Distal Radio-Ulnar Joint Capsulectomy for Post-Traumatic Limitation of Forearm Rotation
William B. Kleinman
Reduced forearm pronosupination following trauma can have a profound, often devastating effect on upper extremity function. Of the four major joints of the upper extremity, the rotating forearm contributes most significantly to our ability to put or place our hand in space in order to maximize hand function (Fig. 36-1A, B). Forearm rotation is a complex activity that relies on integrated motion at the radiocapitellar and proximal radio-ulnar joints of the elbow, the mid-forearm interosseous ligament (IOL), and the distal radio-ulnar joint (DRUJ) at the wrist (Fig. 36-2). The longitudinal forearm axis-of-rotation passes through the center of the proximal radial head, along the forearm, exiting at the fovea of the distal ulna, at the base of the ulna styloid (Fig. 36-3). The ulnotrochlear joint of the elbow is a pure ginglymus (hinged) joint; it does not contribute at all to forearm rotation. Radius, carpus, and hand rotate as a unit around the longitudinal forearm axis-of-rotation from full supination, where the radius and the ulna are essentially parallel, to full pronation, where the radius–carpus–hand unit crosses the fixed ulna (Fig. 36-4). Normal biomechanics of full forearm pronosupination require not only rotation of the radius–carpus–hand unit around this longitudinal forearm axis-of-rotation, but translation of the sigmoid notch of the radius across the articular seat of the distal ulna. Figure 36-5 demonstrates the tracking line of the principal axis of load-bearing* through the full arc of pronosupination at the sigmoid notch (the distal cadaver ulna has been rotated out of the field for visibility of the notch). The obliquity of this load-bearing tracking line represents the relative shortening the radius undergoes as the radius–carpus–hand unit crosses the ulna from supination to pronation. Stability of the DRUJ through its normal 180-degree arc of forearm pronosupination is provided primarily by the complex check-rein components of the triangular fibrocartilage (TFC). The deep volar and dorsal components of the TFC (ligamentum subcruentum) (1) are principally responsible for stabilizing the radius–carpus–hand unit as it rotates and translates around the seat of the distal ulna (Fig. 36-6). The origin of the ligamentum subcruentum is at the fovea of the ulna; its two insertions are at the volar and dorsal aspect of the medial distal radius, distal to the sigmoid notch
(Fig. 36-7A, B). The well-vascularized superficial radio-ulnar ligaments of the TFC form a basket around the hypovascular central articular disc (Fig. 36-8).
(Fig. 36-7A, B). The well-vascularized superficial radio-ulnar ligaments of the TFC form a basket around the hypovascular central articular disc (Fig. 36-8).
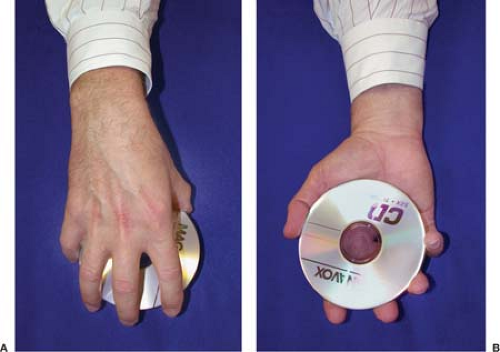 Figure 36-1 Rotation of the forearm is critical for putting or placing the hand in space for maximal function. |
