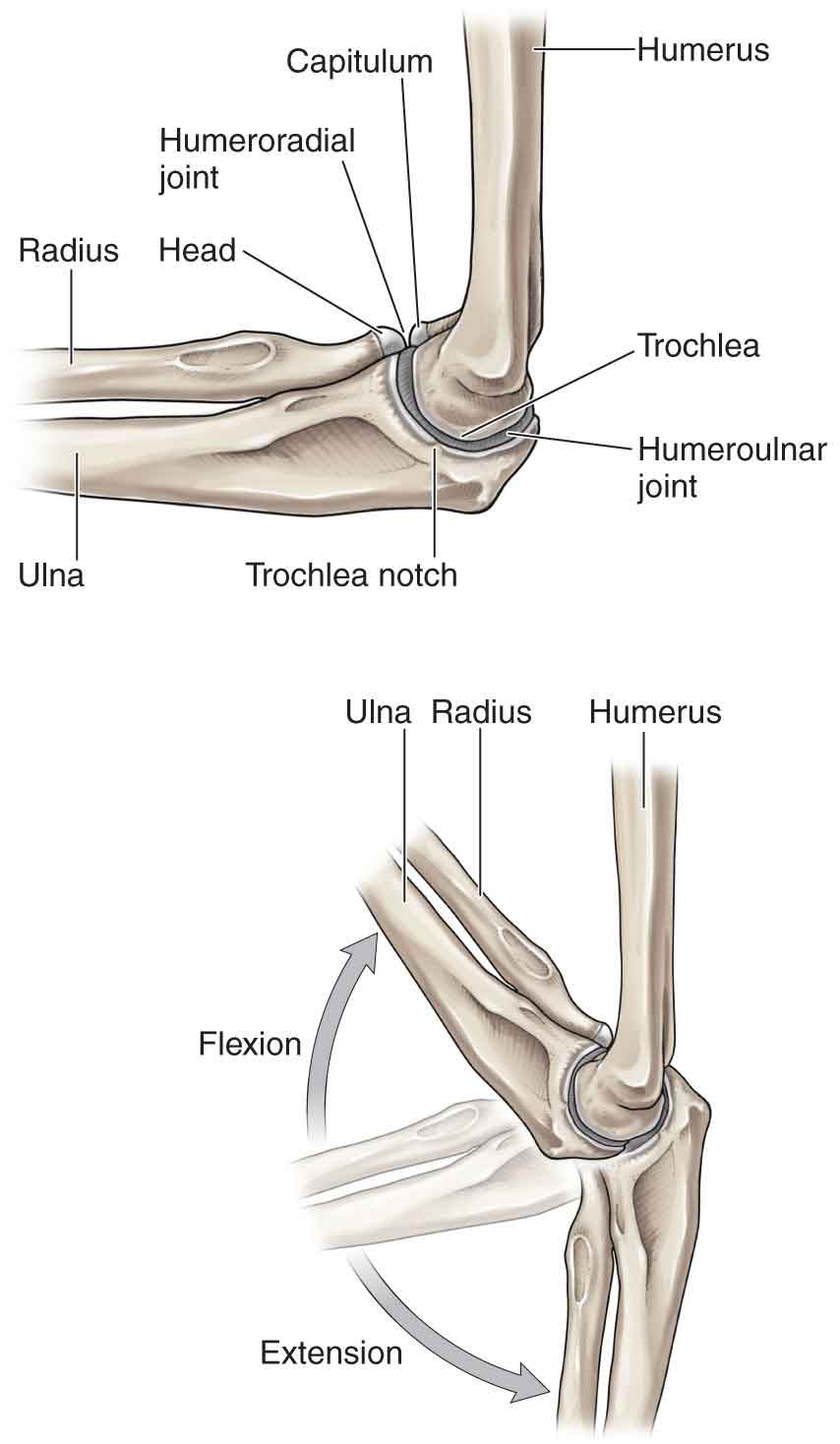
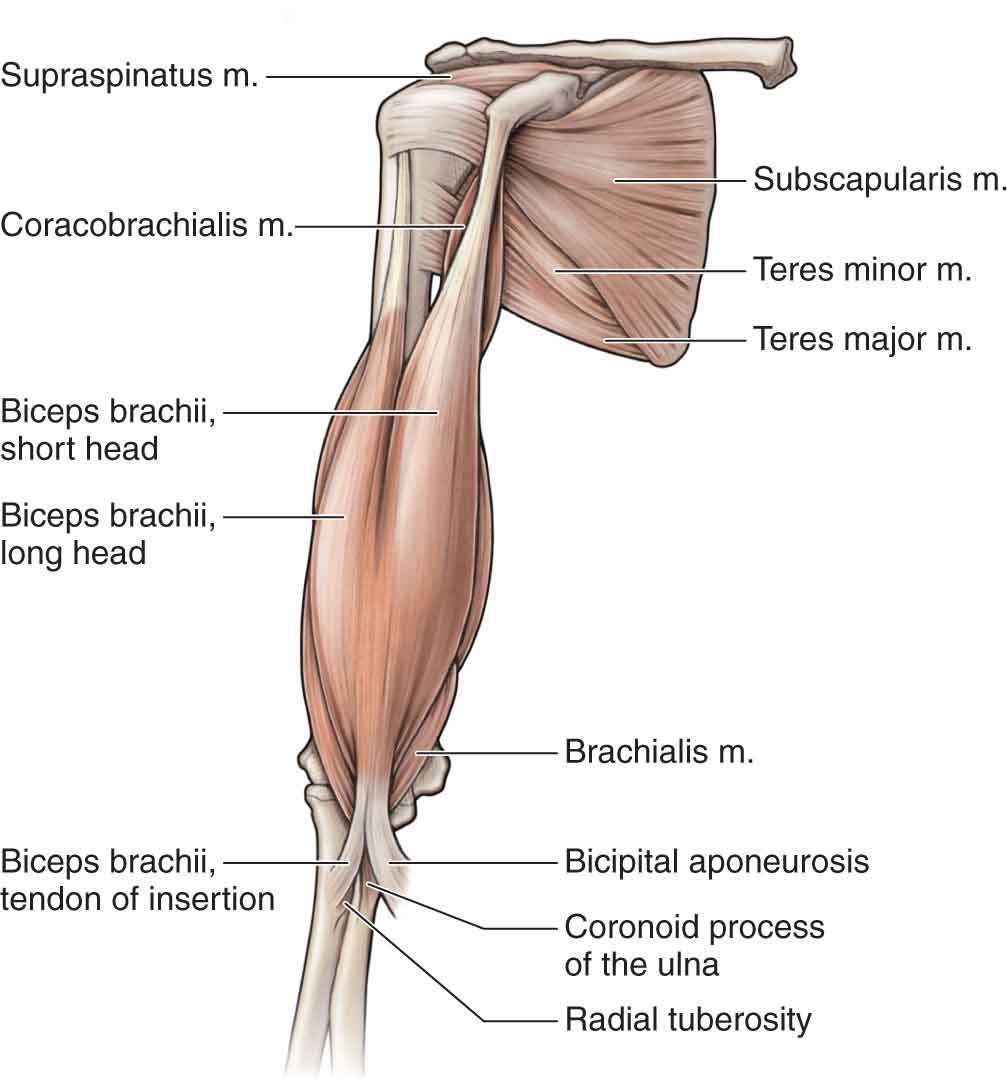
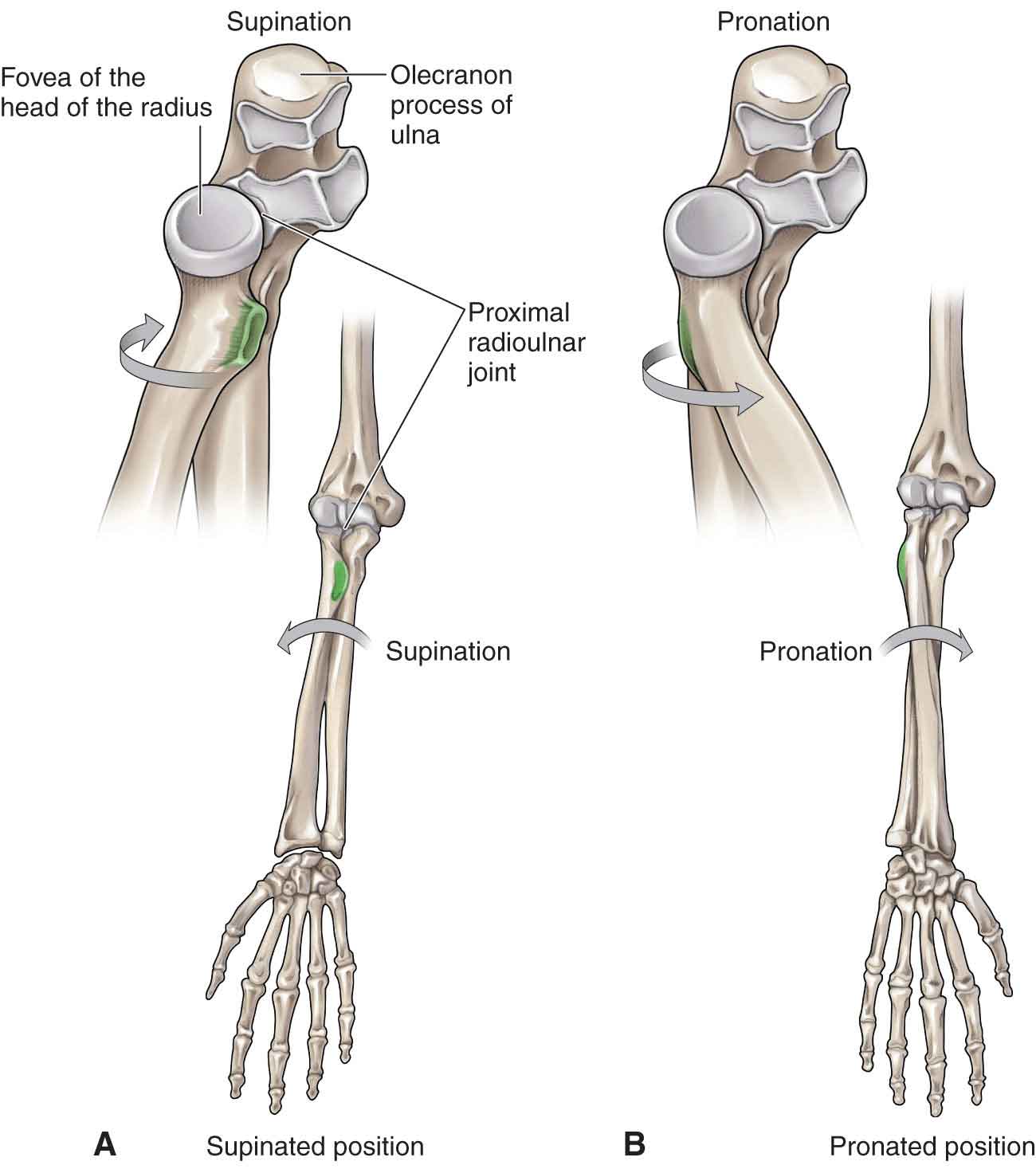
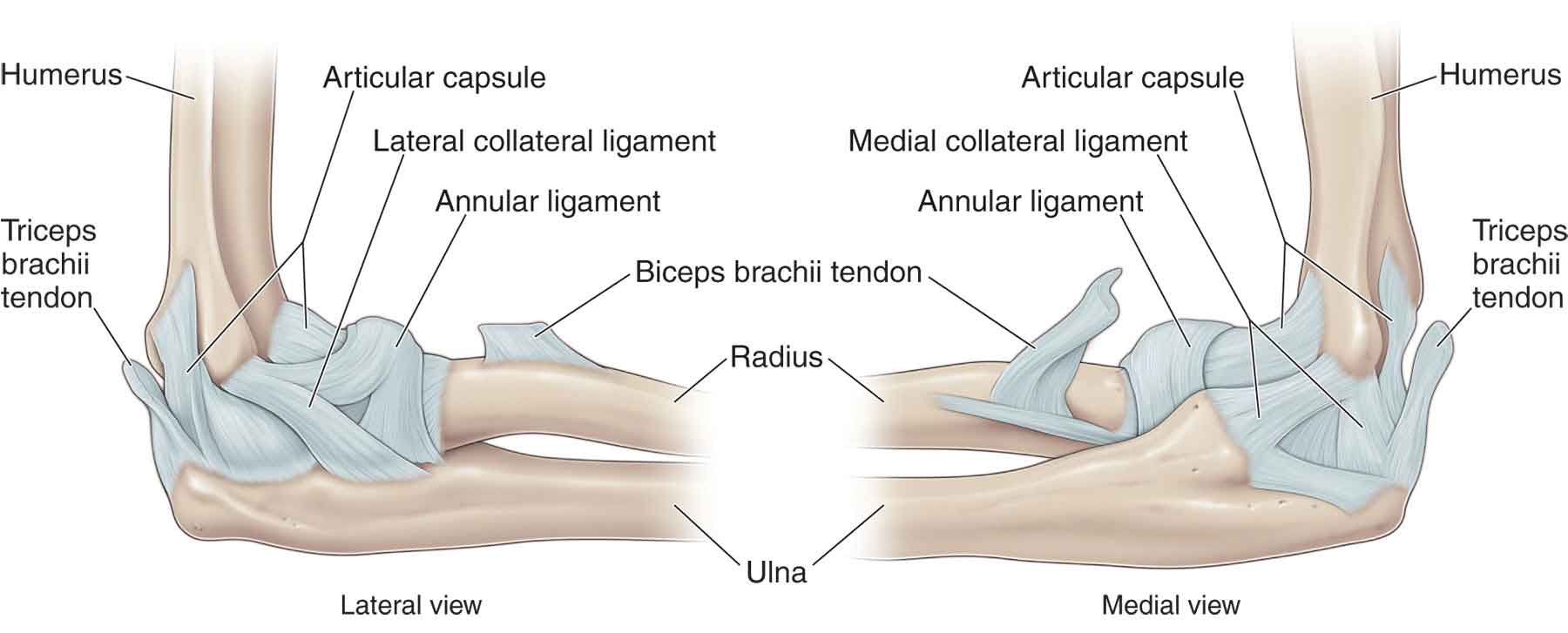
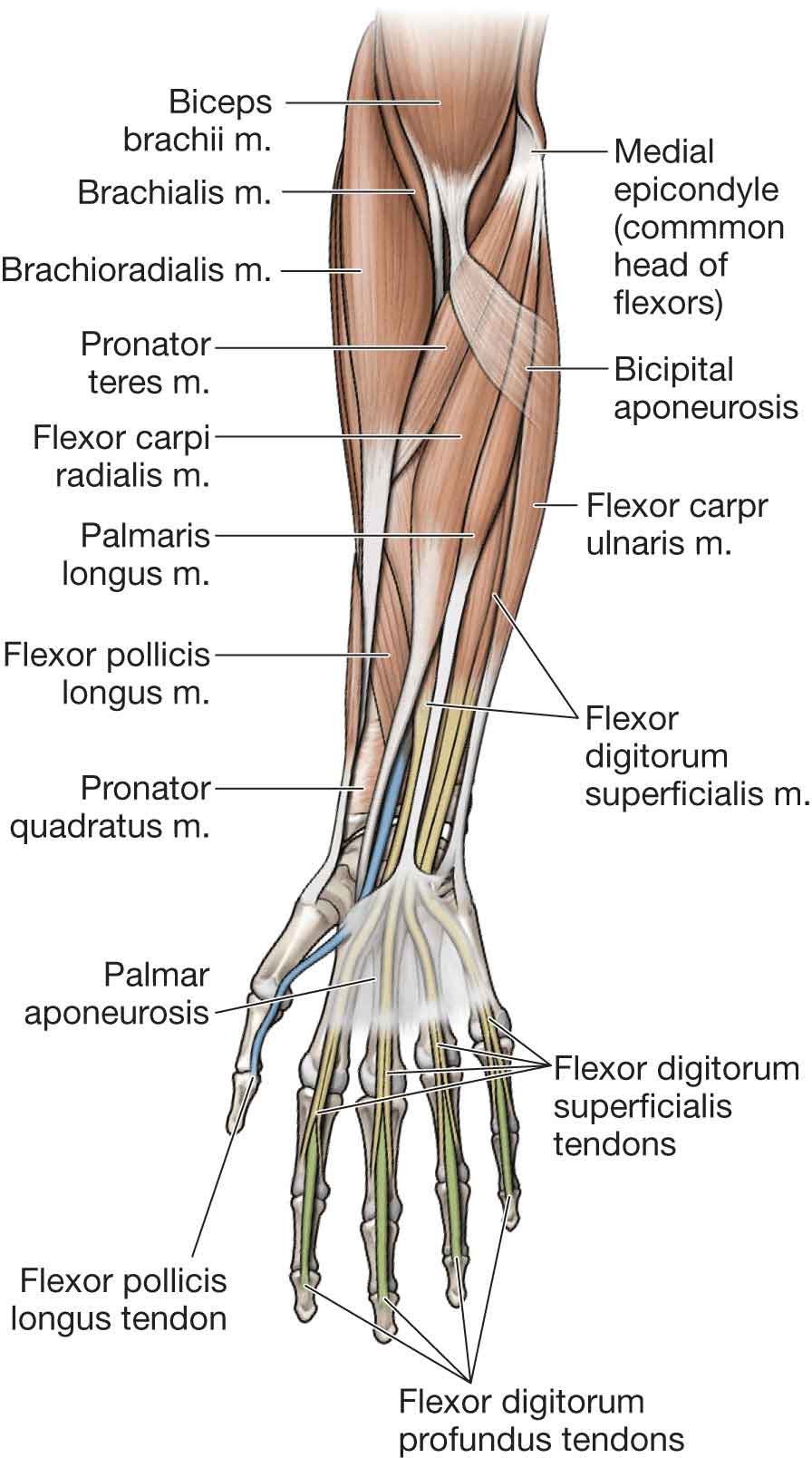
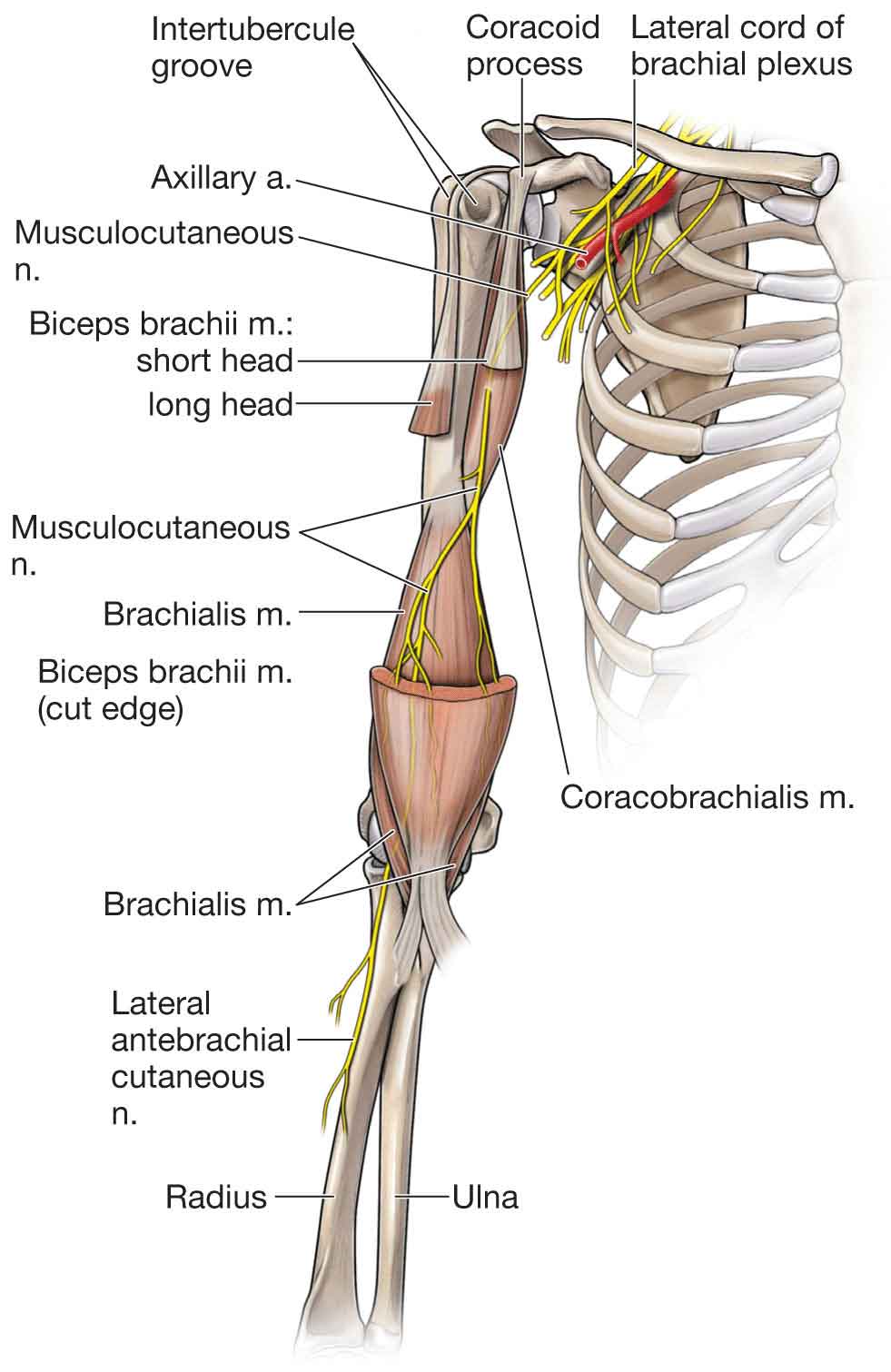
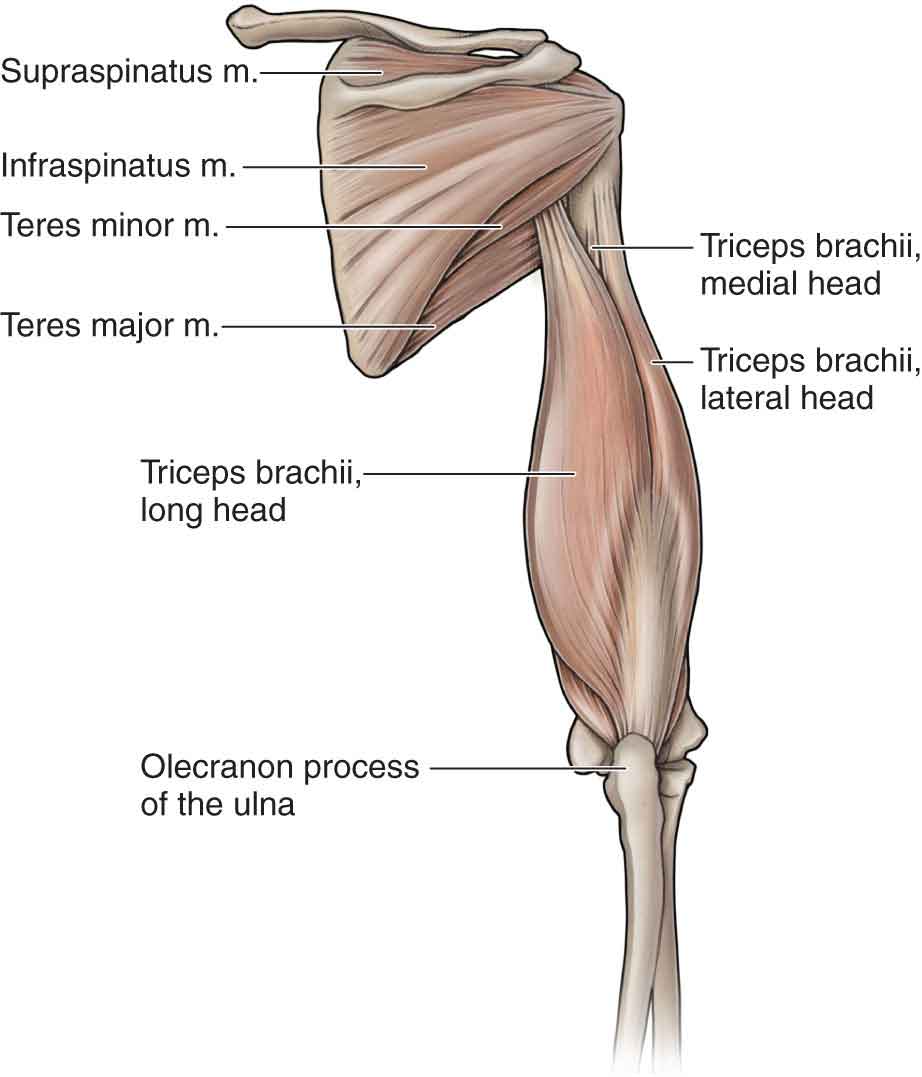
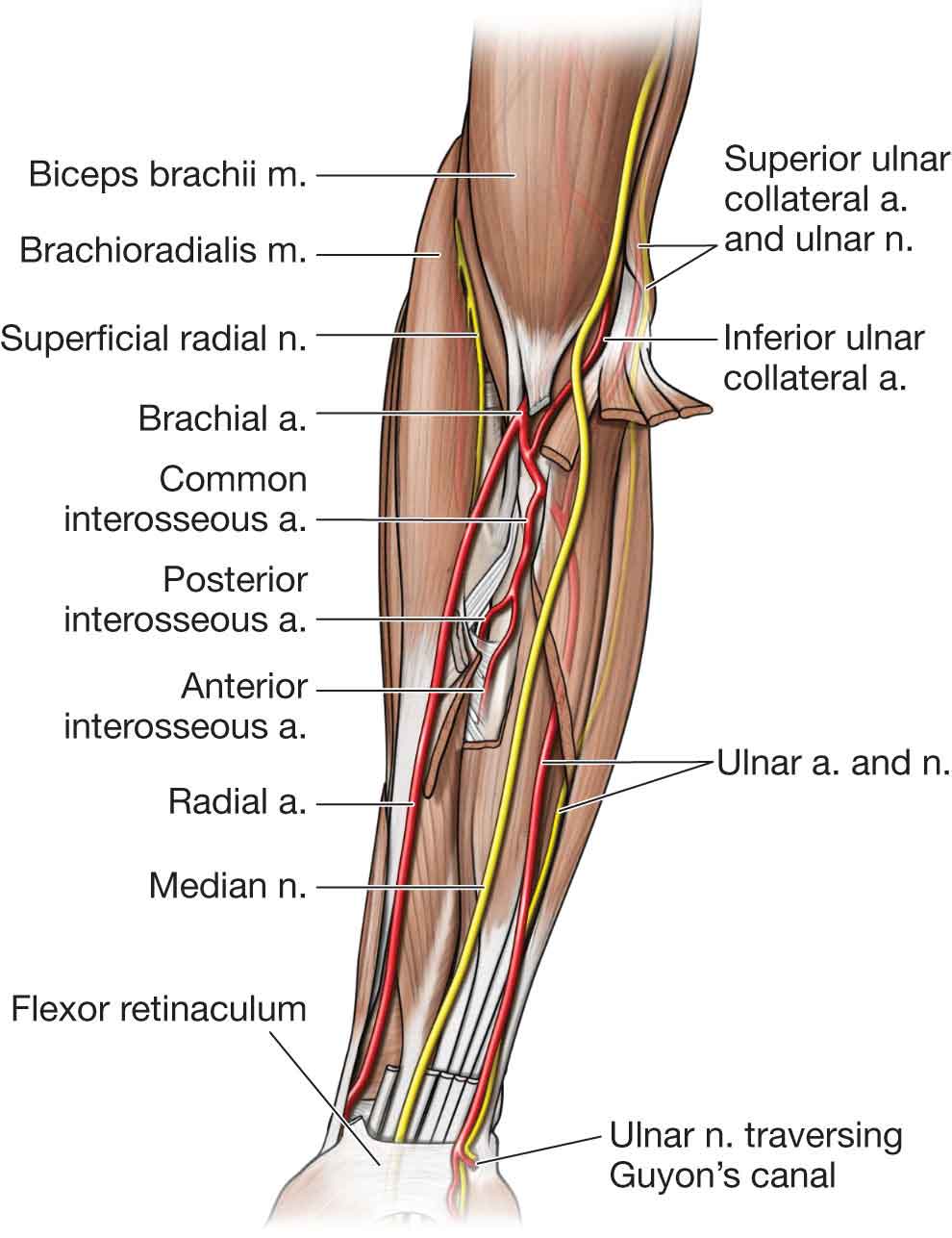
The elbow serves an important linkage function that enables proper positioning of the hand and the transmission of power from the shoulder to the hand, thus augmenting the versatility and agility of the upper extremity. Unlike the shoulder, the elbow complex is an inherently strong and stable joint, because of the interrelationship of its articular surfaces and ligamentous constraints. However, the stability of the elbow complex allows little in the way of compensatory adjustments, making it particularly vulnerable to overuse injury from repetitious muscle activity and sudden movements of acceleration and deceleration. Appropriate diagnosis and treatment require a detailed understanding of the normal anatomy of the elbow. The elbow complex, enclosed within the capsule of the cubital articulation, is composed of three distinct articulations: the humeroulnar joint, the humeroradial joint, and the proximal radioulnar joint. The anterior joint capsule of the elbow originates from the distal humerus proximal to the radial and coronoid fossa, from where it then inserts distally into the rim of the coronoid and the annular ligament (AL).1 Posteriorly, the capsule incorporates the area proximal to the olecranon process; it attaches distally along the articular margin of the sigmoid notch and the proximal aspect of the olecranon fossa.2 The humeroulnar (trochlear) joint is a uniaxial hinge joint formed between the incongruent saddle-shaped joint surfaces of the spool-shaped trochlea of the humerus and the trochlear notch of the proximal ulna (Fig. 17-1). Anteriorly, the humeral trochlear groove is vertical and parallel to the longitudinal groove, while, posteriorly, the groove runs obliquely lateral and distal, forming an acute angle of about 15 degrees with the longitudinal axis of the humerus.7 This valgus angulation is referred to as the “carrying angle” of the elbow. Three hundred degrees of the articular surface of the trochlea is covered with hyaline cartilage, compared with only 180 degrees on the trochlear notch.8 FIGURE 17-1 The bony structures of the elbow complex. (Reproduced, with permission, from Chapter 31. Arm. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy. New York, NY: McGraw-Hill; 2011.) The humeroradial (radiocapitellar) joint is a uniaxial hinge joint formed between the spherical capitellum of the humerus and the concave fovea of the radial head (see Fig. 17-1). The design of this joint allows the elbow to flex and extend and for the radius to rotate. The superior surface of the proximal end of the radius is biconcave while the head of the radius is slightly oval. The radial tuberosity (see Fig. 17-2) serves as a site of attachment for the biceps brachii (see Fig. 17-2). The humerus widens at the elbow and forms the medial and lateral epicondyles. FIGURE 17-2 The biceps. (Reproduced, with permission, from Chapter 31. Arm. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy. New York, NY: McGraw-Hill; 2011.) The radius and the ulna lie side by side, with the radius being the shorter and more lateral of the two forearm bones. The proximal or superior radioulnar joint is a uniaxial pivot joint. It is formed between the periphery of the convex radial head, and the fibrous osseous ring formed by the concave radial notch of the ulna (see Fig. 17-3), which lies distal to the trochlear notch, and the AL. The AL (Fig. 17-4) forms 80% of the articular surface of the proximal radioulnar joint (see AL later). FIGURE 17-3 The proximal radioulnar joint, and the two major movements: (A) supination, and (B) pronation. (Reproduced, with permission, from Chapter 31. Arm. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy. New York, NY: McGraw-Hill; 2011.) FIGURE 17-4 Elbow joint with ligaments detailed. (Reproduced, with permission, from Chapter 31. Arm. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy. New York, NY: McGraw-Hill; 2011.) The proximal and distal radioulnar joints together form a bicondylar joint. An interosseous membrane sometimes referred to as the middle radioulnar articulation and located between the radius and the ulna, serves to help distribute forces throughout the forearm, and provide muscle attachment. Most of the fibers of the interosseous membrane of the forearm are directed away from the radius in an oblique medial and distal direction.8 Approximately 8% of the compression force due to bearing weight to the forearm crosses the wrist between the lateral side of the carpus and the radius.8 The remaining 20% of the compression force passes across the medial side of the carpal bones and the ulna.8 Because of the fiber orientation of the interosseous membrane, some of the proximally directed force through the radius is transferred across the membrane to the ulna.13 Support for the elbow complex is provided through strong ligaments (Fig. 17-4). The ulna collateral ligament (UCL) or medial collateral ligament (MCL) extends from the central two-thirds of the anteroinferior surface of the medial epicondyle to the proximal medial ulna, from just posterior to the axis of the elbow medial epicondyle,14–16 to just distal to the tip of the coronoid (see Fig. 17-4).17,18 The fan-shaped MCL is the most important ligament in the elbow for providing stability against valgus stress, particularly in the range of 20–130 degrees of flexion and extension,19 with the humeroradial joint functioning as a secondary stabilizer to valgus loads.20,21 The MCL achieves this stability through almost the total range of flexion and extension due to its eccentric location with respect to the axis of elbow motion.22–25 In full elbow extension, valgus stability of the elbow is provided equally by the MCL, the joint capsule, and the joint interactions.5 There are three distinct components of the MCL14,17,26,27: the anterior bundle, the transverse bundle, and the posterior bundle (Fig. 17-4). The anterior bundle of the MCL is the strongest and stiffest of the elbow collateral ligaments, with an average load to failure of 260 newtons (N).19 The anterior bundle of the MCL inserts an average of 18 mm distal to the coronoid tip, and is composed of two other components, the anterior band and the posterior band, which perform reciprocal functions:17,22,26 The oblique bundle, also known as Cooper’s ligament, is variably present.14,17,31 It does not cross the elbow joint and comprises fibers running along the medial joint capsule from the tip of the olecranon to the medial ulna, just distal to the coronoid.14,32 The transverse fibers have little role in elbow stability due to the fact that they both originate and insert on the ulna. The posterior bundle of the MCL originates from the medial epicondyle and inserts onto the medial margin of the semi-lunar notch, forming the floor of the cubital tunnel and a thickening of the posterior elbow capsule.32,33 Being thinner and weaker than the anterior bundle, the posterior bundle becomes taut at 60 degrees of elbow flexion but provides only secondary restraint to valgus stress at flexion beyond 90 degrees.22,23 Unlike the medial ligament complex, the lateral ligamentous complex (see Fig. 17-4) is less discrete, and individual variation is common. The lateral complex consists of the AL, the lateral-radial collateral ligament (LCL), and the lateral ulnar collateral ligament (LUCL).19 The LCL courses distally and forms a broad conjoint insertion onto the proximal ulna.34,35 The proximal margin of this conjoined insertion begins at the proximal aspect of the radial head, just inferior to the radial notch. From here, it progresses along a rough ridge in line with the supinator crest of the ulna.19 The LCL is closely associated with the insertions of the extensor carpi radialis brevis (ECRB) and the supinator, with the latter muscle crossing this ligament complex obliquely from distal to proximal at its ulnar attachment and becoming confluent with the underlying AL and LCL more proximally at its humeral origin.19 The LUCL originates from the lateral epicondyle from where it passes over the AL and then begins to blend with it distally where it inserts onto the supinator crest of the ulna.14 It is unclear as to how much stability is provided by the LUCL, but it may help prevent posterolateral rotary instability.36 As a unit, the lateral ligament complex functions to maintain the ulnohumeral and radiohumeral joints in a reduced position when the elbow is loaded in supination. More specifically, the anterior portion of the LCL stabilizes the proximal radioulnar joint during full supination; the posterior portion stabilizes the joint during pronation. As the axis of rotation passes through the origin of the LCL, the various fibers of this ligament maintain consistent patterns of tension whether varus, valgus, or no force is applied to the elbow throughout the arc of flexion.14,28 The LCL contributes only 9% of the restraint to varus stress at 90 degrees of flexion. In extension, the LCL contributes 14% of this restraint.28 Insufficient lateral support of the elbow complex results in lateral gapping at the ulnohumeral joint and posterior translation of the radial head in relation to the capitellum.19 However, the proximal radioulnar relationship remains undisturbed. The AL (Fig. 17-4), which is wider proximally and distally, runs around the radial head from the anterior and the posterior margin of the radial notch, to approximate the radial head to the radial notch and enclose the radial circumference. The AL forms a band that encircles 80% of the radial head and functions to maintain the relationship between the head of the radius and the humerus and ulna. The internal circumference of the AL is lined with cartilage to reduce the friction against the radial head during pronation and supination.8 The external surface of the ligament receives attachments from the elbow capsule, the LCL, and the supinator muscle. The quadrate ligament is a short, stout ligament that arises just below the radial notch of the ulna and attaches to the medial surface of the neck of the radius.8 This ligament lends structural support to the capsule of the proximal radioulnar joint.8 There are numerous bursae in the elbow region.23 The olecranon bursa is the main bursa of the elbow complex and lies posteriorly between the skin and the olecranon process. Under normal conditions, the bursa does not communicate with the elbow joint, although its superficial location puts it at high risk of injury from direct trauma to the elbow. Other bursae in the posterior elbow region include the deep intratendinous bursa and a deep subtendinous bursa, which are present between the triceps tendon and olecranon. Anteriorly, the bicipitoradial bursa separates the biceps tendon from the radial tuberosity. Along the medial and lateral aspects of the elbow are the subcutaneous medial epicondylar bursa and the subcutaneous lateral epicondylar bursa.37 A summary of the muscles of the elbow is outlined in Table 17-1. The muscles of the forearm are contained within three major fascial compartments, the anterior forearm, the posterior forearm, and the compartment referred to as the mobile wad (Table 17-2). TABLE 17-1 Muscles of the Elbow, Forearm, Wrist, and Hand: Their Actions, Nerve Supply, and Nerve Root Derivation Muscles Nerve Supply Nerve Root Derivation Action Triceps Radial C7–8 Elbow extension Anconeus Radial C7–8, (T1) Brachialis Musculocutaneous C5–6, (C7) Elbow Flexion Biceps brachii Musculocutaneous C5–6 Brachioradialis Radial C5–6, (C7) Biceps brachii Musculocutaneous C5–6 Supination of