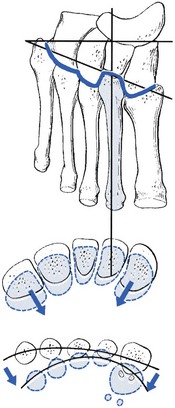
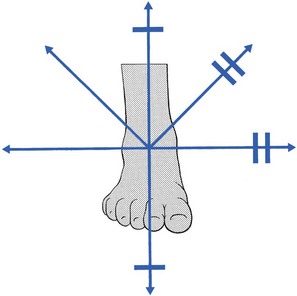
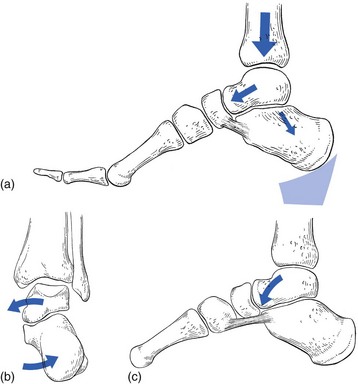
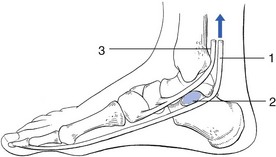
59 At the distal (Lisfranc’s) joint, considerable rotation round the second metatarsal shaft is possible (Fig. 59.1). Because of the specific structure of the joint line, plantiflexion of the metatarsals will always be accompanied by a movement towards the second metatarsal. Therefore a plantiflexion movement at the midtarsal joint increases the curvature of the anterior arch, whereas dorsiflexion is associated with flattening. The capsular pattern at the midtarsal joints is increasing limitation of adduction, supination, plantiflexion and dorsiflexion (Fig. 59.2). The mid-foot finally fixes in an abducted and pronated position because of a spasm of the peroneal muscles. If an excessive strain is imposed on the midtarsal joints – for example, as the result of a deformity (e.g. plantaris) – the power of the musculature (tibialis posterior and flexor hallucis longus) becomes insufficient to maintain the longitudinal arches during weight bearing.2 After some time, the midtarsal ligaments become stretched, elongate and undergo inflammatory changes, so that pain results. Elongation promotes excessive movements at the midtarsal joints, which cause the plantar arch to flatten during weight bearing. As a result, the forefoot dorsiflexes and abducts, which causes the inner side of the foot to become prominent and further overstretches the calcaneonavicular ligament. In due course, the excessive motion of the joints and their poor alignment leads to inflammation of the capsule and to structural damage of the articular surfaces, which finally results in structural deformity and arthrosis. Initially, the body weight bears on the talus via a downward thrust through the tibia. The talus is supported by the calcaneus, on which it lies obliquely. The former therefore has a tendency to glide in a medial and forward direction, especially in patients with an equinus deformity at the ankle or in patients with too short plantiflexor muscles. In women who wear high, oblique heels, the talus also tends to be pushed forwards on the calcaneus (Fig. 59.3a). The forward and medial gliding of the talus imposes medial and downward pressure on the anteromedial calcaneal border. The medial pressure forces the calcaneus towards valgus, which may be furthered by a shortening of the Achilles tendon (Fig. 59.3b). The downward pressure of the talus evokes dorsiflexion at the talonavicular joint.3 This increases the depression of the longitudinal arch and can be responsible for greater stress on the plantar ligaments and the fascia plantaris (Fig. 59.3c). The downward pressure of the talus and the consequent dorsiflexion at the talonavicular joint will initiate a number of other events, which are the source of more deformity and trouble: • Because of the obliquity of the joint surfaces, each dorsiflexion in the midtarsal joints is accompanied by some abduction. The downward movement of the talus is thus at the origin of an abduction deformity in the mid-foot. This dorsiflexed and abducted foot overstretches the inner ligaments (calcaneonavicular ligament and capsule of the talonavicular joint). • Dorsiflexion at the midtarsal joint also causes spreading out and abduction of the metatarsals. Abduction is the result of obliquity of the joint line. Spreading out is caused by the specific cone-shaped form of the bases of the metatarsals, which move their heads away from the centre during extension (see online chapter Applied anatomy of the lower leg, ankle and foot). This flattens the anterior arch and results in a splay foot. • Valgus of the calcaneus with possible shortening of the Achilles tendon • Dorsiflexion and abduction of the mid-foot, with flattening of the longitudinal arch and tension in the plantar and medial ligaments • Flattening and abduction of the forefoot, with spreading of the metatarsal heads and loss of the anterior arch • In due course, there will also be some effect on the tendons: that of the tibialis posterior, the first invertor of the foot, suffers strain and becomes inflamed. The tendon of the flexor hallucis longus, which is not only an invertor, but also, through its position under the sustentaculum tali, has a specific function as a stabilizer of the anterior part of the calcaneus, also becomes strained (Fig. 59.4). Fig 59.4
Disorders of the midtarsal joints
Capsular pattern
Subacute arthritis in adolescence
Subacute arthritis in middle age
Non-capsular pattern
Midtarsal strain
Mechanism
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree