FIGURE 12-1 Annual incidence of all fractures in children. (From Landin LA. Epidemiology of children’s fractures. J Pediatr Orthop B. 1997;6:79–83.)
Large studies that distinguish distal radial fractures from forearm shaft fractures indicate that overall, radial shaft injuries rank as the third most common fracture of childhood (behind distal radial and supracondylar humeral fractures).60 Open fractures in children are most often fractures of the shaft of the radius and ulna or tibial shaft fractures.60 Among pediatric fractures, forearm shaft injuries are the most common site of refracture.185 Forearm shaft fractures have been shown to occur most commonly in the 12- to 16-year-old age group, a challenging age group to treat.60 The impact of increasing age on fracture incidence is further illustrated by Worlock and Stower,353 who showed that the rate of forearm shaft fractures in school-age children (more than 5 years old) is more than double than that in toddlers (1.5 to 5 years old). Age also may have an effect on injury severity. Many experienced clinicians have pointed out the increasing level of treatment difficulty as the level of forearm fracture moves proximally,71,145,243,328,329 and more proximal fractures tend to occur in older patients.71
ASSESSMENT OF DIAPHYSEAL RADIUS AND ULNA FRACTURES
Mechanisms of Injury for Diaphyseal Radius and Ulna Fractures
The primary mechanism of injury associated with radial and ulnar shaft fractures is a fall on an outstretched hand that transmits indirect force to the bones of the forearm.3,66,167 Biomechanical studies have suggested that the junction of the middle and distal thirds of the radius and a substantial portion of the shaft of the ulna have an increased vulnerability to fracture.151 Often, a significant rotational component is associated with the fall, causing the radius and ulna to fracture at different levels (Fig. 12-2).93,210 If the radial and ulnar fractures are near the same level, a minimal torsional component can be inferred (Fig. 12-3). If comminution is present, higher-energy trauma should be suspected.84 Significant hyperpronation forces are associated with isolated shaft fractures of either the radius or the ulna and concomitant dislocation of either the distal or the proximal radioulnar joint (PRUJ). Thus, in any single-bone forearm shaft fracture, these important joints need to be closely scrutinized. Galeazzi and Monteggia fracture dislocations are discussed in Chapters 11 and 14, respectively.

FIGURE 12-3 Radial and ulnar shaft fractures occurring at same level, implying no significant rotation.

FIGURE 12-2 Radius and ulna shaft fractures occurring at different levels, implying rotational mechanism.
A direct force to the arm (such as being hit by a baseball bat) can fracture a single bone (usually the ulna) without injury to the adjacent distal or PRUJs.31 Isolated ulnar shaft fractures have been referred to as “nightstick fractures.” Alignment of the radial head should be confirmed in any child with such a fracture to avoid a “missed Monteggia” injury.149 Isolated radial shaft fractures are rare but notoriously difficult to reduce with closed methods.70,92
The mechanisms of injury of two particular forearm fracture patterns, traumatic bowing (also known as bow fractures or plastic deformation)264 and greenstick fracture, also bear mentioning. The bone behaves differently based on the direction of the forces applied to it. This is the so-called anisotropic property of bone, and it can be simply explained as follows: Bone is more resistant to axial forces than to bending and rotational forces.51 Pediatric bone also is much more porous than its adult counterpart and behaves somewhat differently from a biomechanical standpoint.55,236 Because of its porosity, pediatric bone absorbs significantly more energy prior to failure than the adult bone does.74 When relatively slowly applied, longitudinal forces bend the immature bone beyond its elastic limits and into its plastic zone, resulting in traumatic bowing.36,201 Thus, when a bending force is applied relatively slowly, many microfractures occur along the length of the bone, leading to macroscopic deformity without discernible radiographic fracture. This bending can usually be seen radiographically if suspected.
Greenstick fractures represent an intermediate step between plastic deformation and complete fractures.52 On anteroposterior (AP) and lateral radiographs, greenstick fractures show cortical violation of one, two, or three of their radiographic cortices, and thus some bony continuity is preserved. Rotational deformity is considered to be intimately related to the clinical deformity seen with greenstick fractures of the forearm, and the analogy of a cardboard tube that tends to bend as it is twisted has been offered by Holdsworth.145 Specifically, hyperpronation injuries usually are associated with apex-dorsal greenstick fractures of the forearm, and hypersupination injuries usually are associated with the opposite, apex-volar injuries.92,223 The treatment of these greenstick fractures requires a derotation maneuver in addition to correction of any angulation.52,133
Associated Injuries with Diaphyseal Radius and Ulna Fractures
Most fractures of the shafts of the radius and ulna occur as isolated injuries, but wrist and elbow fractures may occur in conjunction with forearm fractures, and the elbow and wrist region needs to be included on standard forearm radiographs.26,75,167,314,351,358 If clinical suspicion is high, then dedicated wrist and elbow films are necessary. The so-called floating elbow injury (fracture of the bones of the forearm along with ipsilateral supracondylar humeral fracture) is a well-described entity that must not be missed.26,272,314,351 Surgical stabilization of both the supracondylar fracture and the forearm fractures has been recommended by multiple authors in recent years30,138,271,272,319,322 to avoid the risk of a compartment syndrome. Galeazzi and Monteggia fracture dislocations also must be ruled out. Compartment syndrome can also occur in conjunction with any forearm shaft fracture.73,362 This rare but potentially devastating complication can lead to a Volkmann ischemic contracture, which has been shown to occur after forearm shaft fractures almost as often as it does after supracondylar humeral fractures in children.224 Patients with severe pain unrelieved by immobilization and mild narcotic medication should be reassessed for excessive swelling and tight forearm compartments. If loosening of the splint, cast, and underlying cast materials fails to relieve pain, then measurement of compartment pressures and subsequent fasciotomy may be necessary.
Abrasions or seemingly small unimportant lacerations that occur in conjunction with forearm fractures must be carefully evaluated because they may be an indication of an open fracture. Clues to the presence of an open fracture include persistent slow bloody ooze from a small laceration near the fracture site and subcutaneous emphysema on injury films. Careful evaluation and, in some situations, sterile probing of suspicious wounds will be necessary. Open forearm fractures are discussed later in this chapter.
Vascular or neurologic injuries are rarely associated with forearm shaft fractures, but the consequences of such injuries are far-reaching. Serial neurovascular examinations should be performed and documented. Radial and ulnar pulses along with distal digital capillary refill should be routinely evaluated. Davis and Green79 reported nerve injuries in 1% (5/547) of their pediatric forearm fracture patients, with the most commonly injured nerve being the median nerve. Combined data from three large series of pediatric open forearm fractures reveal an overall nerve injury rate at presentation of 10% (17/173), with the median nerve once again being the one most commonly injured.128,135,198 To screen for these rare but significant injuries, every child with a forearm fracture should routinely have evaluation of the radial, ulnar, and median nerves for both motor and sensory function.70 Nerve injuries occurring at the time of injury must be differentiated from treatment-related or iatrogenic neurologic deficits.
Davidson78 suggested using the game of “rock-paper-scissors” for testing the median, radial, and ulnar nerves (Fig. 12-4). The pronated fist is the rock and tests median nerve function. The extended fingers and wrist depict paper and test radial nerve function. Fully flexed small and ring fingers, an adducted thumb, and spreading the index and ring fingers mimic scissors and test ulnar nerve function. Further focused testing should also be done on two important nerve branches: The anterior interosseous nerve (branch of median nerve) and the posterior interosseous nerve (branch of radial nerve). The anterior interosseous nerve provides motor function to the index flexor digitorum profundus, the flexor pollicis longus, and pronator quadratus and is best tested by having the patient make an “OK” sign. The posterior interosseous nerve typically innervates the extensor carpi ulnaris, extensor digitorum communis, extensor digiti minimi, extensor indicis, and the three outcropping muscles of the thumb (abductor pollicis longus, extensor pollicis brevis, and extensor pollicis longus).42 Its function is best documented by full extension of the phalangeal and metacarpophalangeal joints. This is especially difficult to test in a patient in a cast or splint that partially covers the fingers. Most injuries that occur in association with forearm fractures are true neurapraxias and typically resolve over the course of days to weeks.73,79