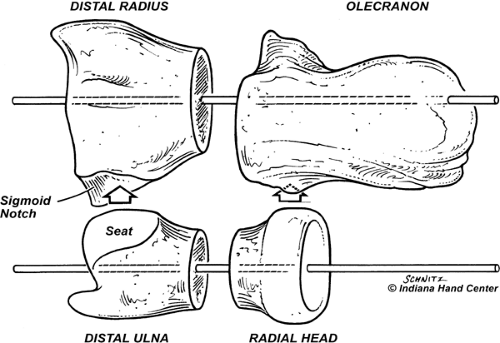 Figure 36-2 Forearm rotation takes place at two joints: (1) the distal radio-ulnar joint (DRUJ); and (2) the proximal radio-ulnar joint (PRUJ). Pronosupination can be conceptualized at both joints by thinking of the forearm as a bicondylar diarthrodial joint. Removing the long diaphyses of radius and ulna from the image places the DRUJ and PRUJ together as a flexing and extending glinglymuslike joint. |
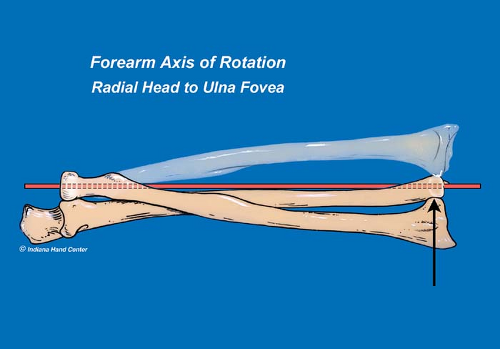 Figure 36-3 The longitudinal mechanical axis of the forearm extends from the fovea at the base of the ulna styloid distally, through the radial head proximally. The stable ulna is held securely at the ulnotrochlear joint of the elbow. The hand–carpus–radius unit rotates around the fixed ulna to generate a full 180-degree arc of normal pronosupination. |
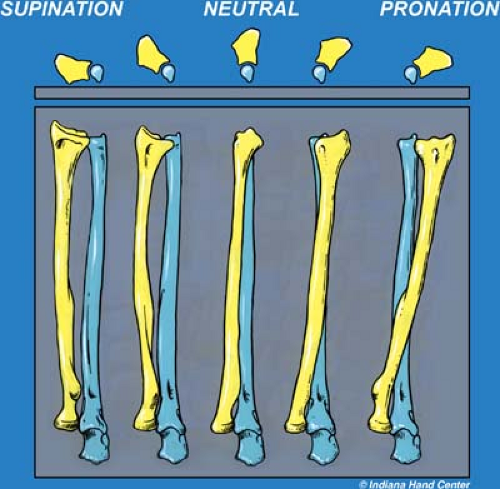 Figure 36-4 As the radius rotates and translates from full supination to full pronation around a fixed ulna, the radiocarpal unit shortens relative to the ulna, resulting in ulna-plus variance in the pronated position. |
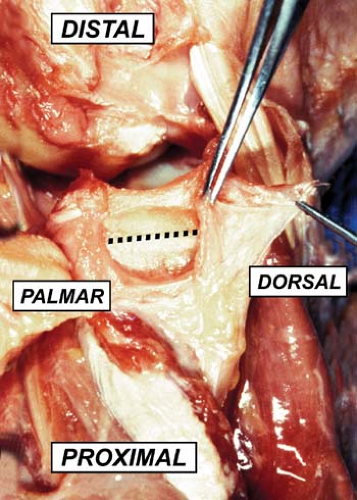 Figure 36-5 The principal axis of load-bearing tracks across the sigmoid notch from proximal/palmar in supination to distal/dorsal in pronation. |
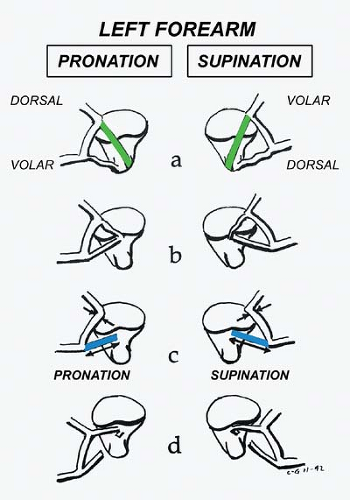 Figure 36-6 The superficial portion of the triangular fibrocartilage (TFC) inserts directly into the ulna styloid. The palmar portion tightens with forearm pronation; the dorsal portion tightens in supination. The deep portion of the TFC (ligamentum subcruentum) inserts in the fovea, just medial to the ulna pole. The palmar fibers of this deep portion tighten in pronation, and the dorsal fibers tighten in supination. (From Hagert CG. Distal radius fracture and the distal radio-ulnar joint-anatomical considerations. Handchir Mikrochir Plast Chir 26:22–26, 1994, With permission.) |
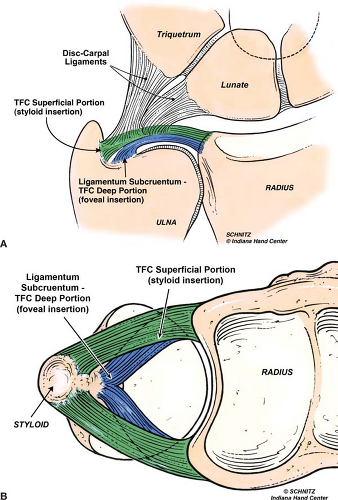 Figure 36-7 A: The triangular fibrocartilage (TFC) supporting the distal radio-ulnar joint (DRUJ) has two distinct insertions on the ulna. The deep portion (blue) is referred to as the ligamentum subcurentum, which inserts into the fovea, just medial to the articular surface of the ulna pole. The superficial portion (green) inserts directly onto the base of the ulna styloid. These two independent insertions allow different components of the TFC to tighten in different positions of forearm rotation. B: The angles-of-attack of these two components of the TFC are quite different, making the deep, blue fibers (ligamentum subcruentum) considerably more effective as a DRUJ stabilizer through the full arc of forearm pronosupination. |
The superficial radio-ulnar ligaments are relatively minor stabilizers of the DRUJ, because full pronation places the radius too volar relative to the entire ulna seat for the dorsal superficial radio-ulnar ligament to be mechanically effective as a DRUJ stabilizer. Conversely, full supination places the radius too far dorsal relative to the entire ulna seat for the volar superficial radio-ulnar ligaments to be effective (1,2) (Fig. 36-6). The articular disc (white; Fig. 36-8) is principally responsible for load transfer from the hand to the forearm through the ulnar side of the wrist, when the hand–forearm unit is ulnar deviated (Fig. 36-9A, B).
