Ectrodactyly
Cornelius M. Donohue
The first description of central deficiencies was published in 1770 by Hartsinck, who reported on certain blacks called Touvingas, or “two-fingered Negroes,” in Dutch Guiana who had similar bilateral hand and foot deformities (4). Cruveilhier first coined the term lobster claw deformity in 1829. His patients had the characteristic absence of the second, third, and fourth rays, with medial deviation of the fifth toe and hallux abductus (5).
Congenital split and cleft foot (lobster foot, partial adactyly, ectrodactyly) are common terms for one of at least 175 types of skeletal dysplasia describing a congenital absence of two or three central rays or digits (1,2 and 3). Cleft foot is an anomaly in which a single cleft extends proximally into the foot, sometimes even as far as the midfoot. Generally, one or more toes and parts of their metatarsals are absent, and often the tarsals are abnormal. Although the deformity varies in degree and type, the first and fifth rays usually are present. Although unilateral and bilateral cleft foot may occur as an isolated deformity, it is usually associated with lobster clawing of the hand and other deformities, including cleft lip and cleft palate (4,5,6,7 and 8) (Fig. 75.10). Wood found that 9 of 20 patients with cleft hand deformity also had cleft foot deformity (8). Cleft foot is sometimes manifested as part of a multiple-defect syndrome such as ectrodactyly-ectodermal dysplasia-clefting syndrome, sometimes referred to as EEC syndrome, with pathology including cleft lip and palate, ectodermal defects, and genitourinary anomalies (9).
Upper and lower extremity structural limb abnormalities include three types of deformities: skeletal dysplasias (e.g., cleft foot and hand), reduction defects (e.g., achondroplasia), and supernumerary growth (e.g., polydactyly). They may result from a variety of causes including: teratogens, single-gene defects, chromosomal abnormalities, secondary destruction (e.g., amniotic band syndrome), mechanical restriction of fetal movement (e.g., extrinsic or postural clubfoot), and multifactorial conditions (e.g., intrinsic clubfoot). A high proportion of isolated bilateral defects are inherited as single-gene traits, whereas unilateral or asymmetric defects are more likely to be nongenetic, such as amniotic band syndrome (10).
Skeletal dysplasias are a genetically heterogeneous group of conditions characterized by the disturbance of the normal process of bone development (11,12). The prevalence of skeletal dysplasias ranges from 2.3 to 7.6 per 10,000 births and approximately 1.5 per 10,000 births for lethal skeletal dysplasias (13,14 and 15). The International Working Group on Constitutional Diseases of Bone has published an international classification of osteochondrodysplasias that categorizes the disorders based on radiodiagnostic criteria (16).
INCIDENCE AND EMBRYOLOGIC PERSPECTIVE
Cleft foot is a rare congenital deformity with an estimated incidence of 1 in 180,000 live births. It is important to note, however, that this is only an estimate because of the rare occurrence of this deformity and the difficulty with developing sound epidemiologic analyses. It is considered to be inherited as an autosomal dominant trait with variable penetrance (17). Some investigators believe that isolated cleft foot may be related to external exposure of certain gene loci to outside agents. In addition, it has been reported that a child exposed in utero to a retinoic acid derivative, during the period of crucial limb development, was born with absent digits and syndactyly (3).
Regarding deformities like cleft foot, it is believed that something occurs during the first trimester of gestation to disturb the normal development of the cartilaginous bone models in the apical portion of the limbs (17). The development of the embryo is most easily disturbed during the organogenetic period, which includes the 4th through the 8th week of the embryonic period (18).
The skeletal system develops from limb buds composed of mesodermal and neural crest cells (ectoderm). The appendicular skeleton consists of the pectoral and pelvic girdles and the limb bones. The lower limb buds appear toward the end of the 4th week (day 27) as slight elevations of the ventrolateral body wall. The apical ectodermal ridge of the limb bud has an inductive influence on the mesenchyme in the limb bud; it promotes growth of the mesenchyme and appears to give it the ability to form specific cartilaginous elements (19,20). Mesenchymal bones form during the 5th week as condensations of mesenchyme appear in the limb buds. During the 6th week, the mesenchymal bone models in the limbs undergo chondrification to form hyaline cartilage bone models. Bones first appear as condensations of mesenchymal cells. This condensation marks the beginning of selective gene activity that precedes cell differentiation into these hyaline cartilage bone models. This limb bud patterning of hyaline cartilage bone models is regulated by homeobox-containing (Hox) genes. Ossification begins in the long bones by the 8th week of embryonic development and initially occurs in the diaphyses of the bones from primary centers of ossification. By 12 weeks, primary ossification centers have appeared in nearly all bones of the limbs. The limb buds elongate by proliferation of the mesenchyme within them (19,20). Programmed cell death or apoptosis is an important mechanism in limb development, for example, in the formation of the notches between the digital rays. Limb muscles are also derived from mesenchyme (myogenic precursor cells) originating in the somites of the embryo. The muscle-forming cells (myoblasts) then form dorsal and ventral masses as they attach to specific cartilaginous boney models (18) (Fig. 75.11).