FIGURE 12-4 Upper extremity motor nerve physical examination. A: Rock position demonstrates median nerve motor function. B: Paper position demonstrates radial nerve motor function. C: Scissor position demonstrates ulnar nerve motor function. D: “OK” sign demonstrates function of anterior interosseus nerve.
Signs and Symptoms of Diaphyseal Radius and Ulna Fractures
The signs and symptoms indicating fracture of the shafts of the radius and ulna usually are not subtle. Deformity and pain are the classic findings. Patients typically experience exquisite pain emanating from the involved area. Decreased pronation and supination motion are also usually noted.309 Neither practitioners nor parents are always reliable assessors of children’s pain, and ideally patients should rate their own pain.172,299 Significant anxiety and muscle spasm almost always amplify a child’s painful experience.46,117 It has been suggested that muscle spasm is a protective effort by the body to splint or otherwise protect the injured body part.117 When such muscle spasm occurs in association with certain fracture patterns (e.g., a radial shaft fracture proximal to the pronator teres insertion), it produces predictable fracture displacement (e.g., a pronated distal radial fragment and a supinated proximal fragment).
More subtle fractures present special diagnostic challenges. Certain pathologic fractures of the forearm may occur in the absence of overt trauma.157,181 Many minimally displaced fractures of the shafts of the radius and ulna can be mistaken for a “sprain” or “just a bruise” for several days to several weeks. This usually occurs in young children who continue to use the fractured arm during low-level play activities. As a general rule, a fracture should be suspected if the child has not resumed all normal arm function within 1 or 2 days of injury.
Imaging and Other Diagnostic Studies for Diaphyseal Radius and Ulna Fractures
Because important forearm fracture treatment decisions frequently are based on radiographic measurement of angular deformities, it must be remembered that these angles are projected shadows that are affected by rotation.102 If angulation is present on both AP and lateral views (commonly called two orthogonal views), the true deformity is out of the plane of the radiographs, and its true magnitude is greater than that measured on each individual view. Certain forearm shaft fracture deformities are clearly “two-plane deformities” whose maximal angular magnitude is in some plane other than the standard AP or lateral plane (Fig. 12-5).16 Bar and Breitfuss16 produced a table (based on the Pythagorean theorem) that predicts the true maximal angulation. Accurate deformity measurement can be made when angulation is seen on only one view and there is no angulation on the other orthogonal view.

FIGURE 12-5 Underestimation of true angulation. A: “Out of the AP and lateral plane” underestimates angulation at 30 degrees. B: True AP and lateral demonstrates that true maximal angulation is 40 degrees.
Evans pointed out the importance of tracking the rotational alignment of the free-moving radial fragment by ascertaining the relative location of the bicipital tuberosity. This was a major step forward in refining the orthopedic care of these forearm injuries. On a fully supinated AP radiograph of an unfractured forearm, the bicipital tuberosity points predominantly in a medial direction (nearly 180 degrees opposite of the radial tuberosity).94 The radius and ulna are also nearly parallel to each other on such a view. On a fully pronated AP radiograph of an unfractured forearm, the bicipital tuberosity points in a lateral direction and the radial tuberosity is situated medially.94 The radius also crosses over the ulna in a pronated AP view. Rang265 noted that in an unfractured limb, the bicipital tuberosity tended to align with a point near the thenar eminence (Fig. 12-6), more nearly a 165-degree relationship than a true 180-degree one. These relationships are best assessed on standard radiographs that include the entire forearm on one film75,257,329 rather than the specialized bicipital tuberosity view originally suggested by Evans.94 A CT scan of both forearms with cuts through the bicipital tuberosity and the radial styloid is probably the best way to accurately identify a rotational malunion after a fracture that could be causing a loss of forearm rotation. The ulna can be similarly assessed by comparing the distal ulnar styloid to the proximal coronoid process on orthogonal views (similar to bicipital tuberosity and radial styloid, the coronoid process, and ulnar styloid should be 180 degrees apart). CT scan cuts of the coronoid process and the ulna styloid on the fractured and nonfractured sides are most reliable for measuring the rotational alignment of the ulna.

FIGURE 12-6 Rang’s illustration depicting the position of the bicipital tuberosity on AP and lateral views with the forearm in pronation, supination, and neutral position. (From Rang M. Children’s Fractures. Philadelphia, PA: JB Lippincott, 1974:126.)
Classification of Diaphyseal Radius and Ulna Fractures
Fractures of the shafts of the radius and ulna often are described in rather imprecise terms such as “both-bone forearm fracture” and “greenstick fracture.” Radiographs confirm the diagnosis of forearm shaft fracture and are the basis for most classification systems. The most comprehensive classification of forearm fractures is the one adopted by the Orthopaedic Trauma Association (OTA).10 Although this system is sound in concept, its 36 discrete subtypes10 make it impractical for everyday clinical use, and it has not been widely used by clinical researchers.269 Despite its complexity, the OTA classification does not account for one of the most important prognostic factors in pediatric forearm shaft fracture: Location of the fracture in the distal, middle, or proximal third of the shaft.
Clinicians and clinical researchers have favored simpler descriptions of forearm shaft fractures. An orderly and practical approach to forearm shaft fracture classification should provide information about the bone (single bone, both bones), the level (distal, middle, or proximal third), and the pattern (plastic deformation, greenstick, complete, comminuted). Bone involvement is important because it not only indicates the severity of injury but also influences suspicion regarding additional soft tissue injury (e.g., single-bone injury increases the likelihood of a Monteggia or Galeazzi injury)333 and affects reduction tactics (unique single-bone fracture reduction strategies can be used) (Fig. 12-7). Single-bone shaft fractures occur, but both-bone fractures are far more common. Level is important for anatomic reasons relative to muscle and interosseous ligament attachments, as well as differences in prognosis for distal-, middle-, and proximal-third shaft fractures. The pattern is important because it significantly alters the treatment approach. For example, the primary reduction strategy is very different for greenstick fractures (rotation) compared to that for complete fractures (vertical traction). Certain comminuted fractures (e.g., comminution of both bones) may preclude reduction and casting and require surgical fixation.104,106 Fortunately, comminuted fracture patterns are rare in children. For all practical purposes, the buckle fracture pattern that is common in the distal radial metaphysis never occurs in isolation in the shaft region. The typical buckle fracture “speed bump” may accompany either plastic deformation or greenstick fractures. Thus, there are two bones, three levels, and four common fracture patterns (Fig. 12-8). We believe this is a practical and clinically relevant way to describe forearm shaft fractures.216

FIGURE 12-7 Isolated ulnar shaft reduction technique (Blount). Valgus force applied to fracture site and direct thumb pressure over distal ligament.

FIGURE 12-8 Practical classification of forearm shaft fractures. (Distal dotted line defined by proximal extent of the Lister tubercle and proximal dotted line defined by proximal extent of bicipital tuberosity.)
Once the forearm fracture has been described in the terms of this practical classification, fracture displacement must be evaluated. Fracture displacement can occur as angulation, rotation, shortening, or translation. Angulation is important in treatment decision-making and can be measured with reasonable reliability.189,320 Rotation is a simple concept, but it is difficult to assess clinically.93,257 The best that usually can be done is to roughly estimate rotation within a 45-degree margin of error.71,257 Based on available clinical studies, it appears that less than 1 cm of shortening should be accepted in either single-bone or both-bone fracture patterns.50,80,85,214,274 It has also been suggested that the shortening that accompanies displaced fractures may help preserve future motion through interosseous membrane relaxation.257 Completely (100%) translated fractures of the middle third71,257 and distal third85,214,274 of the forearm have been shown to reliably remodel. Certain situations may raise concern regarding complete translation, such as isolated middle-third radial fractures with medial (ulnar) displacement that significantly narrows the interosseous space and translation in children who have less than two full years of growth remaining, because remodeling of the translated fracture site is less predictable than in younger children.233,236
Outcome Measures for Diaphyseal Radius and Ulna Fractures
The fundamental reason for treating fractures of the shafts of the radius and ulna relates to the likelihood of bad results in the absence of adequate care. Data from certain developing countries may be as close as we come to natural history studies of untreated fractures. Archibong and Onuba12 reported on 102 pediatric fracture patients treated in Southeastern Nigeria. Their patients most commonly had upper extremity fractures, and they frequently experienced significant delays in seeking medical treatment, which led to high rates of malunion requiring surgical treatment.12 Other Nigerian authors have found that young age was not protective against fracture malunion (more than 50%) and nonunion (25%) following traditional bonesetter treatment.239 It is unclear whether children treated in this fashion are better or worse off than if they had received no treatment at all. The rationale for treating pediatric forearm shaft fractures is thus based on the premise that the results of modern orthopedic treatment will exceed “pseudo-natural histories” such as these.
The consequences of excessively crooked (and malrotated) forearm bones are both aesthetic and functional (Fig. 12-9).28,33,145,209,232,329 Limited forearm supination following a forearm shaft malunion is illustrated in Figure 12-10. Despite their great concern to parents, aesthetic issues have not been formally studied, and as a result the practitioner must interpret forearm appearance issues on a case-by-case basis. Clinical experience has shown that the ulna appears to be less forgiving from an aesthetic standpoint because of its long subcutaneous border. Early and repeated involvement of the parents (or other legal guardians) in an informed and shared decision-making process is essential.

FIGURE 12-9 Effect of forearm malunion on forearm motion. A: Normal arc of forearm motion. B: Angulated radius leads to diminished arc of forearm motion. (From Ogden JA. Skeletal Injury in the Child. Philadelphia, PA: Lea & Febiger; 1982:56–57.)


