Fig. 1
Radiographs (anterior-posterior and lateral-a and long leg view-b) of the left knee showed a primary cruciate retaining mobile-bearing TKR. No signs of loosening or infection. The tibial component was well positioned. No over- or undersizing of the TKR components. A patella infera was seen which was attributed to a proximalisation of the joint line. In addition, there was a significantly flexed femoral TKR component
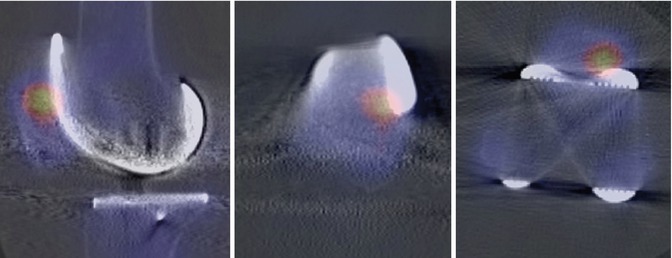
Fig. 2
99mTc-HDP-SPECT/CT images of the left knee showed no increased tracer uptake around the femoral and tibial TKR component indicating a well-fixed TKR and no infection. There was markedly increased bone tracer uptake of the patella indicating an increased loading of the patella due to a patella infera
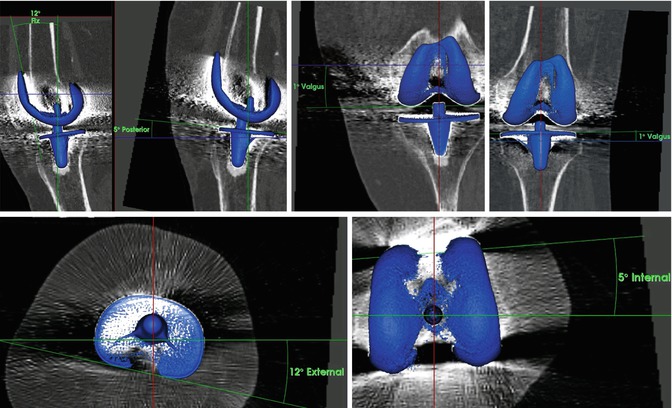
Fig. 3
Measurements of the TKR component position using a customised and validated software showed – 12° flexion (left) and 5° internal rotation (middle) of the femoral TKR component and 5° posterior slope of the tibial TKR component (left up) and 12° external tibial rotation (left bottom)
Questions
1.
What is your differential diagnosis now?
2.
What are your next steps in diagnostics?
99mTc-HDP-SPECT/CT confirmed that there was no loosening or infection. Hyperflexion of the femoral component of the TKR on the left side (12°) with a consecutive ventral, over-shielding, and patellar stress at the upper pole of the left patella baja (Figs. 2 and 3).
Questions
1.
What is your diagnosis and proposed treatment?
2.
 Laboratory Analysis in the Assessment of Painful Total Knee Replacement
Laboratory Analysis in the Assessment of Painful Total Knee Replacement
 Periprosthetic Fractures Following Total Knee Replacement
Periprosthetic Fractures Following Total Knee Replacement
 Joint Line Restoration in Revision Total Knee Replacement
Joint Line Restoration in Revision Total Knee Replacement
 Discussion to Chap. 34: Persistent/Recurrent Pain After TKR Not Always TKR Related
Discussion to Chap. 34: Persistent/Recurrent Pain After TKR Not Always TKR Related
 Use of Stems in Revision Total Knee Replacement
Use of Stems in Revision Total Knee Replacement
 Periprosthetic Fracture Treatment in Total Knee Replacement
Periprosthetic Fracture Treatment in Total Knee Replacement




How would you address the femoral component malposition?
Related posts:
Laboratory Analysis in the Assessment of Painful Total Knee Replacement
Periprosthetic Fractures Following Total Knee Replacement
Joint Line Restoration in Revision Total Knee Replacement
Discussion to Chap. 34: Persistent/Recurrent Pain After TKR Not Always TKR Related
Use of Stems in Revision Total Knee Replacement
Periprosthetic Fracture Treatment in Total Knee Replacement
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
