Chapter 86 Echinacea Species (Narrow-Leafed Purple Coneflower)
Echinacea spp. (family: Asteraceae)
Common names: narrow-leafed purple coneflower, black sampson, snakeroot
Common name: purple coneflower
Common name: pale purple coneflower
 General Description
General Description
Echinacea spp. are perennial herbs native to Midwestern North America, from Saskatchewan to Texas. The genus derives its name from the Greek echinos, meaning sea urchin. This refers to the prickly scales of the dried seed head portion of the flower. Nine species of echinacea have been taxonomically classified by McGregor on the basis of comparative anatomy and morphology (Table 86-1).1
TABLE 86-1 Taxonomic Formation of the Genus Echinacea
| SPECIES | SYNONYMS |
|---|---|
| Echinacea angustifolia | Brauneria angustifolia |
| E. atrorubens | Rudbeckia atrorubens |
| E. laevigata | B. laevigata |
| E. pallida | R. pallida, B. pallida |
| E. paradoxa | B. paradoxa |
| E. purpurea | R. purpurea |
| R. hispida | |
| R. serotina | |
| E. speciosa | E. simulata |
| E. intermedia | |
| E. sanguinea | |
| E. tennesseensis | B. tennesseensis |
Modified from McGregor RL. The taxonomy of the genus Echinacea (Compositae). Univ Kansas Sci Bull. 1968;48:113-142.
Of the nine species, Echinacea angustifolia, E. purpurea, and E. pallida are the most commonly used clinically.2 E. angustifolia, with a typical height of up to 2 ft, is shorter than E. purpurea (1.5 to 5 ft) and E. pallida (1 to 3 ft). Another key to species identification is that E. angustifolia and E. purpurea have yellow pollen, whereas E. pallida is noticeably paler and has white pollen. The portions of the plant used for medicinal purposes include the aerial portion, the whole plant including the root, and the root itself. The tap root of E. angustifolia can reach a length of 3 to 4 ft.3
 Chemical Composition
Chemical Composition
In the case of echinacea, it appears that although individual immune-enhancing compounds produce significant effects when they are combined in meaningful amounts, there is an additive effect. The immune-enhancing components of echinacea work together in a harmonious fashion to produce the phenomena of synergy. A key manner in which echinacea affects immune function is via enhancing the ability of macrophages to engulf and destroy particulate matter. The specific components of echinacea that possess this action are the polysaccharides, alkylamides, and cichoric acid. Although each component is effective alone, the greatest degree of enhancement was noted when the three active components were used in a specific ratio (0.25, 2.5, and 25 mg/mL).4 This phenomena of synergy was noted with a clear dose-dependent effect. In other words, the effects with the three actives were greater than any individual active and the higher the dosage, the greater the effect on enhancing macrophage function. A similar effect was noted in the ability of macrophages to detect the presence of foreign matter in the blood and signal the other components of the immune system to mount an attack via interleukin-1 (IL-1) and granulocyte colony-stimulating factor.
Because echinacea contains a wide assortment of chemical constituents with confirmed immune-enhancing effects, this is important for manufacturers to recognize to ensure sufficient levels of all these active compounds. Unfortunately, most echinacea products on the market do not specify the levels of active compounds because they have not been analyzed for them. In addition, when manufacturers do state the level of a particular marker compound, most consumers fail to realize that concentrating only for one particular active compound of echinacea results in loss of other constituents and, as a result, all of the synergistic effects. For example, some manufacturers standardize for “total phenolic content” or the compound echinacoside.5 Although these types of echinacea extracts were found to have some antioxidant properties, recent studies found them to have no effect on enhancing immune function in experimental animal studies.6,7
Growing understanding of the chemical composition of echinacea requires manufacturers to perform quality control tests not only on the finished product, but also on the plant to ensure that it is being grown properly and harvested at the exact time for maximal levels of all active compounds. It is imperative that echinacea be treated properly after harvesting. In addition, studies indicate that a significant amount of the active ingredients are destroyed in the drying process. If the fresh plant material is not processed immediately, the content of several key components—especially cichoric acid and alkylamides—will be low (as much as 80% will be lost).8–10 Chemical analysis of commercial echinacea preparations demonstrated tremendous variation in the levels of key compounds. For example, one analysis of various commercial echinacea products found that there was not only tremendous variation in the level of cichoric acid, with most products containing either none or little, but even within the same product there was tremendous interbatch variation.11
Polysaccharides
A number of immunostimulatory and mild anti-inflammatory polysaccharides have been isolated from Echinacea spp.2,3,12–15 Most notable are inulin, which is found in a high concentration (5.9%) in E. angustifolia root, and the high-molecular-weight (25,000 to 50,000) polysaccharides found in the aerial part of E. purpurea. These components possess significant immune-enhancing properties. Typically, the most potent immune-enhancing polysaccharides are the water-soluble, acidic, branched-chain heteroglycans composed of many types of sugars rather than the polyfructose content of inulin.