FIGURE 12-10 A 6-year-old male who suffered a right forearm shaft malunion. A: Radiograph one week after fracture showing complete midshaft ulnar and proximal-third radial fractures. B: Healed fractures at 6-month follow-up. C: Twenty-month follow-up. D: Twenty-six month follow-up. E: Symmetrical pronation. F: Limited supination on the right G: Axial alignment with palms together. H: An effort at supination. I: Axial alignment in pronation.
Bony malunion and soft tissue fibrosis have both been implicated as causes of limited forearm motion after forearm shaft fractures.144,232 Limited forearm pronation and supination can have significant effects on upper extremity function.26,245,257 Inability to properly pronate often can be compensated for with shoulder abduction, but no easy compensatory mechanism exists for supination deficits.70,145,245,257 Daruwalla75 identified a nearly 53% rate of limited forearm rotation (subtle in some, dramatic in others) in his series of 53 children with forearm fractures and attributed it to angular deformity and rotational malalignment. Several patients in Price’s257 classic series of pediatric forearm malunions had severe forearm range-of-motion losses that significantly limited vocational and recreational activities. Trousdale and Linscheid329 reported range-of-motion losses severe enough to prompt corrective osteotomies in many of their predominantly pediatric (less than 14 years old at time of injury) patients with forearm malunions. Meier217 also reported significant range-of-motion deficits in association with pediatric forearm malunion.
Range-of-motion losses caused by deformity have been studied by numerous authors using adult cadaveric forearm specimens. Matthews et al.209 studied 10- and 20-degree midshaft angular deformities of the radius and ulna in 10 forearm specimens. They found that 10-degree deformities of either bone individually resulted in little or no measurable motion loss (in the range of 3 degrees or less). When both bones were angulated 10 degrees dorsal, volar, or toward the interosseous membrane, larger motion losses were documented (approximately 10-degree pronation and 20-degree supination). Significantly greater losses of motion occurred when one or both bones were angulated 20 degrees (approximately 40 degrees for both pronation and supination). Some of the 10-degree angulated specimens demonstrated “cosmetically unacceptable deformity.”209 These findings indicate that relatively small angular deformities can be clinically significant.
Additional important information about the influence of fracture level on forearm motion was provided by a series of adult cadaver experiments conducted by Sarmiento et al.281,321 They found that fracture angulation of 15 to 30 degrees led to greater supination losses when the deformity was in the middle third of the forearm (40 to 90 degrees) and greater pronation losses when in the distal third (30 to 80 degrees).321 Fracture angulation of 10 degrees or less in the proximal or middle forearm rarely resulted in more than 15 degrees of motion loss,281,321 but the same angulation in the distal third of the forearm was at times (usually with isolated radius fracture) associated with pronation losses of 20 degrees.281,321 These findings challenge commonly held beliefs that the distal third of the forearm is the most forgiving. These same authors asserted that rotational malalignment led to rotational motion losses that usually were equal in magnitude and opposite in direction to the deformity (e.g., a 10-degree pronation deformity led to a 10-degree loss of supination).321
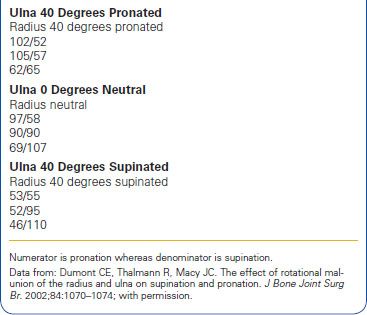
Rotational malalignment of the forearm has been studied in greater detail in recent years, mostly in adults and in the laboratory.88,169,330 In isolated midshaft radial fractures, more than 30 degrees of malrotation was a threshold for significant losses in motion (approximately 15 degrees).169 Isolated midshaft ulnar fracture malrotation did not alter the total arc of forearm motion but did change the set point (e.g., a 30-degree pronation deformity took away 30 degrees of pronation and added 30 degrees of supination).330 Larger ulnar axial malalignment of 45 degrees decreased overall forearm rotation by no more than 20 degrees.330 Large residual ulnar shaft translation has similarly been found to have little impact on forearm rotation.212 Simulated combined radial and ulnar midshaft rotational malunions resulted in the worst motion (more than 50% losses of pronation and supination when 60-degree rotational malunions were in opposite directions).88 Rotational malunions that approximated recommended limits in the literature (45 degrees)257 produced less extreme but real limitations of motion (Table 12-1).88 From these studies and our clinical experience, it appears that the radius is more sensitive to rotational problems and less sensitive regarding aesthetic issues, whereas the ulna is exactly the opposite.
TABLE 12-1 Condensed Range-of-Motion Information
Several generations of orthopedic surgeons have been taught that 50 degrees of pronation and 50 degrees of supination represent adequate forearm motion.222 It must be remembered that this classic study performed by Morrey and his Mayo Clinic colleagues involving 33 normal subjects (18 female, 15 male) from 21 to 75 years of age is not the only study that addresses forearm motion. The average arc of normal forearm motion for the Mayo group (68-degree pronation to 74-degree supination)222 was approximately 20 degrees less than that measured in 53 healthy male subjects who were not older than 19 years old (77-degree pronation to 83-degree supination) reported by Boone and Azen35 and 35 degrees less than that reported by Rickert et al.270 (75-degree pronation to 100-degree supination) in 141 subjects of both sexes between 20 and 30 years of age. Contemporary three-dimensional motion analysis has revealed that maximal pronation occurs when pouring liquid from a pitcher and maximal supination commonly occurs during personal hygiene activities.262 Thus, it seems clear that the forearm motion “goals” reported by Morrey et al.222 are not necessarily ideal or even optimal, but rather they may be considered as the minimal limits of forearm function. Stated another way, losing 20 degrees or 30 degrees of either pronation or supination carries the potential for significant functional impact upon important activities of daily living. At the present time, loss of pronation can affect keyboarding and computer usage.
The goal of treatment is to achieve satisfactory healing of the forearm injury within the established anatomic and functional guidelines while also taking into account the reasonable degree of remodeling that can be expected in growing children.156 Most of the time, these goals can be achieved with closed fracture care, and little or no radiographic or clinical abnormality can be detected following healing. A paradox exists in pediatric forearm fractures whereby anatomic radiographic alignment is not always associated with normal motion, and normal motion often is associated with nonanatomic radiographic healing.144,228,232,321 Herein lies the inherent controversy between operative and nonoperative treatment approaches (Table 12-2). In patients with anatomic radiographs, range-of-motion problems usually have been attributed to scarring of the interosseous membrane.170,245,257 With nonanatomic radiographs (incomplete remodeling), range-of-motion deficits usually are attributed to the radiographic abnormalities. Thus, treatment of forearm shaft fracture must balance the risk of allowing stiffness to occur secondary to malunion against the risk of creating stiffness secondary to surgical procedures.
TABLE 12-2 Pros and Cons of Cast Versus Surgical Treatment

The rationalization for the remodeling of pediatric forearm fractures has strong historical support,22,31,48,241 but knowledge of the limits of remodeling must be taken into consideration. Established reduction criteria state that complete (100%) translation is acceptable,214,257 as well as up to 15 degrees of angulation and up to 45 degrees of malrotation.257 The fundamental reason for treating fractures of the shafts of the radius and ulna relates to the likelihood of bad results in the absence of adequate care or acceptable remodeling. As noted earlier, data from certain developing countries may be as close as we come to natural history studies of untreated fractures. Nigerian12,239 studies indicate high rates of malunion with untreated or bonesetter treatment of diaphyseal fractures.
Published clinical studies have shown that pediatric forearm shaft fractures have great remodeling potential that occurs through several mechanisms.288 The distal radial epiphysis will redirect itself toward normal at about 10 degrees per year. As long as the physis is open, this rate is independent of age. Although the epiphysis will return to normal direction, it will have much less effect on correcting an angular deformity at the midshaft compared to fractures at the subphyseal level. Remodeling also occurs with lengthening of the bone through growth, which produces an apparent decrease in angulation, especially if measured as the difference between the proximal and distal ends of the bone. The bone also remodels by intramembranous apposition on the concave side and resorption on the convex side.74,156,288 This occurs throughout life, but more rapidly when driven by the thick periosteum found in children. Larsen186 found that although the epiphyseal angle realigns quickly, children older than 11 years correct bone angulation less than the younger children. Thomas stated the following regarding pediatric forearm remodeling potential: “We should not fail to recall that the remodeling capabilities of the bones of children have not changed in the last million years and that open reduction and internal fixation must be undertaken only after due deliberation.”323 Others such as Johari158 would state that if one critically evaluates the limits of forearm shaft remodeling capacity you will find a much higher rate (approximately 50%) of incomplete remodeling in children over 10 years of age.
The perfect (or nearly perfect) pediatric diaphyseal forearm fracture outcome study has not yet been performed, therefore scientific answers regarding optimal treatment are lacking.107 However, there is a growing consensus among pediatric orthopedic trauma surgeons that there are patient subsets (usually older patients with more proximal fractures) whose outcomes are clearly improved by flexible intramedullary nail surgical intervention.347 A large retrospective cohort study focusing on radiographic outcomes has indicated that among pediatric forearm shaft fracture patients who underwent reduction, most (51%) exceed established radiographic criteria over the course of 2 to 4 weeks.40 This is greatly concerning as a very clear relationship exists between radiographic and clinical outcomes for forearm shaft injuries in both adults and children.37,87,166 For those patients deemed at higher risk, the risk–benefit ratio also appears to be favorable as flexible nail surgical complications are mainly minor and in some respects measurably lower than nonoperative forearm shaft fracture care.279,300
PATHOANATOMY AND APPLIED ANATOMY RELATING TO DIAPHYSEAL RADIUS AND ULNA FRACTURES
The forearm is a large nonsynovial joint with nearly a 180-degree arc of motion. Its bones, the radius and ulna, are not simple straight bony tubes. The shaft of the radius is a three-sided structure with two prominent curvatures. One major gradual convexity (approximately 10 degrees with its apex lateral-radial) is present along its midportion; a second, more acute curve of approximately 15 degrees with its apex medial occurs proximally near the bicipital tuberosity.100,127,278 The deviation along the midportion is commonly referred to as the radial bow, and maintenance of this normal contour is a goal of forearm shaft fracture care.260,284,285 The most important bony landmarks of the radius are the radial styloid (lateral prominence) and the bicipital tuberosity (anteromedial prominence), which are oriented about 135 degrees away from each other (Fig. 12-11).220 Maintenance of the styloid-tuberosity rotational relationship is another forearm shaft fracture principle. The nutrient artery of the radius enters the bone in its proximal half and courses anterior to ulnar (medial).120 Such nutrient vessels typically are seen on only one orthogonal view and should not be confused with fracture lines. In cross section, most of the shaft of the ulna is also shaped like a classic three-sided prism, although its more distal and proximal portions are much more circular. The most important bony landmarks of the ulna are its styloid process (distally) and its coronoid process (proximally). These two landmarks are oriented nearly 180 degrees from one another, with the styloid aimed in a posterior (dorsal) direction and the coronoid in an anterior (volar) direction.220 Tracking styloid–coronoid rotational alignment of the ulna is another part of forearm shaft fracture care. The ulnar shaft has mild curvatures in both its proximal (apex lateral/radial) and distal (apex medial/ulnar) portions but is otherwise relatively straight.127,278 The nutrient artery to the ulna enters the bone in its proximal half and courses anterior to radial (lateral).120

