Distal Femoral Osteotomy
Eugenio Savarese
Bryce Bederka
Annunziato Amendola
INDICATIONS/CONTRAINDICATIONS
Limb alignment plays a critical role in the development of arthritis and overload syndromes. An osteotomy involves opening or removing a wedge of bone to alter the mechanical axis of that bone in an effort to reduce overloaded areas of a joint surface. Osteotomy about the knee surgically reshapes bone, realigning the mechanical axis of the limb away from the affected compartment. This strategy has the distinct advantage of joint preservation that may be particularly attractive for younger and more active patients with unicompartmental arthritis. Varus malalignment is most commonly corrected with a high tibial osteotomy. In contrast, valgus malalignment is most commonly corrected with a supracondylar femoral osteotomy, using either an opening- or closing-wedge osteotomy (1). Small valgus correction may be carried out with a tibial osteotomy as well, but larger corrections will lead to significant obliquity in the joint line if performed through the proximal tibia.
Distal femoral osteotomy is indicated in:
moderate corrections up to 17.5 degrees for opening wedge (2)
larger corrections from 12 degrees to 27 degrees for closing wedge (3)
mild-to-moderate osteoarthritis (OA) (2)
lateral condyle cartilage lesions (with or without cartilage grafting) (2)
lateral meniscal transplants (2)
individuals younger than 65 years
Distal femoral osteotomy is contraindicated in:
extreme valgus deformity associated with a fixed subluxation of the tibia (4)
severe medial compartment OA (3)
severe tricompartmental OA (3)
severe patellofemoral osteoarthritis (4) (relative contraindication)
inflammatory disease (1)
severe osteoporosis (5)
high body mass index (4) (relative)
individuals older than 65 years (relative)
PREOPERATIVE PLANNING
The standard evaluation begins with assessing the extent of knee arthrosis and lower extremity alignment. Standard radiographic assessment includes bilateral weight-bearing anteroposterior views in full extension, bilateral weight-bearing posteroanterior tunnel views at 30 degrees of flexion, lateral, and skyline views, and a bilateral full-length standing alignment film (Fig. 28-1). The most common deformity seen in the valgus knee is located in the femur. The normal lateral distal femoral angle is 84 degrees, with angles less than that being considered abnormal (Fig. 28-2). Magnetic resonance imaging is useful in the preoperative assessment when significant intra-articular chondral or meniscal pathology is suspected based on history or exam with mechanical findings (4).
 FIGURE 28-1 Standard radiographic assessment of the knee. (A) Standing anteroposterior. (B) Standing posteroanterior in 30 degrees of knee flexion. (C) Merchant. (D) Lateral. (E) Bilateral standing long-leg anteroposterior view from hip to ankle. |
 FIGURE 28-2 The lateral distal femoral angle is the acute angle between a line drawn down the femoral shaft and a line drawn across the femoral condyles. The normal angle is 84 degrees, with smaller angles associated with a valgus deformity. In this case, the angle measures 77 degrees. |
The required correction is calculated according to the method described by Dugdale at al (6). The osteotomy is planned so that it will place the weight-bearing line (center of the femoral head to the center of the tibiotalar joint) to fall at a selected position approximately through the tip of the medial tibial spine (Fig. 28-3). In case of significant medial joint line opening on weight-bearing radiographs, the total amount of correction should be measured from a supine or a varus stress radiograph
to take out the deformity from ligamentous laxity, which would be corrected by soft tissue reconstruction. Overcorrection to varus is absolutely contraindicated if an optimal long-term result is to be gained (2,4).
to take out the deformity from ligamentous laxity, which would be corrected by soft tissue reconstruction. Overcorrection to varus is absolutely contraindicated if an optimal long-term result is to be gained (2,4).
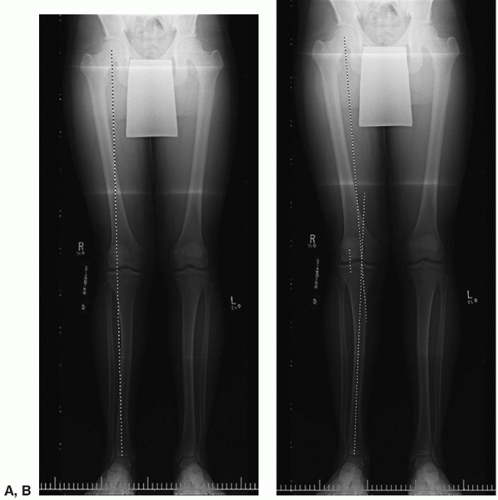 FIGURE 28-3 Radiographic planning of a distal femoral osteotomy according to the method described by Dugdale et al (6). (A) A native weight-bearing line is drawn on the bilateral standing full-length anteroposterior radiograph. (B) Planned axes of tibia and femur are drawn through the point of correction. (C) The planned osteotomy is marked, and the length is taken. (D) The length is transferred to the new femoral weight-bearing line. (E) The horizontal distance between the lines equals the size of the corrective osteotomy. |
 FIGURE 28-3 (Continued) |
SURGICAL TECHNIQUE
A distal femoral valgus osteotomy can be performed using two surgical techniques: (1) distal femoral medial closing-wedge osteotomy and (2
 Traditional Medial Approaches to the Knee
Managing Patella Problems in Primary Total Knee Arthroplasty
Varus and Valgus Deformities
Simultaneous Total Knee Arthroplasty and Femoral Osteotomy
Impaction Bone Grafting for Large Bone Defects
Unicompartmental Total Knee Arthroplasty With Conventional Instrumentation
Traditional Medial Approaches to the Knee
Managing Patella Problems in Primary Total Knee Arthroplasty
Varus and Valgus Deformities
Simultaneous Total Knee Arthroplasty and Femoral Osteotomy
Impaction Bone Grafting for Large Bone Defects
Unicompartmental Total Knee Arthroplasty With Conventional Instrumentation




Related posts:
Traditional Medial Approaches to the Knee
Managing Patella Problems in Primary Total Knee Arthroplasty
Varus and Valgus Deformities
Simultaneous Total Knee Arthroplasty and Femoral Osteotomy
Impaction Bone Grafting for Large Bone Defects
Unicompartmental Total Knee Arthroplasty With Conventional Instrumentation
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