the forearm Supinator Posterior interosseous (radial) C5–6 Pronator quadratus Anterior interosseous (median) C8, T1 Pronation of the forearm Pronator teres Median C6–7 Flexor carpi radialis Median C6–7 Extensor carpi radialis longus Radial C6–7 Extension of the wrist Extensor carpi radialis brevis Posterior interosseous (radial) C7–8 Extensor carpi ulnaris Posterior interosseous (radial) C7–8 Flexor carpi radialis Median C6–7 Flexion of the wrist Flexor carpi ulnaris Ulnar C7–8 Flexor carpi ulnaris Ulnar C7–8 Ulnar deviation of the wrist Extensor carpi ulnaris Posterior interosseous (radial) C7–8 Flexor carpi radialis Median C6–7 Radial deviation of the wrist Extensor carpi radialis longus Radial C6–7 Abductor pollicis longus Posterior interosseous (radial) C7–8 Extensor pollicis brevis Posterior interosseous (radial) C7–8 Extensor digitorum communis Posterior interosseous (radial) C7–8 Extension of the fingers Extensor indicis Posterior interosseous (radial) C7–8 Extensor digiti minimi Posterior interosseous (radial) C7–8 Flexor digitorum profundus Lateral: anterior interosseous (median) Medial: Ulnar C8, T1 C8, T1 Flexion of the fingers (lateral aspect flexes the second and third digits; medial aspect flexes the fourth and fifth digits Flexor digitorum superficialis Median C7–8, T1 Flexion of the fingers TABLE 17-2 Muscle Compartments of the Forearm Compartment Principal Muscles Anterior Pronator teres Flexor carpi radialis Palmaris longus Flexor digitorum superficialis Flexor digitorum profundus Flexor pollicis longus Flexor carpi ulnaris Pronator quadratus Posterior Abductor pollicis longus Extensor pollicis brevis Extensor pollicis longus Extensor digitorum communis Extensor digitorum proprius Extensor digiti quinti Extensor carpi ulnaris Mobile wad Brachioradialis Extensor carpi radialis longus Extensor carpi radialis brevis Anatomic, biomechanic, and electromyographic (EMG) analyses have demonstrated that the prime movers of elbow flexion are the biceps, brachialis, and brachioradialis (see Table 17-1).38 The pronator teres, flexor carpi radialis (FCR), flexor carpi ulnaris (FCU) (Fig. 17-5), and the extensor carpi radialis longus (ECRL) muscles are considered to be weak flexors of the elbow.37 Most elbow flexors, and essentially all the major supinator and pronator muscles, have their distal attachments on the radius.8 Contraction of these muscles, therefore, pulls the radius proximally against the humeroradial joint.39,40 The combined efforts of all the elbow flexors can create large amounts of elbow flexion torque. The interosseous membrane transfers and dissipates a portion of this muscle force to the radius and to the ulna.8 The reverse action of the elbow flexors can be used in a closed-chain activity by bringing the upper arm closer to the forearm such as when performing a pull-up.41 FIGURE 17-5 Muscles of the anterior forearm. (Reproduced, with permission, from Chapter 32. Forearm. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy. New York, NY: McGraw-Hill; 2011.) The biceps is a two-headed muscle that spans two joints. The short head of the biceps arises from the tip of the coracoid process of the scapula where it meshes with the coracobrachialis and pectoralis minor tendon, whereas the long head arises from the supraglenoid tuberosity of the scapula (Fig. 17-2). The biceps has two insertions: a common tendinous insertion at the radial tuberosity and by the lacertus fibrosus (bicipital aponeurosis) that emanates from the biceps muscle belly at the level of the musculotendinous junction and crosses distally and medially to insert along the subcutaneous border of the ulnar (see Fig. 17-2).42 At the elbow, the biceps is a dominant flexor, but its secondary function is supination of the forearm.43 The supination action of the biceps increases the more the elbow is flexed and is maximal at 90 degrees. It diminishes again when the elbow is fully flexed. No,44 or limited,45 biceps muscle activity has been demonstrated during elbow flexion, with the forearm pronated.37 The biceps, via its long head, also functions as a shoulder flexor (see Chapter 16). The brachialis (Fig. 17-6) originates from the lower two-thirds of the anterior surface of the humerus and inserts on the ulnar tuberosity and the coronoid process. The brachialis is the workhorse of the elbow and functions to flex the elbow regardless of the degree of pronation and supination of the forearm,45 It is the most powerful flexor of the elbow when the forearm is pronated.46 FIGURE 17-6 The brachialis muscle. (Reproduced, with permission, from Chapter 31. Arm. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy. New York, NY: McGraw-Hill; 2011.) The brachioradialis (Fig. 17-5) arises from the proximal two-thirds of the lateral supracondylar ridge of the humerus and the lateral intermuscular septum. It travels down the forearm and inserts on the lateral border of the styloid process on the distal aspect of the radius. The brachioradialis appears to have a number of functions, two of which occur with rapid movements of elbow flexion. Initially it functions as a shunt muscle, overcoming centrifugal forces acting on the elbow, and then by adding power to increase the speed of flexion.43 The brachioradialis also functions to bring a pronated or supinated forearm back into the neutral position of pronation and supination. In the neutral or pronated position, the muscle acts as a flexor of the elbow, an action that diminishes when the forearm is held in supination.45,47 The pronator teres (see Fig. 17-5) has two heads of origin: a humeral head and an ulnar head. The humeral head arises from the medial epicondylar ridge of the humerus and common flexor tendon, whereas the ulnar head arises from the medial aspect of the coronoid process of the ulna. The pronator teres inserts on the anterolateral surface of the midpoint of the radius. The muscle functions predominantly to pronate the