Alkylamides
Alkylamides typically exert a tingling sensation on the tongue, which is representative of their mild anesthetic effect. These compounds are found in highest concentrations in the roots. The roots of E. angustifolia contain higher concentrations (0.004% to 0.039%) than E. purpurea (0.009% to 0.151%) and E. pallida (0.001%).16,17 Alkylamides are among the most active constituents of echinacea on macrophage function.18 In a human pharmacokinetic study, alkylamides were detected in plasma 20 minutes after ingestion of an echinacea preparation, and indicated that dosing at least three times a day was required to maintain plasma concentrations.19
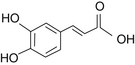
Caffeic Acid Derivatives
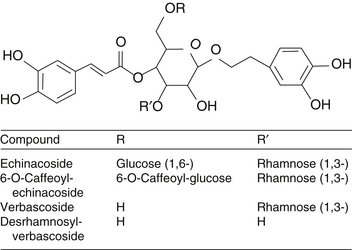
Caffeic acid serves as the backbone for a number of important medicinal plant compounds in other plants, as well as Echinacea spp. (Figure 86-1). The first compound believed to be unique to Echinacea was echinacoside, a compound eventually shown to be composed of caffeic acid, a caffeic acid derivative (similar to catechol), glucose, and rhamnose, all attached to a central glucose molecule (Figures 86-2 and 86-3).20 Echinacoside accumulates in the roots but is also found in smaller concentrations in the flowers. The roots of E. angustifolia contain 0.3% to 1.3%, whereas the roots of E. pallida contain a similar concentration of 0.4% to 1.7%.12 It is assumed that E. purpurea has similar echinacoside levels as well.
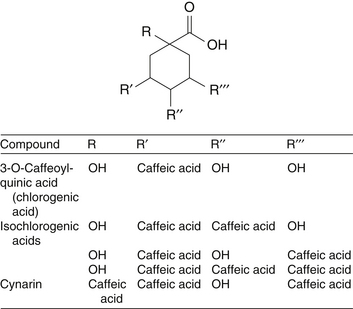
Other caffeic acid derivatives important in the pharmacology of Echinacea include cichoric acid, chlorogenic acid, and cynarin.3 Cichoric acid was originally isolated from E. purpurea and is found in much higher concentrations in this species compared with E. angustifolia and E. pallida.3,21 However, E. angustifolia and E. pallida have higher amounts of other types of caffeic acid derivatives. These differences are not thought to have much clinical significance; rather, they may prove to be valuable in quick chemical differentiation of species.
Flavonoids
The leaves and stems of E. angustifolia and E. purpurea have been shown to contain numerous flavonoids, with rutoside being the most abundant.3 The total flavonoid content (calculated as quercetin) for E. angustifolia and E. purpurea was 0.48% and 0.38%, respectively.3
Essential Oils
The essential oil content varies among the three common species22:
• E. angustifolia root and leaves contain less than 0.1%.
• E. purpurea root contains 0.2%, and flowers and leaves contain 0.6%.
• E. pallida root contains up to 2%, and the leaves contain less than 1%.
