is a common location.
• Sclerosing/morpheaform: Lesions are plaque-like, waxy, and often white to yellow in color, with a subtly-abnormal surface appearance allowing deep growth and extension prior to diagnosis.2,4
Diagnosis
History
Patients often describe a scaling or nonhealing sore, or a bleeding lesion. Typically, lesions are present for an extended period of time prior to presentation.
Physical Examination
BCCs are most easily recognized when they have a pearly border, scaling, and surface ulceration. Telangiectatic vessels are often visible throughout and surrounding the lesion. The vast majority of BCC will be found on the head and neck region and can occur in non-sun-exposed areas as well.
Differential Diagnosis
Depending on the clinical subtype at presentation, BCC can resemble dermal nevi, keratoacanthoma, irritated seborrheic keratosis, psoriasis, molluscum, and sebaceous hyperplasia. Shave, punch, or excisional biopsies are options for definitive diagnosis.2,4
Treatment
Medical/Surgical
In planning definitive treatment of BCC, it is important to consider histology, lesion size, clinical presentation, and location. Treatment options are determined based on level of risk. See Table 16.8-1.
Low-Risk BCC
Low-risk BCCs are clinical subtype nodular or superficial, slow growing, well-defined borders, and small (head <6 mm, neck <10 mm, trunk <20 mm). Treatment options for low-risk BCC are as follows:
• Electrodesiccation and curettage (ED&C): The tissue integrity of a BCC is weak and collapses with curettage in a characteristic way that is palpable at the time of removal. ED&C has a 95% cure rate when used appropriately.
• Excision: Use local anesthesia with sharp elliptical excision of the lesion with 2- to 3-mm margins. If pathology shows tumor extension to the borders of the specimen, re-excision is indicated.
• Radiation: Reserved for special cases for patients who would not tolerate other treatment, such as the elderly.2,4
• Topical treatment: Two topical treatments can be used in the treatment of BCC:
• Imiquimod 5%: An immune modulator that causes a local T-cell-mediated immune response. It is applied five times per week for 6 weeks. Recurrence rate of 20% at 2 years is higher than with surgical interventions. The local skin reaction is generally well tolerated.5
• 5-Fluorouracil 5%: An antimetabolite that incorporates into DNA of rapidly dividing cells and leads to cell death. It is applied twice daily for 12 weeks. Local skin reaction occurs with erythema and flaking.5
High-Risk BCC
Subtypes at higher risk for recurrence and metastasis are sclerosing BCC, morpheaform, basosquamous, or micronodular, or larger lesions as described above. Special consideration must be given to lesions in the area of the nose and eyes because of possible local extension.
Mohs surgery: High-risk histologic subtypes have been associated with up to 7 mm of microscopic extension around the primary tumor. Mohs surgery is a microscopically controlled surgery to treat poorly defined tumors, large tumors, or those in challenging areas such as the nose or eyelid. It is the treatment of choice for sclerosing BCCs.6
SQUAMOUS CELL CARCINOMA
General Principles
Definition
SCC occurs in areas of actinic damage, thermal injury, chronic inflammation, or radiation exposure with potentially aggressive behavior depending on clinical type. SCC has significant metastatic potential. The cells affected are the epithelial keratinocytes.
Epidemiology
Those at highest risk are fair skinned with high cumulative sun exposure. Other indicators of risk include history of sunburns or evidence of sun damage (freckling, telangiectasias, wrinkling), and older age. SCC can arise from actinic keratosis (AK), cutaneous horns, Bowen disease—squamous cell carcinoma in situ (SCCIS), leukoplakia, lichen sclerosis, chronic infection, and thermal burns. SCC occurs in sun-exposed areas of the scalp, back, dorsal aspect of the hands, and pinna. Similar to BCC, transplant patients are at high risk because of immunosuppression.
Malignant potential of SCC is related to size, location, histology, immunologic status, and invasion depth. Lesions that are associated with higher metastatic potential are size >2 cm, depth >4 mm, show poorly differentiated histology, are located on lip/ear/scar, or reveal perineural involvement. Mode of spread of SCC is by direct extension, by lateral extension along tissue planes, by perineural or perivascular routes, and by local metastasis via lymphatics. If SCC has progressed, distant metastasis via hematogenous dissemination to the lungs, liver, brain, skin, and bone is possible.2
Classification
SCC exists as part of a continuum of disease; precursor lesions are listed below in order of progression toward SCC. Progression of disease in dysplasia and SCC itself is defined by increasing depth and invasion of the epidermis.
• AK: Dysplastic change (“atypia”) confined to the epidermis. Progression to SCC occurs in 20% of lesions. Generally AKs are rough, red/brown, and dry in appearance often with silver-white scale. There is a higher likelihood of SCC in thicker, red, painful, ulcerated, growing or large AKs. These are commonly found in elderly patients, and may be isolated or occur as multiple lesions.
• Bowen disease and erythroplasia of Queyrat (SCCIS): These lesions are often slow growing, red, scaly patches that can develop into invasive SCC. Erythroplasia of Queyrat is SCCIS affecting the penis.
• SCC: Proliferating atypical keratinocytes penetrate the epidermal basement membrane into the dermis, resulting in induration and increased potential for local destruction and distant metastasis.2,4
Diagnosis
History
Patients may describe a persistent or growing lesion that has evolved over time and has grown in either size or thickness. Lesions can arise from chronically inflamed or scarred skin.
Physical Examination
SCC often appears flat, scaly, or indurated and is present in sun-exposed areas, often with other signs of sun damage surrounding lesions (except in African Americans in whom SCC commonly occurs in non-sun-exposed areas). Given the mode of extension, evaluation of regional lymph nodes is important.
Differential Diagnosis
Psoriasis, eczema, superficial BCC, seborrheic keratosis, and MM can be diagnosed. Diagnostic or excisional biopsy should be performed for uncertain diagnosis.2
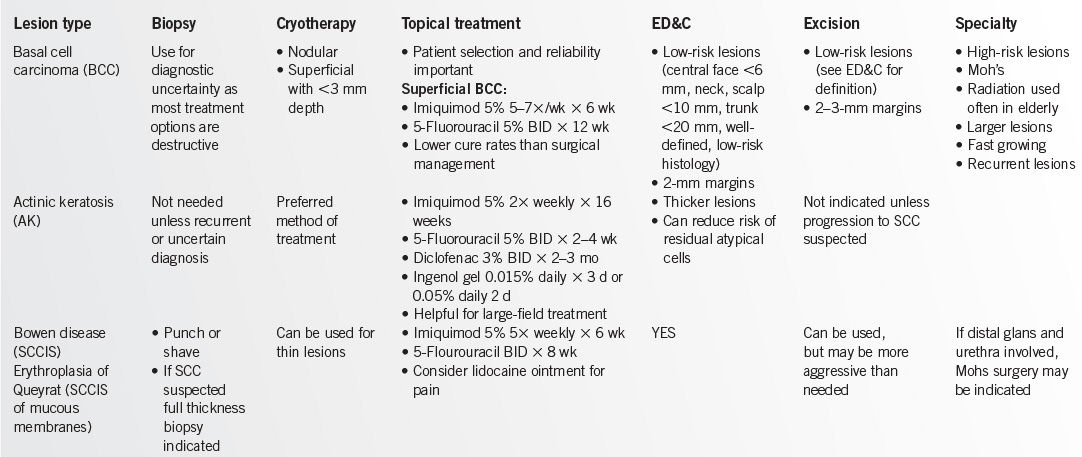
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