forearm, but can also assist with elbow flexion.5,46,47 The ECRL arises from a point superior to the lateral epicondyle of the humerus on the lower third of the supracondylar ridge, just distal to the brachioradialis. It travels down the forearm to insert on the posterior surface of the base of the second metacarpal. The muscle functions as a weak flexor of the elbow, as well as assisting with wrist extension and radial deviation. The FCR (see Fig. 17-5) arises from the common flexor tendon on the medial epicondyle of the humerus and inserts on the base of the second and third metacarpal bones. The FCR functions to flex the elbow and wrist but also assists in pronation and radial deviation of the wrist. The FCU (see Fig. 17-5) has two heads of origin. The humeral head arises from the common flexor tendon on the medial epicondyle of the humerus. It inserts on the pisiform, hamate, and fifth metacarpal bones. The FCU functions to assist with elbow flexion in addition to flexion and ulnar deviation of the wrist. See above. The fibers of the pronator quadratus run perpendicular to the direction of the arm, running from the most distal quarter of the anterior ulna to the distal quarter of the anterior radius (see Fig. 17-5). It is the only muscle that attaches only to the ulna at one end and the radius at the other end. The pronator quadratus is the main pronator of the hand. See above. The effectiveness of the biceps as a supinator is greatest when the elbow is flexed to 90 degrees, placing the biceps tendon at a 90-degree angle to the radius. In contrast, with the elbow flexed only 30 degrees, much of the rotational efficiency of the biceps is lost.41 The supinator originates from the lateral epicondyle of the humerus, LCL, the AL, the supinator crest, and the ulnar fossa. It inserts on the superior third of the anterior and lateral surface of the radius. The supinator muscle is a relentless forearm supinator, similar to the brachialis during elbow flexion. The supinator functions to supinate the forearm in any elbow position, while the previously mentioned ECRL and brevis work as supinators during fast movements, and against resistance. The nervous system usually recruits the supinator muscle for low-power tasks that require a supination motion only, while the biceps remains relatively inactive—a fine example of the law of parsimony (see Chapter 3).8 There are two muscles that extend the elbow: the triceps and the anconeus (see Table 17-1). The triceps brachii (Fig. 17-7) has three heads of origin. The long head arises from the infraglenoid tuberosity of the scapula, the lateral head from the posterior and lateral surface of the humerus, and the medial head from the lower posterior surface of the humerus. The muscle inserts on the superoposterior surface of the olecranon and deep fascia of the forearm. The triceps has its maximal force in movements that combine both elbow extension and shoulder extension. Like the biceps, it is a two-joint muscle. The medial head of the triceps is the workhorse of elbow extension, with the lateral and long heads recruited during heavier loads.50 During strong contractions of the triceps, for example, a push-up, which involves a combination of elbow extension and shoulder flexion, as the triceps strongly contracts to extend the elbow, the shoulder simultaneously flexes by the action of the anterior deltoid, which overpowers the shoulder extension torque of the long head of the triceps.41 FIGURE 17-7 The triceps. (Reproduced, with permission, from Chapter 31. Arm. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy. New York, NY: McGraw-Hill; 2011.) The anconeus arises from the lateral epicondyle of the humerus and inserts on the lateral aspect of the olecranon and posterior surface of the ulna. The exact function of the anconeus in humans has yet to be determined, although it appears to be a fourth head of the elbow extension mechanism, similar to the quadriceps of the knee.8 It has been suggested that in addition to assisting with elbow extension, forearm pronation, and supination, the anconeus functions to stabilize the ulnar head in all positions (except radial deviation) and to pull the subanconeus bursa and the joint capsule out of the way during extension, thus avoiding impingement.5,51 The anconeus has also been found to stabilize the elbow during forearm pronation and supination.45 The cubital tunnel, a fibro-osseous canal, was originally described by Feindel and Stratford.53 The ulnar nerve passes through this tunnel. The floor of the tunnel is formed by the MCL, whereas the roof is formed by an aponeurosis, the arcuate ligament, or Osborne’s band, which extends from the medial epicondyle to the olecranon and arises from the origin of the two heads of the FCU.54–57 The medial head of the triceps constitutes the posterior border of the tunnel, and its anterior and lateral borders are formed by the medial epicondyle and olecranon, respectively.30 The volume of the cubital tunnel is greatest with the elbow held in extension.58 As the elbow is brought into full flexion, there is a 55% decrease in canal volume.54 Vanderpool et al.59 reported that with each 45 degrees of flexion of the elbow, there was a concomitant 5-mm increase in distance between the ulnar and humeral attachments of the arcuate ligament. At full elbow flexion, there was a 40% elongation of the ligament and a decrease in canal height of approximately 2.5 mm. A few other factors have been associated with a decrease in the size of the cubital tunnel. These include space-occupying lesions, osteoarthritis, rheumatoid arthritis, heterotopic bone formation, or trauma to the nerve.58 Patients with systemic conditions such as diabetes mellitus, hypothyroidism, alcoholism, and renal failure also may have a predisposition.60 Bulging of the MCL has also been described as a factor.59 More than 40% of athletes with valgus instability develop ulnar neuritis secondary to irritation from inflammation of the MCL.61,62 O’Driscoll et al.57 reported that the groove on the inferior aspect of the medial epicondyle was not as deep as the groove posteriorly, and the floor of the canal seems to rise with elbow flexion.57 These changes lead to an alteration of the cross-sectional area of the cubital tunnel from a rounded surface to a triangular or elliptic surface with elbow flexion.54,58 The cubital fossa (Fig. 17-8) represents a triangular space, or depression that is located on the anterior surface of the elbow joint, and which serves as an “entry way” to the forearm, or antebrachium. The boundaries of the fossa are as follows: FIGURE 17-8 The cubital fossa. (Reproduced, with permission, from Chapter 32. Forearm. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy. New York, NY: McGraw-Hill; 2011.) The contents of the fossa include (see Fig. 17-8): The neurologic supply of the bones, joints, muscles, and skin of the elbow and forearm is derived from the C5 through C8 nerve roots, which exit from the intervertebral foramina of C4–5 through C7–T1 (Figs. 17-6 and 17-9).63 FIGURE 17-9 Nerve supply of the elbow and forearm. (Reproduced, with permission, from Chapter 31. Arm. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy. New York, NY: McGraw-Hill; 2011.) From its origin as the largest branch of the medial cord of the brachial plexus, the ulnar nerve continues along the anterior compartment of the arm, before passing through the medial intermuscular septum at the level of the coracobrachialis insertion. At the level of the elbow, the ulnar nerve passes posterior to the medial epicondyle, where it enters the cubital tunnel. Ulnar nerve compression in the cubital tunnel is a common entrapment neuropathy of the upper extremity, second only to carpal tunnel syndrome (CTS).64 After leaving the cubital tunnel, the ulnar nerve passes between the two heads of the FCU origin and traverses the deep flexor–pronator aponeurosis.65,66 The median nerve extends medially down the upper arm across the anterior aspect of elbow joint. The ligament of Struthers arises from an abnormal spur on the shaft of the humerus and runs to the medial supracondylar process.56 The supracondylar process with its ligamentous extension encloses a foramen, bounded medially by the medial intermuscular septum, and the distal anterior surface of the medial epicondyle, through which the brachial artery and median nerve pass.67 As the median nerve passes through the cubital fossa, the anterior interosseous nerve (AIN) branches off it, as it passes through the two heads of the pronator teres muscle. The AIN supplies the motor innervation to the index and middle flexor digitorum profundus (FDP), the flexor pollicis longus (FPL), and the pronator quadratus. The radial nerve sits superiorly and medially in the upper arm and winds around the humeral shaft. At a point approximately 10–12 cm proximal to the elbow joint, the radial nerve passes from the posterior compartment of the arm by piercing the lateral intermuscular septum.68 The nerve travels in the anterior forearm between the brachialis muscle and the biceps tendon medially, and the brachioradialis, ECRL, and ECRB muscles laterally.68 Within an area approximately 3 cm proximal or distal to the elbow joint, the radial nerve branches into a deep mixed nerve, the posterior interosseous nerve (PIN), and a superficial sensory branch.69,70 After dividing, the two terminal divisions usually follow the same course, sharing a single epineurium for several centimeters, before the superficial radial nerve moves anteriorly to lie on the undersurface of the brachioradialis, and the deep branch travels posteriorly to enter the radial tunnel/supinator canal, distal to the origin of the ECRB, at the level of the radiohumeral joint.68 Entering the canal, the deep branch supplies the ECRB then passes deep to the superficial head of the supinator, where the arcade of Fröhse1 can impinge on the nerve.71,72 The nerve continues between the two heads of the supinator and innervates this muscle during its passage to the posterolateral aspect of the radius. On emerging from the supinator, a motor division (supplying the abductor pollicis longus, extensor pollicis brevis, extensor indicis proprius, and extensor pollicis longus muscles) and a mixed lateral branch (supplying the extensor carpi ulnaris [ECU], extensor digitorum communis, and extensor digiti minimi muscles) are recognized. The lateral branch continues along the posterior-radial border of the radius to the wrist as the sensory branch of the PIN, which innervates the posterior (dorsal) capsule of the wrist and intercarpal joints (see Chapter 18).68,72 The radial tunnel lies on the anterior aspect of the radius and is approximately three to four fingerbreadths long, beginning just proximal to the radiohumeral joint and ending at the site where the PIN passes deep to the superficial part of the supinator muscle.73 The lateral wall of the tunnel is formed by the brachioradialis, ECRL, and ECRB. These muscles cross over the nerve to form the anterior wall of the radial tunnel as well, while the floor of the tunnel is formed by the capsule of the humeroradial joint, and the medial wall is composed of the brachialis and biceps tendon.68 The vascular supply to the elbow (Fig. 17-10) includes the brachial artery, the radial and ulnar arteries, the middle and radial collateral artery laterally, and the superior and inferior ulnar collateral arteries.37 FIGURE 17-10 Vascular supply of the elbow and forearm. (Reproduced, with permission, from Chapter 31. Arm. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy. New York, NY: McGraw-Hill; 2011.) 