Distal Radius Fractures: Open Reduction Internal Fixation
Distal Radius Fractures: Open Reduction Internal Fixation
Andrea S. Bauer
Jesse B. Jupiter
INTRODUCTION
Recent epidemiological studies show that the operative treatment of distal radius fractures continues to increase. Koval et al. (1) reviewed the cases submitted by candidates for Part II of the American Board of Orthopaedic Surgery and found that the proportion of distal radial fractures treated with open surgical treatment had increased from 42% in 1999 to 81% in 2007. Some of this increase is related to the large number of internal fixation devices now available in the marketplace, which is heavily promoted. These commercially available volar locked plates are specifically designed for fixation of distal radius fractures (Fig. 14.1). Additionally, the advent of locking plate technology allows improved fixation in osteoporotic bone when compared to conventional plating and has led to increased use in elderly patients (2).
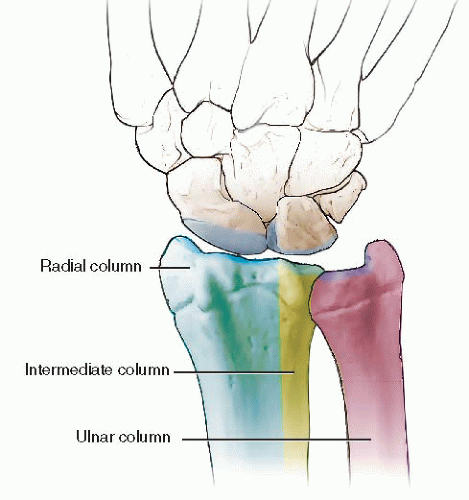
While advances in technology have facilitated internal fixation of the distal radius, the surgeon must still be aware of the structure and biomechanics of the distal radius. The column theory of the distal radius, as described by Rikli and Regazzoni in 1996, continues to be a useful guide in understanding and treating distal radius fractures (3) (Fig. 14.2). The radial column consists of the radial styloid and the scaphoid facet of the distal radius. This area serves to buttress the carpus radially and is the origin of important intracarpal stabilizing ligaments. The intermediate column consists of the lunate facet of the distal radius as well as the sigmoid notch and functions in load transmission from the carpus to the distal radius. The entire distal ulna and triangular fibrocartilage complex is considered the ulnar column, which stabilizes the distal radioulnar joint (DRUJ) as well as the ulnar carpus. Whether or not “fragment-specific” implants are used, it is important to understand the roles of each column in restoring anatomy and biomechanics of the distal radius.
INDICATIONS AND CONTRAINDICATIONS
The decision for operative fixation of a distal radius fracture is based on a combination of fracture and patientspecific factors. The type of fracture, associated soft-tissue and neurovascular injuries, associated fractures (of the ipsilateral limb or distant sites), and the overall medical condition of the patient must all be taken into account. However, with the advent of fixed-angle locking screw-plate constructs, underlying osteopenia is no longer a contraindication to internal fixation.
Definite Indications for ORIF
Some fracture patterns are inherently unstable, such as those involving dislocation or subluxation of the radiocarpal joint, and require open reduction internal fixation (ORIF) to restore stability. Other fracture patterns, such as articular fractures with a displaced, rotated lunate facet fragment, cannot be reduced by closed maneuvers and require ORIF. Finally, fractures with unacceptable amounts of displacement that present 3 weeks or more after injury can rarely be reduced closed and require ORIF (Table 14.1).
FIGURE 14.1 A few of the many implants constructed specifically for the volar distal radius.
Relative Indications
Many factors specific to the fracture type and the patient are relative indications for ORIF of the distal radius. These include bilateral displaced fractures, fractures associated with ipsilateral limb trauma or in the setting of a polytrauma, some fractures with associated progressive swelling or nerve dysfunction, open fractures, fractures associated with DRUJ instability, and unstable fractures not reduced after closed reduction and cast immobilization (Table 14.2). There are several agreed-upon radiographic indications of fracture instability (4, 5 and 6). These include dorsal comminution >50% of the width on a lateral radiograph, any palmar metaphyseal comminution, initial dorsal tilt >20 degrees, initial fragment translation >1 cm, initial radial shortening >5 cm, intra-articular disruption, associated ulna fracture, and severe osteoporosis (Table 14.3).
Relative Contraindications
Patients with medical conditions that prohibit the use of anesthesia, with poor compliance, or with local softtissue problems, such as active infection or complex regional pain syndrome, may not benefit from internal fixation of their fracture (Table 14.4). Additionally, low-demand elderly patients with fracture displacement but good alignment of the carpus on the forearm may not achieve functional improvement with ORIF, despite radiographic improvement (7). The surgeon must keep in mind that anticipated functional loading, rather than chronological age, should be used to guide treatment decisions.