FIGURE 12-11 Radial and ulnar anatomy.
The classic works of Evans helped focus attention on rotational deformity associated with fractures of both bones of the forearm.94,210,264 Evans stated, “The orthodox position in which to immobilize these fractures is that of full supination for the upper third, and the midposition for fractures of the middle and lower thirds, these positions being based on the anatomical arrangement of the pronators and supinators of the forearm. However, it is unreasonable to suppose that all fractures at a given level will present the same degree of rotational deformity.”94 The radius and ulna are joined by three major passive restraints: The PRUJ, the distal radioulnar joint (DRUJ), and the interosseous membrane complex, all of which have important stabilizing and load-transferring functions. These structures allow rotation of the radius about the ulna along an axis that runs approximately from the center of the radial head to the center of the distal ulna.146,245 The PRUJ and DRUJ are discussed elsewhere in this book (Chapters 9 and 11). The structure and biomechanic function of the interosseous membrane have been studied extensively in recent years. Hotchkiss et al.150 showed that the central band of the interosseous membrane (the interosseous ligament) courses from a point near the junction of the proximal and middle thirds of the radius to a point near the junction of the middle and distal thirds of the ulna. It is an important longitudinal stabilizer of the forearm in that 71% of forearm longitudinal stiffness is provided by the interosseous ligament after radial head excision.150 Transverse vectors have also been identified248 and reflect the stabilizing effect of the interosseous ligament during pronation and supination movements. The interosseous ligament demonstrates tensile properties comparable to the patellar tendon and the anterior cruciate ligament,249 indicative of the magnitude of the arm forces to which this structure is subjected.
Although some difference of opinion still exists,81,110,304 multiple studies have shown that the most strain in the central band of the interosseous membrane is generated when the forearm is in the neutral position.206,207,304 These findings of maximal strain in neutral in cadaver studies also are consistent with radiographic measurement studies71 and dynamic magnetic resonance imaging studies of the forearm showing that the interosseous space is maximal near a neutral position.229 This may help explain certain pathologic situations such as the fixed supination deformity of neonatal brachial plexus palsy211 as well as limitations of pronation and supination because of encroachment on the interosseous space from malangulated fractures (Fig. 12-12).359 The interosseous membrane also serves as an important anchoring point for several forearm muscles: The flexor digitorum profundus, flexor pollicis longus, extensor indicis, and the outcropping muscles (extensor digitorum brevis, abductor pollicus longus).

FIGURE 12-12 Anatomy of interosseous ligament. A: Central oblique orientation of interosseous ligament. B: Interosseous ligament attachment in terms of percentage forearm length. (From Skahen JR III, Palmer AK, Werner FW, et al. Reconstruction of the interosseous membrane of the forearm in cadavers. J Hand Surg Am. 1997;22:986–994.)
The paired and seemingly balanced radial and ulnar bones have an unbalanced number of muscular connections. The ulna typically has 14 attached muscles and the radius only 10 (Tables 12-3 and 12-4).86,127 Powerful supinators attach to the proximal third of the forearm, whereas important pronators attach to its middle and distal thirds (Fig. 12-13). The accompanying vasculature of the forearm is complex: These muscles are supplied by more than 248 vascular pedicles arising from the brachial artery, its branches, or other collateral vessels.268 The radial, ulnar, and median nerves (or their branches) along with the musculocutaneous nerve provide all of the key innervations to the motors that attach to the forearm bones. As mentioned earlier, the median nerve is the most commonly injured nerve with forearm fractures.78,79,128,135
TABLE 12-3 Ten Muscles that Attach to the Radius (and Their Innervation)

TABLE 12-4 Fourteen Muscles that Attach to the Ulna (and Their Innervation)