1The arcade of Fröhse is an inverted arched structure that lies within 1 cm distal of the fibrous edge of the ECRB and approximately 2–4 cm distal to the radiohumeral joint. It represents the proximal border of the superficial head of the supinator, through which the radial nerve passes. There is still controversy in the literature as to the precise biomechanics of the elbow,74 and how the axes of motion relate to the anatomy of the joint. Biomechanically, the elbow predominantly functions as an important central link in the upper extremity kinetic chain, allowing for the generation and transfer of forces that occur in the upper extremity. The common stresses that occur at the elbow include valgus stress, which results in medial tension and lateral compression loading; varus stress, which results in lateral tension loading; extension stress; and multiple combinations of these stresses. These forces produce repetitive tensile loads on the ligamentous and muscular support systems around the elbow, and compressive and shear loads on the bony constraints.75 Truly impressive loads can be placed on the elbow during activities such as throwing or pitching (see Chapter 30). It is important that the elbow is able to move freely and painlessly throughout its available motion. These motions include elbow flexion and extension, and forearm pronation and supination. Flexion–extension of the elbow complex occurs about a relatively fixed axis of rotation passing through the center of arcs formed by the trochlea and the capitellum (Fig. 17-1). The maximal range of passive motion generally available to the elbow is from 5 degrees of hyperextension to 145 degrees of flexion. Full active extension in the normal elbow is some 5–10 degrees short of that obtainable by forced extension, due to passive muscular restraints (biceps, brachialis, and supinator).76,77 Passive extension is limited by the impact of the olecranon process on the olecranon fossa, tension in the dermis, the fibers of the MCL, and the anterior capsule.78 Excessive ectopic bone formation around the olecranon fossa can also limit full passive extension. Passive flexion is limited by bony structures (the head of the radius against the radial fossa and the coronoid process against the coronoid fossa), tension of the posterior capsular ligament, soft-tissue approximation, and passive tension in the triceps.78 Pronation and supination require simultaneous joint movement at the proximal and distal radioulnar joints (Fig. 17-3).8 The longitudinal axis of rotation about which supination and pronation occur is considered to pass through the center of the head of the radius to the convex articular surface of the ulnar at the distal radioulnar joint. Supination at the proximal radioulnar joint occurs as a spinning of the radial head within the fibro-osseous ring formed by the AL and radial notch of the ulna.8 The arthrokinematics of pronation at the proximal radioulnar joint occurs by similar mechanisms. Restrictions in the passive range of pronation and supination motions can occur from tightness in muscle and/or connective tissues (Table 17-3).79,80 TABLE 17-3 Structures that can Restrict Supination and Pronation Limit Supination Limit Pronation Pronator teres, pronator quadratus Biceps or supinator muscles Palmar capsular ligament at the distal radioulnar joint Posterior (dorsal) capsular ligament at the distal radioulnar joint Oblique cord, interosseous membrane, and quadrate ligament Ulnocarpal complex Ulnocarpal complex Data from Neumann DA. Elbow and forearm complex. In: Neumann DA, ed. Kinesiology of the Musculoskeletal System: Foundations for Physical Rehabilitation. St. Louis, MO: Mosby, 2002:133–171. Data from Kleinman WB, Graham TJ. The distal radioulnar joint capsule: Clinical anatomy and role in posttraumatic limitation of forearm rotation. J Hand Surg Am. 1998;23:588–599. Data from Bert JM, Linscheid RL, McElfresh EC. Rotatory contracture of the forearm. J Bone Joint Surg Am. 1980;62:1163–1168. The motions that occur at the humeroulnar joint involve impure flexion and extension, which are primarily the result of rotation of the concave trochlear notch of the ulna about the convex trochlea of the humerus. At the humeroulnar articulation, flexion involves an anterior roll and a distal/anterior slide at the ulnar joint surface. During extension, there is a posterior roll and a proximal/posterior slide at the ulnar joint surface. From a sagittal section, the firm mechanical link between the trochlear and the trochlear notch, however, limits the motion to essentially a sagittal plane.8 Any motion at the elbow and forearm complex involves motion at the humeroradial joint. Thus, any limitation of motion at the humeroradial joint can disrupt both flexion and extension, and pronation and supination.8 During flexion and extension of the elbow, the humeroradial joint follows the pathway dictated by the anatomy of the ulnohumeral joint to which it is firmly attached by the annular and interosseous ligaments.63 At the humeroradial articulation, flexion involves an anterior roll and an anterior slide at the radial joint surface. During extension, there is a posterior roll and a posterior slide at the radial joint surface. At rest in full extension, little if any physical contact exists at the humeroradial joint.8,81 During active flexion, however, muscle contraction pulls the radial fovea against the capitulum.82,83 Some supination and pronation also occur at this joint due to a spinning of the radial head. Although the humeroradial joint provides minimal structural stability to the elbow complex, it does provide an important bony resistance against a valgus force.8,21 At the proximal radioulnar joint, one degree of freedom exists, permitting pronation and supination (Fig. 17-3). Both the fascia and the musculature of the forearm depend on the integrity of the interosseous radioulnar relationship for their mechanical efficiency.63 The proximal radioulnar joint is structurally an ovoid, with very little swing available to it due to its ligamentous constraints. As a consequence, its movement is confined to accommodating the osteokinematic