Arthroscopic Repair of the Triangular Fibrocartilage Complex (TFCC)
Randall W. Culp
Sam J. Biafora
Indications
Triangular fibrocartilage complex (TFCC) injury is a frequent cause of ulnar-sided wrist pain. On presentation, the patient may recall a recent fall on an outstretched hand. These traumatic injuries tend to result from the application of an extension–pronation force to the axially loaded wrist. Alternatively, the patient may complain of long-standing ulnar-sided pain of insidious onset without a known traumatic event. This scenario should raise suspicion for a more chronic, degenerative process. The classification system described by Palmer (1) distinguishes between traumatic and degenerative TFCC injuries. We focus on the treatment of traumatic TFCC lesions in this chapter.
The classification distinguishes between class I (traumatic) and class II (degenerative) lesions (Table 31-1). Traumatic lesions are categorized according to their location. Degenerative lesions involve the central portion of the disk. The classification of degenerative lesions follows a progression related to increasing repetitive loading of the TFCC as a result of ulnar impaction. A spectrum of injuries to surrounding structures is identified. We will focus on the traumatic lesions of the TFCC. A class IA lesion is a perforation in the central portion of the TFCC. It is usually located 2 to 3 mm medial to the TFCC’s radial attachment. A flap of cartilage may be attached to the medial border. Class IB lesions represent an avulsion of the TFCC from its insertion into the distal ulna or a fracture of the ulnar styloid base. This injury may also be associated with distal radioulnar joint (DRUJ) instability. Class IC lesions represent an avulsion of the ulnocarpal portion (ulnolunate and ulnotriquetral ligaments) of the TFCC from the ulnar carpus. This may result in ulnar carpal instability with palmar translocation of the carpus. A class ID lesion is a detachment of the TFCC from the radius (Fig. 31-1).
The TFCC is composed of the triangular fibrocartilage proper (the articular disk), the meniscus homologue (the ulnocarpal meniscus), the ulnar collateral ligament, the dorsal radioulnar ligament, the volar radioulnar ligament and the subsheath of the extensor carpi ulnaris tendon (ECU) (2). Injury to one or a combination of these structures can lead to instability and pain. The TFCC functions as a stabilizer of the DRUJ and the ulnar carpus and as a load-bearing cushion for the transmission of axial loads between the ulnar carpus and the forearm unit (3). Biomechanical analysis of the DRUJ has revealed that the distal ulna, through its articulation with the medial carpus via the TFCC, carries approximately 20% of the axial load of the forearm (4). The thickness of the articular disk portion of the TFCC varies inversely with positive ulnar variance (3). Histologic studies reveal the more central articular disc to contain interweaving obliquely oriented sheets of collagen fibers, whereas parallel, longitudinally oriented collagen fibers are found in the periphery (5). The vascular anatomy of the TFCC has also been investigated. Thiru-Pathi et al. (6) found that small vessels supply the outer 15% to 20%. Bednar et al. (7) found vascular
penetration into the periphery ranging from 10% to 40% of the width of the TFCC (Fig. 31-2). Both studies found the central and radial portions to be avascular. This is of clinical significance, suggesting that peripheral tears may be able to illicit the appropriate reparative response to render it amenable to repair.
penetration into the periphery ranging from 10% to 40% of the width of the TFCC (Fig. 31-2). Both studies found the central and radial portions to be avascular. This is of clinical significance, suggesting that peripheral tears may be able to illicit the appropriate reparative response to render it amenable to repair.