FIGURE 14.2 The column theory of the distal radius.
TABLE 14.1 Definite Indications for ORIF
Radiocarpal subluxation or dislocation
Displaced fracture of the radial styloid
Rotated fracture of the volar lunate facet
Displaced intra-articular fractures seen late (after 3 wk)
TABLE 14.2 Relative Indications for ORIF
Bilateral displaced fractures
Fractures associated with ipsilateral limb trauma
Fractures in the setting of polytrauma
Fractures associated with excessive swelling or nerve dysfunction
Open fractures
Fractures associated with DRUJ instability
Unstable fractures that failed cast immobilization
TABLE 14.3 Radiographic Signs of Instability
Dorsal comminution >50%
Palmar metaphyseal comminution
Dorsal tilt >20 degrees
Fragment translation >1 cm
Radial shortening >5 cm
Intra-articular disruption
Associated ulna fracture
Severe osteoporosis
TABLE 14.4 Relative Contraindications to ORIF
Patients with medical conditions that prohibit anesthesia use
Poor patient compliance
Poor local soft-tissue conditions or complex regional pain syndrome
PREOPERATIVE PLANNING
As with any musculoskeletal injury, a careful evaluation of the patient’s overall condition, as well as that of the involved limb and hand, must be made before a decision is rendered to proceed with operative intervention. The fracture characteristics are not always easily appreciated before the fracture is reduced and repeat x-rays are taken. Furthermore, additional x-ray views, including oblique views that focus on the articular surface or computed tomography (CT) scanning, may further influence the decision about treatment (8).
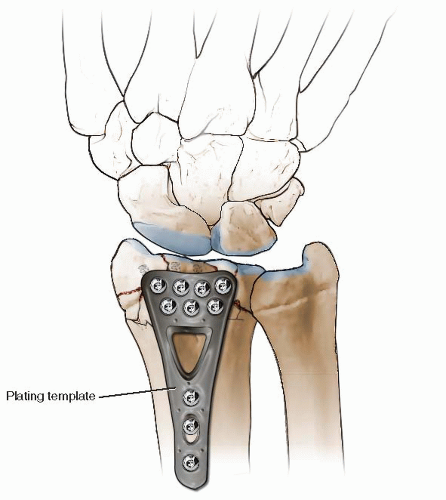
A thorough evaluation of the imaging studies preoperatively helps in determining which reduction maneuvers may be necessary, and whether fixation of the fracture will require a special exposure or additional equipment. For particularly complex fractures, a preoperative template may be useful (Fig. 14.3).
When the fracture involves impacted articular fragments and/or extensive metaphyseal comminution, the potential for autogenous, allogeneic, or bone-substitute grafts should be noted in the preoperative plan. In these cases, the patient should also be informed that bone grafting may be necessary.
OPERATIVE TECHNIQUES
ORIF of the distal radius is generally performed as outpatient surgery with regional anesthesia, pneumatic tourniquet control, and the involved limb extended on a hand table. A parenteral antibiotic, usually cefazolin, is given at least 30 minutes prior to incision as prophylaxis against surgical site infection. A surgeon-operated mini-C-arm fluoroscopy unit is used throughout the procedure to confirm fracture reduction and hardware placement. Distal radius fractures may be operatively approached through several different exposures, which will be highlighted here with emphasis on the pearls and pitfalls of each.
Volar Approach
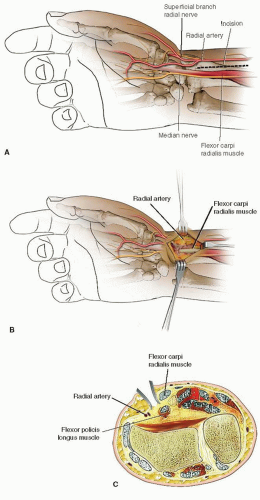
The uncomplicated volar shearing, as well as the extra-articular, volar-displaced Smith’s, and many dorsally displaced fractures may be approached through the modified Henry approach to the distal radius (Fig. 14.4). An advantage of a volar approach is the surgeon’s ability to judge rotational alignment as well as length by reducing the volar cortical fracture lines as this area is not usually comminuted even in impacted, dorsally displaced fractures. The modified Henry approach exploits the interval between the radial artery and the flexor carpi radialis (FCR). The incision is marked out directly over the FCR, which is almost always palpable, beginning approximately 5 cm proximal to the distal wrist crease.
FIGURE 14.3 Preoperative template for ORIF of a distal radius fracture.
FIGURE 14.4A-C. Volar modified Henry approach to the distal radius.
Only gold members can continue reading. Log In or Register to continue

 Intra-Articular Fractures of the Distal Humerus: Total Elbow Arthroplasty
Intra-Articular Fractures of the Distal Humerus: Total Elbow Arthroplasty