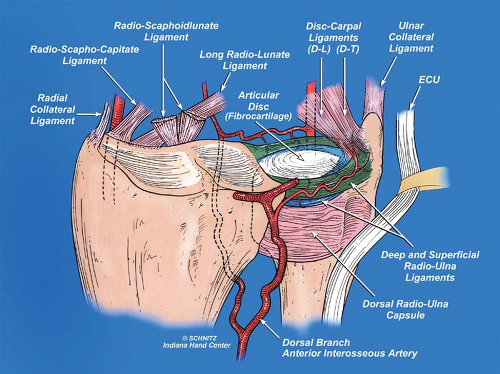 Figure 36-8 The primary intrinsic stabilizer of the distal radio-ulnar joint (DRUJ) relationship is the triangular fibrocartilage (TFC) complex. This tissue consists of a central avascular atricular disc or centrum, disc-carpal ligaments, vascularized palmar and dorsal limbi (the radio-ulnar ligaments), and the ulnocarpal meniscus homologue. The deep subsheath of the extensor carpi ulnaris (ECU) (the independent fibrosseous canal of the sixth dorsal compartment) is blended intimately with the TFC at its dorsal margin (the subsheath of the ECU is not represented in this diagram). |
It is important to recognize that, although four extrinsic factors have been described as contributing to the stability of the DRUJ (extensor carpi ulnaris [ECU] tendon; ECU retinacular subsheath [VIth dorsal compartment], pronator quadratus [PQ] muscle, and interosseous ligament), the intrinsic components of the TFC bear the major responsibility for physiologic DRUJ stability (Figs. 36-6, 36-7 and 36-8). The entire DRUJ complex is biomechanically similar to any other diarthrodial joint in the human body. Two articular surfaces are joined for movement under load. Each opposing surface is covered by hyaline cartilage. The joint is surrounded 360 degrees by a capsule, the thickened parts of which form ligaments that guide motion between the two articular surfaces. The cartilage is nourished by synovial fluid. At the DRUJ, the TFC is the critical ligament complex guiding the radio-ulnar relationship through a physiologic arc of pronosupination. Vesely in 1967 gave the portion of the capsule other than the TFC the confusing name “volar and dorsal radio-ulnar ligaments,” implying that this remainder tissue represented some stabilizing component of the DRUJ capsule (3,4). More recently, details of the anatomy of the DRUJ capsule were investigated in our cadaver laboratory by my former hand surgery fellow, Dr. Thomas Graham, and me. Our findings were published in 1998, in the American Journal of Hand Surgery (3,5) (Figs. 36-10 and 36-11). Through our work in the lab, it became clear that, although the dorsal and volar DRUJ capsular components are anatomically distinct, neither of them plays a supportive role in DRUJ mechanics. Only the TFC and its various components are responsible for normal DRUJ stability.
Through a prospective clinical trial based on our newly acquired knowledge of the DRUJ capsule, we hypothesized that—as in all diarthrodial joints—normal elasticity of the DRUJ diarthrodial capsule could be clinically compromised by hemorrhage, exudate, and scarring associated with trauma to the wrist, especially with the magnitude of injury associated with fracture of the distal radius. It also became clear to us that chronic, post-traumatic stiffness of the forearm, following either closed manipulation or surgical intervention for displaced distal radius fractures, might be
directly attributable to trauma-induced contracture of the dorsal or volar capsules of the distal radio-ulnar joint. Forearm stiffness could be a consequence of prolonged immobilization or limited range-of-motion following injury.
directly attributable to trauma-induced contracture of the dorsal or volar capsules of the distal radio-ulnar joint. Forearm stiffness could be a consequence of prolonged immobilization or limited range-of-motion following injury.