Interestingly, in one study, the essential oil content of E. pallida root was found to rise to 3.5% to 4% in April and May but fall to 1% to 1.5% for the rest of the year.23 The major essential oil components are sesquiterpene derivatives, borneol, α-pinine, and related aromatic compounds.3
Polyacetylenes
A number of polyacetylenes have been identified from the roots of all three commercial species.24 The difference in the type of polyacetylene and susceptibility to breakdown may help to differentiate which species is best for commercial use. Because the polyacetylenes of E. pallida are quite susceptible to autoxidation, E. angustifolia may be better for commercial products.25 Research showed that long-term storage greatly decreases the content of polyacetylenes to only trace levels at best. However, the polyacetylene derivatives of autoxidation of E. pallida are quite characteristic and useful in differentiating E. pallida from E. angustifolia.
Miscellaneous
Undoubtedly, other constituents contribute to the pharmacology of echinacea. The occurrence of a “colorless alkaloid” was first reported by the great John Uri Lloyd in 1897 and substantiated recently by the isolation of the alkaloids tussilagine and isotussilagine.26 Other compounds isolated from Echinacea spp. include the following3:
 History and Folk Use
History and Folk Use
Echinacea was used extensively by the Native Americans living in areas where it grew. American Indians used echinacea against more illnesses than any other plant. The root was used externally for the healing of wounds, burns, abscesses, and insect bites; internally for infections, toothache, and joint pains; and as an antidote for rattlesnake bites.27
H.C.F. Meyer, a German lay healer, introduced a commercial product containing echinacea to Americans around 1870. He recommended “Meyer’s blood purifier”3 as a wonder cure for almost every conceivable malady, and there were numerous case reports of successful treatments for snakebites, typhus, diphtheria, and other infections.
E. angustifolia became a favorite with eclectic physicians, since it was thought to be greater in activity than other species. Eclectics used it externally as a local antiseptic, stimulant, deodorant, and anesthetic, and internally for “bad blood” (i.e., to correct “fluid depravation with tendency to sepsis and malignancy”).28,29
Although many physicians began to investigate and use echinacea as a serious medicine, in 1909 the Council on Pharmacy and Chemistry of the American Medical Association refused to recognize echinacea as an active drug, stating: “In view of the lack of any scientific scrutiny of the claims made for it, Echinacea is deemed unworthy of further consideration until more reliable evidence is presented in its favor.” Despite this opposition, echinacea was included in the National Formulary of the United States and remained there until 1950.3
With the demise of the eclectic movement, the popularity of echinacea in the United States waned except among naturopathic physicians until around 1980, when it was rediscovered due to increased consumer interest in immune system disorders such as candidiasis, chronic fatigue syndrome, acquired immunodeficiency syndrome (AIDS), and cancer. Although interest in echinacea decreased in America between the 1930s and 1980s, European physicians continued research. Much of this research was initiated by a 1932 study by Gerhard Madaus, who demonstrated immune-enhancing effects of a preparation from the fresh juice of the aerial portion of E. purpurea. This was followed by development of a commercial product (Echinacin) and a great deal of scientific study. Thus, E. purpurea began to be as respected as E. angustifolia among herbal practitioners in Europe.3
 Pharmacology
Pharmacology
The chemistry, pharmacology, and clinical applications of echinacea have been the subject of more than 300 scientific studies.2,3,30 This section summarizes some of the pharmacologic information on Echinacea with attention to the species used, part of the plant used, solvent used for extraction, and other relevant features. When no species delineation is made, the activity described is similar in all species.