Table 31-1. Classification of Triangular Fibrocartilage Complex Lesions | ||
|---|---|---|
|
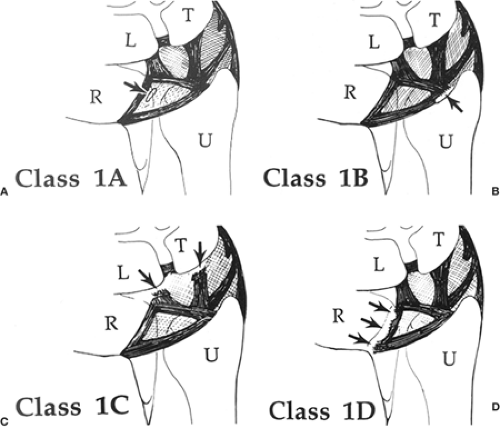 Figure 31-1 Palmer classification of traumatic triangular fibrocartilage complex (TFCC) lesions. A: Tear of the horizontal portion of TFCC, 2 to 3 mm medial to radial attachment of TFCC. B: Traumatic avulsion of the TFCC from its insertion into the distal ulna. The TFCC may alternatively be avulsed from the distal ulnar by a fracture of the base of the ulnar styloid. C: Avulsion of the TFCC from its distal attachment to the lunate and triquetrum. D: Traumatic avulsion of the TFCC from its attachment onto the sigmoid notch of the distal radius. (From: Palmer AK. Triangular fibrocartilage complex lesions: a classification. J Hand Surg 14A:594–606, 1989, with permission.) |
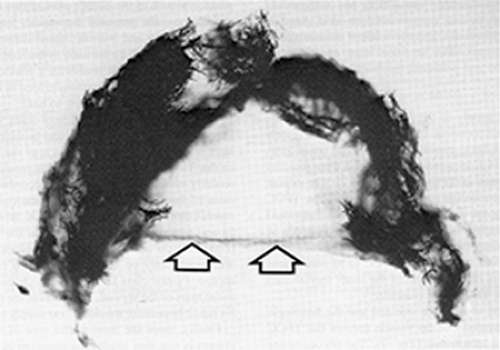 Figure 31-2 Axial view of the triangular fibrocartilage complex (TFCC) after vascular perfusion and tissue clearing. Central portion and radial attachment (arrows) without vascular penetration. (From: Bednar MS, Arnoczky SP, Weiland AJ. The microvasculature of the triangular fibrocartilage complex: its clinical significance. J Hand Surg [Am] 16A:1101–1105, 1991, with permission.) |
Arthroscopic evaluation and attempted repair of a TFCC tear is indicated when symptoms of pain on the ulnar side of the wrist have failed conservative, nonoperative measures. The initial treatment of most TFCC tears should include a trial of immobilization. Take care to assure that no other associated findings (e.g., DRUJ instability or ECU subluxation) are present. If routine radiographs and physical examination rule out other significant findings, we recommend immobilization for 4 weeks. A peripheral tear has substantial healing potential because of its good blood supply. Those with central tears may be treated in similar fashion; although the healing potential is poor, they may become asymptomatic. Arthroscopic evaluation for TFCC tear is indicated when 3 to 4 months of nonoperative treatment modalities have failed to provide sufficient relief of symptoms.
Contraindications
A TFCC tear is only one diagnosis in a long list of differentials of ulnar-sided wrist pain (8). Although wrist arthroscopy can be used to diagnose this particular etiology of wrist pain, other causes may coexist and must, therefore, be ruled out to provide the optimal environment for a successful arthroscopic TFCC repair. A peripheral TFCC tear can be associated with significant DRUJ instability. In this instance, an open anatomic repair using transosseous sutures through the fovea is indicated. Arthroscopic repair of a central TFCC tear is also contraindicated. Its avascular nature provides for poor healing potential. Repair of radial sided TFCC tears is controversial for similar reasons. Tendinitis or subluxation of the ECU may coexist with a TFCC lesion because of its anatomic relationship. Failure to address an injury to the ECU subsheath will yield a poor outcome. Although ulnar-positive variance is more commonly associated with degenerative type tears, it may also be apparent in a peripheral tear. Arthroscopic repair of a TFCC tear in a patient with ulnar-positive variance who requires repetitive weight-bearing across the wrist and ulnar deviation activities during daily activities may also yield a poor result.
Preoperative Preparations
Patients presenting with acute TFCC injuries will complain of pain and occasionally clicking on the ulnar side of the wrist. Symptoms are typically exacerbated with daily activities that involve ulnar deviation of the wrist, twisting maneuvers, and axial traction or weight bearing. Power grip may
also aggravate symptoms. Depending on the acuity of the injury, physical examination will reveal swelling on the ulnar side of the wrist and point tenderness over the TFCC or distal ulnar. Focal tenderness will frequently be localized between the ECU and flexor carpi ulnaris (FCU) distal to the ulnar styloid. Alternatively, pain can be diffusely distributed over the ulnar side of the wrist, with inability to localize focal tenderness. Axial load with simultaneous rotation on the ulnarly deviated wrist (TFCC compression test) is a provocative maneuver that is positive when a painful response is elicited. A painful click may also be apparent. It is also important to assess for DRUJ instability. Significant instability indicates involvement of the radioulnar ligaments, which precludes arthroscopic TFCC repair. Examine the ulnar carpus for a supination or palmar sag deformity, which would suggest a more significant ligamentous injury. A peripheral TFCC tear may also be associated with disruption of the ECU subsheath. Accordingly, ECU subluxation must also be excluded.
also aggravate symptoms. Depending on the acuity of the injury, physical examination will reveal swelling on the ulnar side of the wrist and point tenderness over the TFCC or distal ulnar. Focal tenderness will frequently be localized between the ECU and flexor carpi ulnaris (FCU) distal to the ulnar styloid. Alternatively, pain can be diffusely distributed over the ulnar side of the wrist, with inability to localize focal tenderness. Axial load with simultaneous rotation on the ulnarly deviated wrist (TFCC compression test) is a provocative maneuver that is positive when a painful response is elicited. A painful click may also be apparent. It is also important to assess for DRUJ instability. Significant instability indicates involvement of the radioulnar ligaments, which precludes arthroscopic TFCC repair. Examine the ulnar carpus for a supination or palmar sag deformity, which would suggest a more significant ligamentous injury. A peripheral TFCC tear may also be associated with disruption of the ECU subsheath. Accordingly, ECU subluxation must also be excluded.