spin of the radius. As the radial head forms the convex partner, there is a tendency for the radial head to move posterolaterally during pronation and anteromedially during supination, but these movements are strongly curtailed by the annular and interosseous ligaments. At the joint surfaces, pronation involves an anterior roll of the complex rim of the radial head and a posterior slide. During supination, there is a posterior roll of the rim of the radial head and an anterior slide. Conjunct rotations occur at the elbow complex with all motions. In addition, the elbow motions of flexion and extension are associated with adduction and abduction motions. The ability to abduct and adduct can easily be observed during pronation and supination. In the fully supinated position, the ulna is much nearer the midline of the body than it is in full pronation. Therefore, abduction occurs with pronation, and adduction occurs with supination. The abduction that occurs with extension occurs at the humeroulnar joint and is more apparent than real. An increase in the carrying angle of the forearm during extension must not be confused with the abduction of the ulna, which occurs because of the unequal ranges of extension between the ulna and the humerus, and the radius and the humerus (the capitellum being oriented more anteriorly than the trochlear). This inequity produces a conjunct humeral adduction with flexion and a conjunct humeroulnar abduction with extension, both of which are controlled by the lateral and MCL.63 Thus, it is apparent that pronation–supination and flexion–extension are interdependent, and each is a conjunct motion of the other, at least at the extremes of the range. Since pronation and supination involve the proximal and distal radioulnar joints and the humeroulnar, humeroradial, and radiocarpal joints, mechanical dysfunction of any of these joints may become apparent, especially in the extremes of elbow flexion or extension.63 The role of the elbow musculature as dynamic joint stabilizers is still somewhat unclear. Both varus and valgus forces are produced by muscles during elbow motions. The valgus forces are produced by the ECU, EDC, ECRL, and brachioradialis, while varus forces are produced by the FCR, FDS, pronator teres, and FCU. Forces transmitted across the articulating surfaces include the forces created by muscles working together to produce the desired activity. The important force couples of the elbow include:84
CHAPTER 17
Elbow
OVERVIEW
ANATOMY
HUMEROULNAR JOINT
HUMERORADIAL JOINT
PROXIMAL RADIOULNAR JOINT
LIGAMENTS
Medial Ligament Complex
Anterior Bundle
 The anterior band of the anterior bundle is the most important component of the ligamentous complex, because it primarily stabilizes the elbow against valgus stress in the ranges of 0–60 degrees of flexion, and becomes a secondary restraint with further flexion.3,14,17,20–22,24,26,28 The anterior band is primarily responsible for stability against valgus stresses at 30, 60, and 90 degrees of flexion, making it the most important component in resisting the valgus forces associated with overhead sports activities.1 Recently, Ochi et al.15 determined that the deep middle portion of the anterior band, previously described as the “guiding bundle,”27 is a prime limiting factor in humeroulnar motion.22,29
The anterior band of the anterior bundle is the most important component of the ligamentous complex, because it primarily stabilizes the elbow against valgus stress in the ranges of 0–60 degrees of flexion, and becomes a secondary restraint with further flexion.3,14,17,20–22,24,26,28 The anterior band is primarily responsible for stability against valgus stresses at 30, 60, and 90 degrees of flexion, making it the most important component in resisting the valgus forces associated with overhead sports activities.1 Recently, Ochi et al.15 determined that the deep middle portion of the anterior band, previously described as the “guiding bundle,”27 is a prime limiting factor in humeroulnar motion.22,29
 The posterior band is taut from 60 to 120 degrees of elbow flexion and is a secondary restraint to valgus stress at 30 degrees and 90 degrees of flexion, but a primary restraint to valgus at 120 degrees of elbow flexion.26 The posterior band functions as an equal co-restraint with the anterior band at terminal elbow flexion,3,19,22,26,28 and also acts as a primary restraint to passive elbow extension. In the higher degrees of flexion, the posterior band is nearly isometric and is thus functionally important in the overhead athlete in counteracting valgus stresses.30
The posterior band is taut from 60 to 120 degrees of elbow flexion and is a secondary restraint to valgus stress at 30 degrees and 90 degrees of flexion, but a primary restraint to valgus at 120 degrees of elbow flexion.26 The posterior band functions as an equal co-restraint with the anterior band at terminal elbow flexion,3,19,22,26,28 and also acts as a primary restraint to passive elbow extension. In the higher degrees of flexion, the posterior band is nearly isometric and is thus functionally important in the overhead athlete in counteracting valgus stresses.30
Oblique (Transverse) Bundle
Posterior Oblique Bundle
Lateral Ligament Complex
Annular Ligament
Quadrate Ligament
BURSAE
Muscles
Elbow Flexors
Biceps Brachii
Brachialis
Brachioradialis
Pronator Teres
Extensor Carpi Radialis Longus
Flexor Carpi Radialis
Flexor Carpi Ulnaris
Forearm Pronators
Pronator Teres
Pronator Quadratus
Flexor Carpi Radialis
Forearm Supinators
Biceps
Supinator
Elbow Extensors
Triceps Brachii
Anconeus
CUBITAL TUNNEL
CUBITAL FOSSA
 Lateral. Brachioradialis and ECRL muscles;
Lateral. Brachioradialis and ECRL muscles;
 Medial. Pronator teres muscle;
Medial. Pronator teres muscle;
 Proximal. An imaginary line that passes through the humeral condyles;
Proximal. An imaginary line that passes through the humeral condyles;
 Floor. Brachialis muscle.