Descriptive terms such as amelia and meromelia have been used to define complete absence of a limb or limbs and partial absence of a limb or limbs, respectively. It is quite interesting to note, regarding the timing of mechanisms of malformations, that suppression of limb bud development during the early part of the 4th week results in amelia but arrest or disturbance of differentiation or growth of the limbs during the 5th week results in various type of meromelia, including cleft foot deformity (18).
 Figure 75.10 Seven-year-old female with bilateral cleft foot and cleft hand deformity. A: Plantar view of both feet. B: Plantar view of right foot. C: Dorsal view of right hand. |
PATHOPHYSIOLOGY
It is customary to divide the causes of congenital malformations into the following:
Genetic factors, for example, the chromosomal abnormalities associated with trisomy 18
Mutant genes, for example, as in brachydactyly or osteogenesis imperfecta
Environmental factors, for example, teratogens such as thalidomide
Combination of genetic and environmental factors (multifactorial inheritance), for example, intrinsic clubfoot
Vascular disruption and ischemia, for example, limb reduction defects
However, it is not always possible to separate clearly the factors that cause the abnormalities (18).
Patten described six mechanisms that can cause congenital malformations such as cleft foot during this extremely vulnerable period in development: too little growth, too little resorption, too much resorption, resorption in the wrong direction, normal growth in an abnormal position, and local overgrowth of a tissue or structure (21).
In cleft foot deformities, it has been observed clinically and radiographically that when a metatarsal is missing, so too is the corresponding digit (ectrodactyly), reinforcing the concept that the metatarsal and corresponding digit are derived from the same embryologic cartilaginous precursor (2).
The final common pathway of cartilaginous precursors being transformed by enchondral ossification can also explain
the possible clinical spectrum of deformities, from isolated cleft foot deformities to cleft foot deformities as part of a more extensive skeletal dysplasia such as ECC or simultaneous appearance of cleft foot and hand in the same patient, depending on the nature and extent of gene mutation(s) or chromosomal defects impacting on the many interacting events occurring during the first trimester of fetal development.
the possible clinical spectrum of deformities, from isolated cleft foot deformities to cleft foot deformities as part of a more extensive skeletal dysplasia such as ECC or simultaneous appearance of cleft foot and hand in the same patient, depending on the nature and extent of gene mutation(s) or chromosomal defects impacting on the many interacting events occurring during the first trimester of fetal development.
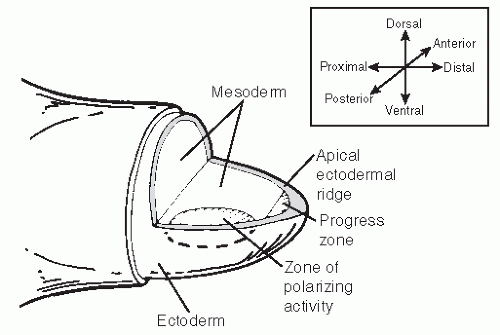 Figure 75.11 Limb bud. Apical ectodermal ridge extends from anterior to posterior along dorsal/ventral boundary of growing limb bud. Proximal to apical ectodermal ridge is the progress zone (an area of proliferating mesodermal cells). In posterior mesoderm is the zone of polarizing activity, an important signaling center. These centers are interconnected, so limb patterning and growth are partly dependent on coordinated function. (Redrawn after Jorde LB, Carey JC, Bamshad M, White RW. Medical genetics. London, UK: Mosby, 1999.) |
A model for understanding cleft foot, and congenital malformations in general, should include three interacting variables: primary, representing the intrinsic genetic deformity of the bone or, more appropriately, a defect in the cartilaginous precursor for a specific bone; secondary, which is the effect of external forces, such as muscular attachments (symmetrical and asymmetrical)on the bone; and tertiary, the external forces on the bone itself (intrauterine pressure, weight-bearing), which can contribute tertiary forces to maintain the deformity already established by primary and secondary forces (Fig. 75.12).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