Imaging studies should include plain radiographs with neutral rotation posteroanterior (PA) and lateral views. Dynamic changes in ulnar variance may be seen with a pronated, clenched-fist PA view of the wrist. Abnormal findings, such as ulnar styloid fracture, DRUJ arthritis, DRUJ widening, and ulnar-positive variance may change the treatment algorithm.
Wrist arthrography may be helpful in isolating intercarpal ligament or TFCC tears. When wrist arthrography is performed, the triple injection technique is recommended. This method helps to ensure that one-way flaps are not missed. Introduce the first injection of the contrast material into the radiocarpal joint. Observe the flow of the dye during the early flow phase to assure there is no leakage into the midcarpal joint and DRUJ. Once adequate time has passed to allow for the absorption of the contrast from the first injection, inject the contrast material into the midcarpal joint and the DRUJ. Weiss et al. (9) compared the results of triple injection cinearthrography with arthroscopy. The sensitivity, specificity, and accuracy in detecting tears of the TFCC were 60%, 100%, and 76%, respectively. Essentially, normal arthrographic findings did not rule out the possibility of a TFCC tear. As the comfort level of wrist arthroscopy continues to grow and the accessibility of high-resolution magnetic resonance imaging (MRI) increases, the clinical application of wrist arthrography will remain controversial.
Computed tomography (CT) has a limited role in diagnosis of a TFCC tear. Although it is not useful in identifying a tear, it may assist in cases where the stability of the DRUJ is in question. It should be performed in supination, neutral, and pronation to assess for DRUJ incongruency. Evaluate both wrists in identical rotation in these cases.
The most commonly used imaging study for TFCC tear has become MRI. The image of greatest diagnostic importance is a T2-weighted image in the coronal plane. Its appearance is similar to that of an arthrogram in that the synovial fluid appears bright and may outline the tear in the TFCC. The addition of a wrist coil has improved the reliability of its results. Studies comparing MRI and wrist arthrography have revealed varying results. Morley et al. (10) reviewed MRIs performed using 1.5 Tesla scanner without a wrist coil. They found 44% sensitivity for detection of TFCC tear. Using a 1.5 Tesla magnet with wrist coil, Potter et al. (11) reported 100% sensitivity, 90% specificity, and 97% accuracy for the detection of TFCC tear. The use of high-resolution MRI in the detection of TFCC tears appears to yield more reliable results.
Arthroscopy remains the gold standard for the identification of a tear in the TFCC. It can assess for size, stability, and location of the tear. A complete diagnostic wrist arthroscopy, which would include midcarpal arthroscopy, should be performed so that other associated findings may be addressed. These findings may include synovitis, lunate chondromalacia, lunotriquetral tear, ulnar extrinsic ligament tear, or proximal hamate chondromalacia. These findings may indicate the need for additional procedures.
Technique
Under regional or general anesthesia, with the patient in the supine position, place a well-padded pneumatic tourniquet on the arm proximally. The tourniquet may be inflated during the procedure if excessive bleeding obscures optimal visualization.
Use this time to examine the wrist for instability of the DRUJ and the ulnar side of the wrist.
Make note of any crepitus or abnormal clicking.
Appropriately prepare and drape the arm.
Place finger traps over the index and long fingers.
Using a standard arthroscopic traction device, pad and secure the arm to provide for countertraction force and then place the wrist in about 5.4 kg (12 lb) of traction.
Begin initial evaluation with placement of the 2.3-mm arthroscope through the 3-4 portal.
Inspect the integrity of the radial side of the radiocarpal joint systematically and note abnormalities. Synovitis may be evident in more acute TFCC lesions, as the arthroscope is directed ulnarly.Related posts:
 Closed Reduction and Percutaneous Pinning
Intrafocal Pinning with “Arum” Pins
Ligamentous Repair for Acute Scapholunate Dissociation
Operative Reconstruction of the Distal Radioulnar Joint
Distal Radio-Ulnar Joint Capsulectomy for Post-Traumatic Limitation of Forearm Rotation
Release of the First Dorsal Compartment
Closed Reduction and Percutaneous Pinning
Intrafocal Pinning with “Arum” Pins
Ligamentous Repair for Acute Scapholunate Dissociation
Operative Reconstruction of the Distal Radioulnar Joint
Distal Radio-Ulnar Joint Capsulectomy for Post-Traumatic Limitation of Forearm Rotation
Release of the First Dorsal Compartment

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