Floor. Brachialis muscle.
 the tendon of the biceps brachii, which lies as the central structure in the fossa;
the tendon of the biceps brachii, which lies as the central structure in the fossa;
 the median nerve, which runs along the lateral edge of the pronator teres muscle;
the median nerve, which runs along the lateral edge of the pronator teres muscle;
 the brachial artery, which enters the fossa just lateral to the median nerve and just medial to the biceps brachii tendon;
the brachial artery, which enters the fossa just lateral to the median nerve and just medial to the biceps brachii tendon;
 the radial nerve (not shown), which runs along the medial edge of the brachioradialis and ECRL muscles and is vulnerable to injury here; and
the radial nerve (not shown), which runs along the medial edge of the brachioradialis and ECRL muscles and is vulnerable to injury here; and
 the median cubital or intermediate cubital cutaneous vein, which crosses the surface of the fossa.
the median cubital or intermediate cubital cutaneous vein, which crosses the surface of the fossa.
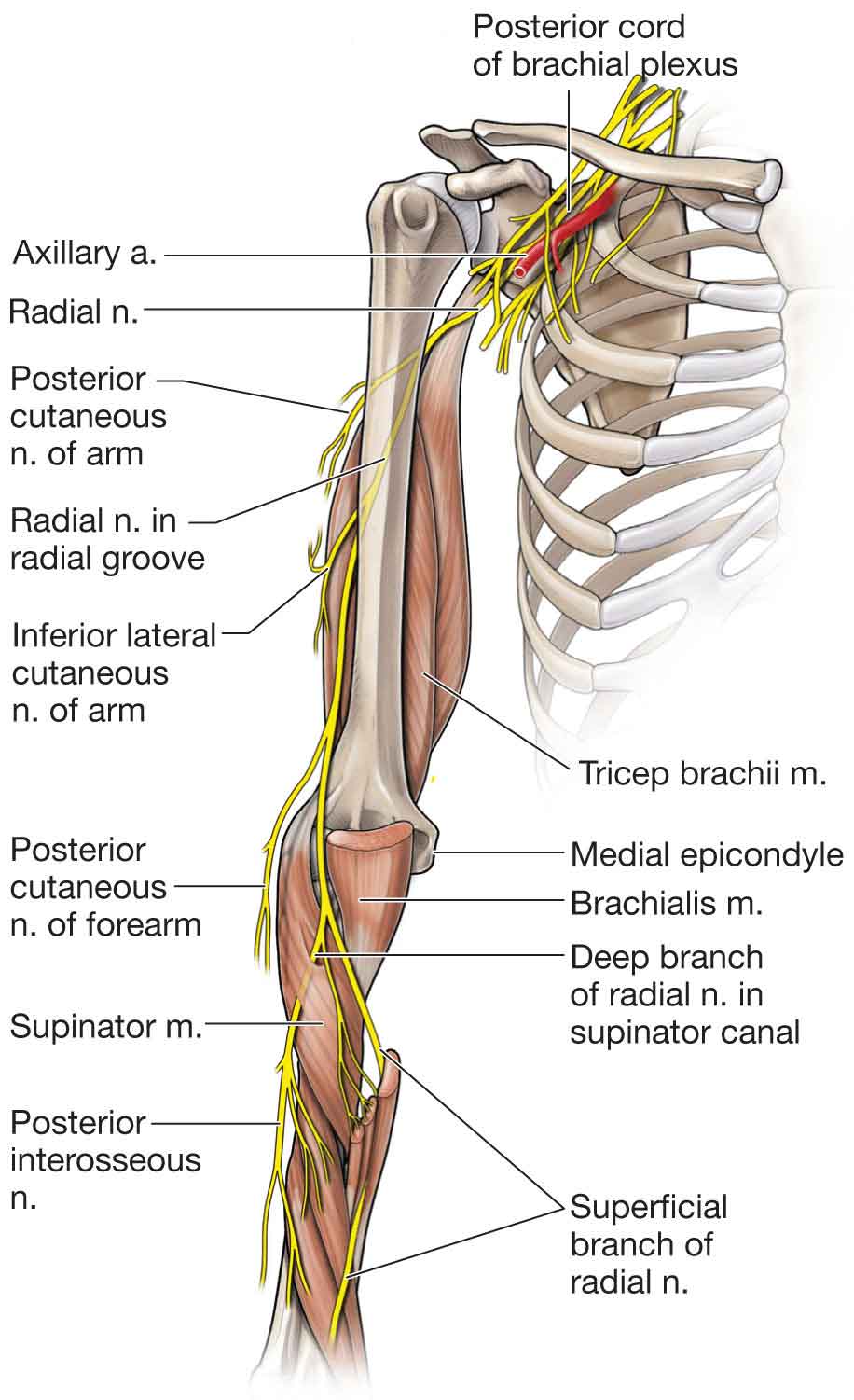
NERVES
Ulnar Nerve (C8–T1)
Median Nerve (C5–T1)
Radial Nerve (C5–T1)
The Radial Tunnel/Supinator Canal
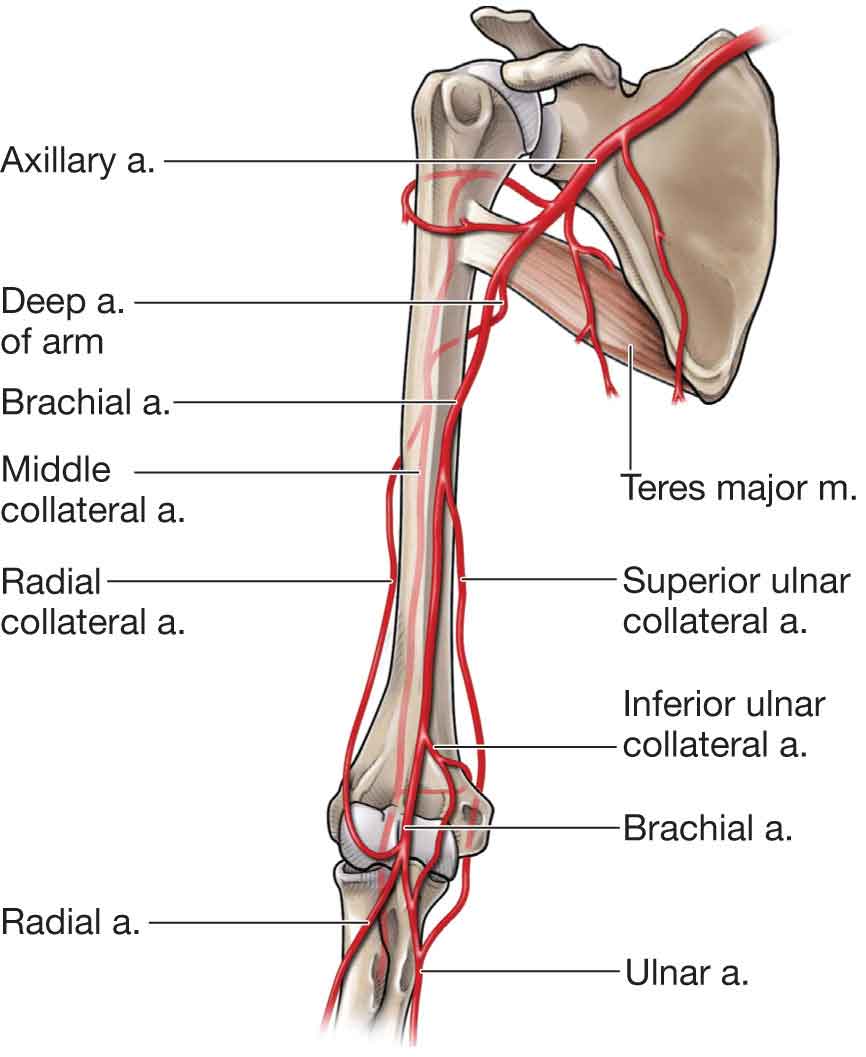
VASCULAR SUPPLY
BIOMECHANICS
Flexion–Extension
Supination–Pronation
HUMEROULNAR JOINT
HUMERORADIAL JOINT
PROXIMAL RADIOULNAR JOINT
COUPLED MOTIONS
FORCE COUPLES OF THE ELBOW
 the triceps/biceps during elbow extension and flexion;
the triceps/biceps during elbow extension and flexion;
 pronator teres and pronator quadratus/supinator during forearm pronation and supination;
pronator teres and pronator quadratus/supinator during forearm pronation and supination;
 FCR, FCU, flexor digitorum communis/ECRL, ECRB, and extensor communis during wrist flexion and extension; and
FCR, FCU, flexor digitorum communis/ECRL, ECRB, and extensor communis during wrist flexion and extension; and
 triceps/biceps and brachioradialis; pronator teres/supinator; and FCR, FCU/ECRB, and ECRL during activities requiring elbow stabilization.
triceps/biceps and brachioradialis; pronator teres/supinator; and FCR, FCU/ECRB, and ECRL during activities requiring elbow stabilization.Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree