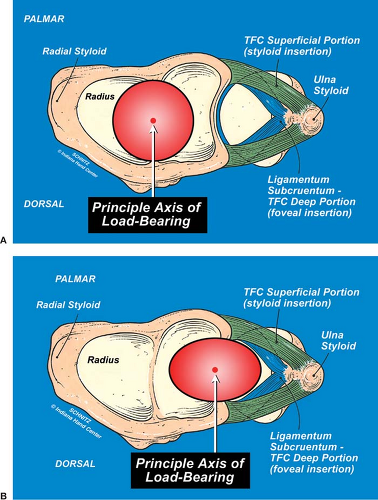 Figure 36-9 The prime intrinsic stabilizer of the distal radio-ulnar joint is the triangular fibrocartilage (TFC). The TFC complex consists of superficial (green) and deep (blue) radio-ulnar fibers. The articular disc is responsible for transferring load from the medial carpus to the pole of the distal ulna. The vascularized, peripheral radio-ulnar ligaments (green and blue) are nourished by dorsal and palmar branches of the posterior interosseous artery and are responsible for guiding the radiocarpal unit around the seat of the ulna. A: The deep radio-ulnar fibers of the TFC (dorsal and palmar) originate at the dorsal and palmar edges of the medial border of the distal radius, and insert onto the fovea of the ulna (blue fibers, referred to as the ligamentum subcurentum). Their obtuse angle-of-attack makes them particularly effective in guiding the radius around the ulna through a functional arc of pronosupination. In compressive mode, with the hand–forearm unit in neutral deviation, the principal axis of load-bearing passes through the scapholunate ligament onto the articular surface of the distal radius. B: Deep fibers of the TFC (ligamentum subcruentum) insert onto the ulna fovea at an obtuse angle-of-attack (blue). Superficial radio-ulnar fibers (green) insert onto the ulna styloid and have little function in controlling forearm rotation at the distal radio-ulnar joint. As the principal axis of load-bearing shifts onto the TFC in ulnar deviation, the articular disc is supported by the superficial palmar and dorsal (green) radio-ulnar ligaments, attaching directly to the bony ulna styloid. |
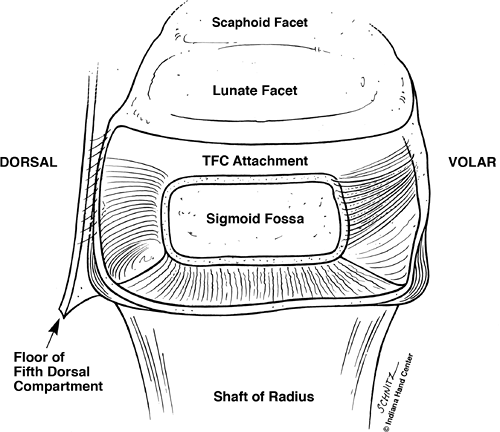 Figure 36-10 Representative diagram of cadaver findings. The distal radio-ulnar joint (DRUJ) capsule has palmar, dorsal, and proximal components. In conjunction with the triangular fibrocartilage (TFC), it completely envelopes the seat and pole of the distal ulna. The palmar and dorsal components in their native state are capacious, and allow the ulna pole to translate and rotate into redundant palmar tissue in supination, and into the redundant dorsal tissue in pronation. |
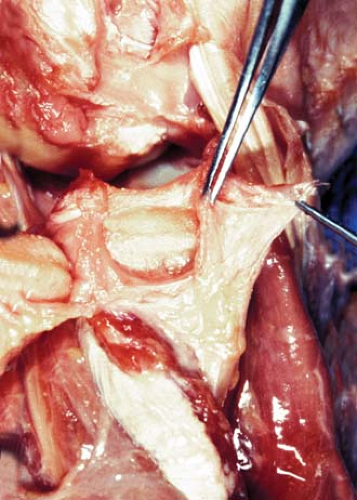 Figure 36-11 The viewer is looking directly at the radius sigmoid notch. The ulna has been rotated out of the field to the viewer’s left. The distal radio-ulnar joint (DRUJ) capsule completely envelopes the joint. In this specimen, the dorsal component is reflected to the viewer’s right by a forceps and skin hook. The volar component tethers the distal ulna, to the viewer’s left. The triangular fibrocartilage (TFC) has been removed from its origin distal to the sigmoid notch. |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