Tissue Regeneration and Antiinflammatory Properties
Echinacin (a commercial product consisting of the freshly pressed juice of E. purpurea stabilized in ethanol) as well as polysaccharide components of echinacea have been shown to promote tissue regeneration and reduce inflammation in experimental studies.31 This effect is apparently largely due to inhibition of the enzyme hyaluronidase via formation of a polysaccharide complex with hyaluronic acid, thereby maintaining the structure and integrity of the collagen matrix in connective tissue and ground substance. In addition to increased hyaluronic acid stabilization, echinacea also stimulates fibroblast growth and manufacture of glycosaminoglycans, a critical goal in wound healing. Echinacea exerts a mild, direct cortisone-like effect and enhances the secretion of adrenal cortex hormones.3 The polysaccharide portion appears to be responsible for the direct anti-inflammatory effects, although the alkylamide fraction has also demonstrated some activity.32
Immunostimulatory Properties
Echinacea possesses a broad spectrum of effects on the immune system as a result of its content of a diverse range of active components affecting different aspects of immune function.2,3 For example, inulin, the major component in the root of E. angustifolia, activates the alternative complement pathway and thus promotes chemotaxis of neutrophils, monocytes, and eosinophils; solubilization of immune complexes; neutralization of viruses; and bacteriolysis. Echinacea also increases the levels of properdin, the normal serum globulin that stimulates the alternative complement pathway.2,3,33 Another nonspecific immune enhancement is echinacea’s enhancement of serum leukocyte and granulocyte counts.2,3,30–34
The high-molecular-weight heteroglycan polysaccharide components of echinacea have profound immunostimulatory effects. The majority of these effects appear to be mediated by the binding of active echinacea polysaccharides to carbohydrate receptors on the cell surface of macrophages and T-lymphocytes. However, some of the T-cell activation found in early studies is now thought to be due to a contaminant protein. Later studies using a purer polysaccharide fraction did not show significant results.3
Echinacea promotes nonspecific T-cell activation (i.e., transformation, production of interferon, and secretion of lymphokines). The resultant effect is enhanced T-cell mitogenesis, macrophage phagocytosis, antibody binding, natural killer cell activity, and increased numbers of circulating neutrophils.3,30
Echinacea polysaccharides were also shown to enhance macrophage phagocytosis and to stimulate macrophages to produce increased amounts of tumor necrosis factor (TNF), interferon, and IL-1; destroy tumor cells in tissue culture; and inhibit Candida albicans infection in rats infected intravenously with a lethal dose (3 × 105 cells) of C. albicans.3,34 The interactions with macrophages were most likely responsible for much of the immune system enhancement of echinacea polysaccharides.
In addition to the polysaccharides, lipophilic alkylamides and caffeic acid derivatives like cichoric acid are thought to contribute to the immunostimulatory aspects of echinacea, especially alcoholic extracts.2,3,30 Although most research has been devoted to the water-soluble components such as polysaccharides, the lipophilic fraction yields the most potent enhancement of macrophage phagocytosis.3,4
The carbon clearance test is often used to measure systemic macrophage activation. The method involves measuring the rate of disappearance of carbon granules from the blood at varying intervals after administration of the test substance. Root extracts of echinacea administered orally tend to yield greater effects on phagocytic activity than the aerial portion, with E. purpurea greater than E. angustifolia, which is greater than E. pallida.3
Many studies used injectable preparations, but oral preparations are generally thought to yield similar or even better results, although direct comparisons are apparently not available. For example, intramuscular Echinacin administered to healthy males on 4 successive days was shown to increase granulocytic phagocytosis by nearly 50%, whereas the oral administration of an E. purpurea root extract at a dose of 30 drops three times a day to healthy males for 5 consecutive days resulted in an increase of 120%.3 However, this difference might be due to the differing constituents of the forms used. The expressed juice of the aerial portion E. purpurea, as found in Echinacin, has lower concentrations of several of the phagocytosis-stimulating compounds characteristic to echinacea, including polysaccharides, alkylamides, and caffeic acid derivatives like cichoric acid compared with alcoholic extract.3
In general, echinacea appears to offer benefits for all infectious conditions. An exception to this statement may be AIDS. It is unclear at this time if echinacea should be recommended for AIDS. Although this condition is associated with widespread depression of the immune system, presumably due to the human immunodeficiency virus, stimulation of T-cell replication may also stimulate replication of the virus as well. In addition, echinacea was shown to lower T-helper cells and decrease T-helper cell–to–suppressor cell ratios.2,3 Although there are anecdotal reports of echinacea’s efficacy in human immunodeficiency virus-infected individuals, more research is necessary.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