FIGURE 12-13 Muscle forces acting in proximal, middle, and distal thirds.
The radial nerve proceeds from a posterior to anterior direction and enters the forearm after passing the lateral epicondyle between the brachialis and brachioradialis muscles. Near this same level, it divides into superficial and deep terminal branches. The deep motor branch of the radial nerve is also known as the posterior interosseous nerve. In addition to its routine innervation of the brachioradialis and extensor carpi radialis longus, most commonly (55% of the time) a motor branch arises from the radial nerve proper or its superficial terminal branch to innervate the extensor carpi radialis brevis, whereas the rest of the time (45%) this motor branch comes from the posterior interosseous nerve.2 The superficial branch travels along with and beneath the brachioradialis. The posterior interosseous nerve enters the supinator muscle, passing the fibrous thickening called the arcade of Frohse shortly after branching from the radial nerve proper. It courses within the supinator past the proximal radius, later exiting this muscle dorsally (posteriorly) near the junction of the proximal and middle thirds of the radius. Following its emergence from the supinator, the posterior interosseous nerve branches repetitively to the superficial extensors and the deeper outcropping muscles. The ulnar nerve enters the forearm between the two heads of the flexor carpi ulnaris.122 It traverses the forearm between the flexor carpi ulnaris and the flexor digitorum profundus. In the distal forearm, it lays just beneath the flexor carpi ulnaris. The median nerve enters the forearm as it passes between the two heads of the pronator teres.57 It next passes beneath the archway created by the two heads of the flexor digitorum superficialis. The median nerve then continues down the course of the forearm nestled between the flexor digitorum superficialis and the flexor digitorum profundus. It becomes much more superficial as it nears the level of the carpal tunnel. The anterior interosseous branch arises from the median nerve at the level of the pronator and travels deep with the anterior interosseous vessels. Abundant muscles shield the radial, ulnar, and median nerves from the shafts of the radius and ulna through most of the forearm except for the posterior interosseous nerve near the proximal radius.
Common Surgical Approaches of Diaphyseal Radius and Ulna Fractures
The large exposure required for plate fixation of pediatric forearm fractures can be achieved with: The Henry (anterior) or Thompson (posterior) approaches to the radial shaft and the direct (medial) approach to the ulnar shaft.72,226 Compartment syndrome release usually requires the serpentine incision of McConnell’s combined approach.142 These approaches and their variations are well described and illustrated in detail elsewhere.4,18,90,148,296 For open reduction of both the radius and the ulna, most authors favor separate incisions to minimize the possibility of communicating hematoma and the development of a radioulnar synostosis.184,260,332 The Thompson approach to the radius is generally used for fractures of its proximal third357 but requires special care to protect the posterior interosseous nerve.83,218,318 Other authors have emphasized the utility of the Henry approach for plating of the entire radius including the proximal aspect.218 When open reduction is done in conjunction with other internal fixation techniques (e.g., intramedullary fixation), limited versions of the same surgical approaches are used.
Indirect reduction and internal fixation of forearm fractures require knowledge of appropriate physeal-sparing entry portals about the distal and proximal forearm. Because of the relative inaccessibility of its proximal end, the radius usually is approached only distally through either a dorsal or radial entry point. The dorsal entry point is near the proximal base of the Lister tubercle or just lateral to it in a small bare area between the second and third dorsal compartments. This location is a short distance proximal to the physis of the distal radius. Another dorsal alternative is pin entry just medial to the Lister tubercle, between the third and fourth dorsal compartments,273 but this may entail greater risk to the extensor tendons, especially the extensor pollicus longus. The most commonly used radial entry point is located in line with the styloid process just proximal to the physis.354 Entry in this area passes adjacent to the first dorsal compartment, and thus the tendons of abductor pollicis longus and extensor pollicis brevis (as well as branches of the superficial radial nerve) must be protected (Fig. 12-14). Because of its extensive branching pattern, portions of the superficial branch of the radial nerve may be at risk when dorsal or radial intramedullary entry points are used.1,14


FIGURE 12-14 Distal radial entry. A: Distal radial incision in proximity to superficial branch of radial nerve. B: Distal radial entry position for intramedullary rod placement in relationship to superficial branch of radial nerve. C: Radiograph of lateral starting point for intramedullary nail. D: Alternate entry point just proximal to the Lister tubercle between second and third dorsal compartments.
Both distal and proximal intramedullary entry sites for the ulna have been described.192,197,256,297,335 In the distal portion of the ulna, an entry site can be made proximal to the physis and in the interval between the extensor carpi ulnaris and flexor carpi ulnaris tendons. Care must be taken to avoid branches of the dorsal cutaneous sensory nerve. Ulnar entry is most easily accomplished in the proximal portion of the bone along its lateral metaphyseal border (just distal to the olecranon apophysis), piercing peripheral fibers of the anconeus (Fig. 12-15).45,188,194 This anconeus entry site described by the Nancy group avoids the physis and avoids the painful bursa that tends to form over “tip of the olecranon” pins.

FIGURE 12-15 Proximal ulnar entry. A: Anconeus entry point. B: Radiograph of proximal ulnar entry point.
Transphyseal approaches to both the distal radius363–365 and the proximal ulna8,197,318 have been suggested by some authors. Significant growth potential exists at the distal radius (approximately 10 mm per year), whereas there is proportionately less from the olecranon apophysis (approximately 2 mm per year). There is an unnecessary risk to the radial physis and few if any technical advantages to transphyseal entry of the radius in diaphyseal level fracture fixation. The ulna apophyseal entry site is used in many centers.
TREATMENT OPTIONS FOR DIAPHYSEAL RADIUS AND ULNA FRACTURES
Nonoperative Treatment of Diaphyseal Radius and Ulna Fractures
Indications/Contraindications (Table 12-5)
TABLE 12-5 Diaphyseal Radius and Ulna Fractures

Most pediatric radial and ulnar shaft fractures can be treated by nonoperative methods.365 Low-energy, undisplaced, and minimally displaced forearm fractures can be immediately immobilized in a properly molded (three-point mold concept of Charnley) above-elbow cast.8 If post-traumatic tissue swelling is a concern, noncircumferential splint immobilization (e.g., sugar-tong splint) can be used initially.70,325,361 For fractures in the distal third of the forearm, below-elbow casting has been shown to be as effective as above-elbow casting in maintenance of satisfactory fracture alignment.61,113 Appropriate follow-up is important for these undisplaced fractures (an initial follow-up radiograph usually is taken 7 to 14 days after injury) because displacement may still occur for a variety of reasons: New trauma to the extremity, male gender, and poor casting technique.70,114,289,361
Good casting technique is infrequently discussed in contemporary orthopedic textbooks and sometimes is underemphasized during orthopedic residency training. The principles of good forearm casting technique include: (a) interosseous molding, (b) supracondylar molding, (c) appropriate padding, (d) evenly distributed cast material, (e) straight ulnar border, and (f) three-point molding (Fig. 12-16). The risk of excessive cast tightness can be minimized through the use of the stretch-relax fiberglass casting technique described by Davids et al.76 Chess et al.61 described a cast index for distal radial fractures defined as the sagittal cast width divided by the coronal cast width at the level of the fracture site; a normal ratio is considered to be 0.70. The cast index has not been validated for forearm shaft fractures, but it embodies the sound concept of good interosseous molding. Techniques such as pins and plaster and cast wedging also have had a role in fracture care.17,89 Cast wedging is almost always done with an opening wedge technique because this entails less risk of soft tissue impingement.171

FIGURE 12-16 Interosseous mold technique.
Displaced fractures usually require reduction following appropriate analgesia.85,334 Options include hematoma block,108,141,160 regional intravenous (IV) anesthesia43,77,164 and inhalational methods,95,129,141 and IV sedation with propophol. After informed consent for sedation and reduction is obtained, monitored sedation can be used in the emergency department with a combination of narcotics and anxiolytics.175 This typically requires a dedicated nurse to administer oxygen and perform appropriate monitoring functions (vital signs, continuous electrocardiogram, and pulse oximetry).7,64,143 Ketamine protocols are also being used with increased frequency.121,175 Young children with less than 5 or 10 degrees of angulation in the plane of wrist and elbow motion probably do not require the additional trauma, time, expense, and sedation risk involved in a formal reduction because of the predictable remodeling in this age group as long as immobilization brings stability to the fracture and prevents late displacement.12 It has been shown that the more displaced the fracture, the more likely that formal monitored sedation techniques will be used for pediatric forearm fracture reduction as opposed to other techniques.334
More specific closed treatment options are discussed for pediatric forearm injuries in terms of their common fracture patterns: Bow (plastic deformation), greenstick, complete, and comminuted.
Traumatic Bowing/Plastic Deformation
Although traumatic bowing was described by Rauber in 1876,298 it was not widely recognized until Spencer Borden’s classic paper was published in 1974.36 This injury occurs almost exclusively with children’s forearm fractures.178 Bow fractures (Fig. 12-17) show no obvious macroscopic fracture line or cortical discontinuity, but they do demonstrate multiple microfractures (slip lines) along the length of the bow.280 At times, a nearly classic buckle fracture (torus fracture) coexists with a bow fracture. The most common clinical scenario is a plastically deformed ulna along with a more typical fracture of the radius.201

FIGURE 12-17 Bow fracture: Approximately 15 degrees of apex-dorsal bowing of radius and ulna shaft.
Borden36 and subsequent authors stressed the importance of natural remodeling potential in these injuries but voiced concern about this approach in older children (especially those over 10 years of age).36,201,280 Vorlat and De Boeck337 reported incomplete remodeling in 3 of 11 children at long-term follow-up (average 6.7 years) after traumatic bowing of the forearm. Because these three children were between the ages of 7 and 10 at the time of injury, the authors recommended more aggressive efforts at reduction in all patients with clinically significant deformity (more than 10 degrees) older than 6 years of age.337 Traumatic bowing that causes aesthetically and/or functionally unacceptable angular deformity277 should be manipulated under general anesthesia or deep sedation because strong (20 to 30 kg) gradual force applied over 2 to 3 minutes is required to obtain acceptable alignment (Fig. 12-18).280 Application of this reductive pressure over a rolled towel, block, or surgeon’s knee fulcrum followed by a three-point molded cast can substantially (although at times still incompletely) correct the deformity. Care must be taken to avoid direct pressure over adjacent epiphyses for fear of creating a physeal fracture.

FIGURE 12-18 Reduction technique of bow fracture over fulcrum. (From Sanders WE, Heckman JD. Traumatic plastic deformation of the radius and ulna: A closed method of correction of deformity. Clin Orthop Relat Res. 1984;188:58–67.)
Greenstick Fractures
Greenstick fractures present special issues in terms of diagnosis and treatment. Angulated greenstick fractures of the shafts of the radius and ulna at different levels indicate a significant rotational component to the injury (Fig. 12-2). Evans, Rang, and others have stated that the apex-volar angulation pattern usually is associated with a supination-type injury mechanism, whereas most apex-dorsal greenstick fractures involve a pronation-type injury mechanism (Fig. 12-19),92,94,233,265 although exceptions certainly occur.92,132 Often, the apparent angular deformity can be corrected by simply reversing the forearm rotational forces (e.g., reducing an apex-dorsal pronation-type injury with supination). Noonan and Price233 observed that it is difficult to remember whether to use pronation or supination reductive forces and suggested that most fractures can be reduced by rotating the palm toward the deformity. They also noted that most greenstick fractures are supination injuries with apex-volar angulation and thus can be reduced by a pronation movement.233 Pediatric orthopedic researchers from the Arnold Palmer Hospital for Children have recently proposed the “radius crossover sign” as an indicator of significant angular and torsional deformity in greenstick fractures of the radial shaft.355 Proper interpretation of this sign relies on full length forearm films that include a good AP view of the distal humerus.

FIGURE 12-19 Shaft fractures at different levels implies rotational mechanism. A: Apex-volar angulation with supination deformity of the forearm. B: Apex-dorsal angulation with pronation deformity of forearm.
Greenstick fractures that occur near the same level probably have little to no rotational component and are best corrected by manipulative reduction and three-point molding techniques (Fig. 12-3). Charnley believed that greenstick fractures of the forearm in children perfectly illustrated his dictum that “A curved plaster is necessary to make a straight limb.”59 He also stated that “The unsuspected recurrence of angular deformity in greenstick fractures of the forearm, while concealed in plaster, is an annoying event if it takes the surgeon by surprise and is not discovered until the plaster is removed. Parents, quite understandably, may be more annoyed about this happening to their children than if it had happened to themselves, and do not easily forgive the surgeon.”59 Despite these concerns, it is clear from large published reports that greenstick fractures can almost always be successfully treated with nonoperative methods.363
Two philosophies are reflected in the literature regarding greenstick fracture reduction: One in which the greenstick fracture is purposely completed and another in which it is not. Those who favor completing the fracture (dating back at least to the 1859 work of Malgaigne) cite concerns about lost reduction and recurrent deformity that can be prevented only by converting the greenstick into a complete fracture.23,31,106,153 Others prefer to maintain and perhaps exploit some of the inherent stability of the greenstick fracture.5,61,79,92,323 In addition to the traditional view that loss of reduction is less likely if a greenstick fracture is completed, there also is the theoretical advantage of a lower refracture rate because of more exuberant callus formation.61,233 To the best of our knowledge, these theories have not been validated in any controlled clinical studies. Davis and Green79 advocated a derotational approach to greenstick fracture reduction and reported a 10% (16/151) reangulation rate in their series of patients with greenstick fracture. They compared this to the 25% (12/47) reangulation rate in patients with complete fractures and questioned the wisdom of routinely completing greenstick fractures.79 In a prospective study, Boyer et al.41 showed statistically that greenstick fractures maintain their reduction better than complete forearm fractures.
Complete Fractures
Complete fractures in different regions of the shaft of the forearm behave differently from a clinical perspective and have classically been divided into distal-, middle-, and proximal-third fractures. Single-bone complete fractures usually are caused by direct trauma (nightstick fracture) and are difficult to reduce. Blount described a reduction technique that may be effective for reduction of a displaced single-bone shaft fracture. The intact bone is used as a lever to re-establish the length of the fractured bone, and then transverse forces are applied to realign the bone ends (Fig. 12-7). Both-bone complete fractures (often with bayonet shortening) are common and are best treated with finger-trap or arm traction applied over 5 to 10 minutes. This stretches out the soft tissue envelope and aids in both reduction and cast or splint application. Traction allows complete fractures to “seek their own level of rotation” and allows correction of rotational malalignment.79
The position of immobilization for forearm fractures has been an area of debate since the days of Hippocrates.31 Theoretically, the position of forearm rotation in an above-elbow cast or splint affects rotational alignment of complete fractures at all levels; however, a study of distal-third forearm fractures found no significant effect of forearm rotation position on ultimate alignment.41 We are aware of no similar studies analyzing the effects of forearm position on middle- or proximal-third shaft fractures, and treatment is influenced by certain anatomic considerations. Because of the strong supination pull of the biceps, aided by the supinator, complete proximal radial fractures may be best immobilized in supination so that the distal forearm rotation matches that of the proximal forearm (Fig. 12-13). The position of immobilization of fractures in the middle third of the forearm commonly is dictated by whether the radial fracture occurs distal or proximal to the insertion of the pronator teres. Fractures proximal to its insertion are best treated by fully supinating the distal fragment, whereas those distal to its insertion are probably best treated in a neutral position. Fractures at different levels in the midshaft that require pronation or supination as part of the reduction maneuver should be immobilized in the position of reduction.
Manipulated fractures should be evaluated weekly for the first 2 to 3 weeks because most position loss can be recognized and corrected during this time.182,338 Any significant shift in position between visits necessitates cast wedging or a cast change, with remolding and possible fracture remanipulation if unacceptable displacement is present. Voto et al.338 found that, in general, 7% of forearm fractures redisplace; this can occur up to 24 days after the initial manipulation. Davis79 reported a 25% reangulation rate in complete fractures. Remanipulation can be done in the office following administration of oral analgesics. Judicious use of benzodiazepines may also be valuable because of their anxiolytic effects.
Although in adults the above-elbow cast generally is changed to a below-elbow cast after 3 to 4 weeks, this is unnecessary in most children because they heal more quickly and permanent elbow stiffness is rare.173 A cast change at week 3 or 4 also can be traumatic to a young child and carries the additional small risk of cast saw injury. Once the fracture shows good callus formation, the cast can be removed. Because shaft fractures of the radius and ulna in children have a significant rate of refracture,13,185,328 they should be splinted for an additional period of time.69 Parents should be warned that forearm shaft fractures have the highest risk of the risk of refracture, which can occur even 6 to 12 months after the original injury.
Above-elbow casting with the elbow in extension has been suggested for some complete fractures of the middle and proximal thirds.292,341,345 The supination moment exerted by the biceps has been shown to be diminished when the elbow is extended.227 Walker and Rang341 reported successful treatment of 13 middle- or proximal-third forearm shaft fractures with this method (some following failed flexed-elbow casting). They suggested that the “short fat forearms” of some young children prevented successful flexed-elbow casting.341 Shaer et al.292 also reported 20 children treated with this method and emphasized full supination of the forearm. Three of their patients required cast wedging, but at final follow-up 19 of the 20 patients had excellent results.292 One patient who was lost to follow-up for 6 months (presumably removing his own cast) did suffer “mild residual deformity.”292 Walker and Rang341 recommended that benzoin be applied to the skin, in addition to creation of an adequate supracondylar mold, to further secure the cast. Casting the thumb in abduction with extra padding may prevent the cast from sliding. Turco293 suggested that reduction should be obtained with horizontal traction applied to the extended upper extremity, followed by additional steps outlined in Table 12-6. Based on published clinical results, concerns related to cast slippage and elbow stiffness appear to have been overstated.292,341 The main drawback of this technique is its awkwardness as compared to flexed-elbow casting341 (Fig. 12-20).
TABLE 12-6 Technique for Extended Elbow Cast Treatment


FIGURE 12-20 A forearm fracture lost of position while treated in an above-elbow cast with elbow at standard 90-degree elbow flexion. At 3 weeks post injury the arm was remanipulated and placed in an above-elbow cast with elbow extended down to only 45 degrees of flexion, with three- point mold placed. The fracture healed anatomically.
Because radius and ulna shaft fractures have the highest rate of childhood refracture, casting is generally recommended for 6 to 8 weeks. This is followed with a forearm splint until all four cortices are healed and there is no transverse lucency at the site of the original fracture (complete healing).
Comminuted Fractures
Although comminuted forearm fractures are less common in children than in adults,323 they do occur.24,104,106,153,184,357 Comminuted fractures tend to occur in conjunction with high-energy injuries, such as open fractures.153,208 Comminuted forearm fractures deserve special attention because they often require specially tailored treatment approaches. If satisfactory reduction cannot be achieved or maintained by closed methods, then other treatment alternatives should be considered.
One option is to accept some shortening; according to Price,257 this may help maintain motion through interosseous membrane slackening. Shortening of more than 1 cm is unacceptable in either single-bone or both-bone comminuted patterns. Standard closed fracture treatment generally is unsuccessful when both bones are comminuted, and surgical stabilization may be necessary.106 Bellemans and Lamoureux24 reported intramedullary nailing of all comminuted forearm fractures in their pediatric series. Other reported fixation methods for comminuted forearm fractures in children include plate-and-screw devices,104,106 flexible intramedullary nailing for single-bone comminution,269 and pins-and-plaster techniques.339 Bone grafting is rarely if ever indicated in acute comminuted forearm features in children.
Operative Treatment of Diaphyseal Radius and Ulna Fractures
Indications/Contraindications
Duncan and Weiner89 cited an “aggressive surgical mentality” as the reason for frequent operative treatment of pediatric forearm fractures, and Wilkins350 expressed concern about “impetuous” surgeons who are too eager to operate. Cheng et al.60 and Flynn et al.103 documented a 10-fold and sevenfold increase in the rate of operative treatment of forearm shaft fractures in children, but it is unclear as to whether this increase in operative treatment has led to a commensurate improvement in clinical outcomes.
Operative treatment of radial and ulnar shaft fractures usually is reserved for open fractures, those associated with compartment syndrome, floating elbow injuries, and fractures that develop unacceptable displacement during nonoperative management. Residual angulation after closed treatment is much better tolerated by younger children than older adolescents and adults because of the increased remodeling potential in the younger age group.113 As a consequence, adolescents are more likely to benefit from surgical treatment of their forearm fractures than are younger children. Although internal fixation is the standard of care for displaced forearm fractures in adults, the success of nonoperative methods and the complications associated with internal fixation have tempered enthusiasm for its application to pediatric forearm fractures. Compared to closed treatment methods, healing is slower after open reduction and internal fixation,24 no matter what type of implant is used.106 Crossed Kirschner wire (K-wire) fixation techniques that often are used successfully in the distal radius are technically difficult in the shaft region of the radius and ulna. In rare situations, external fixation has been used for pediatric forearm fixation.290
Preoperative planning is essential regardless of which surgical technique is chosen. Assessment of the fracture, including rotation and the presence or absence of comminution, is important. Bone–plate mismatch (because of narrow bones and wide plates) and extensive soft tissue dissection are risks when adult-sized plates are applied to pediatric bones.354 Before intramedullary nailing of fractures, the forearm intramedullary canal diameter should be measured, especially at the narrowest canal dimension; typically this is the central portion of the radius305 and the distal portion of the ulna near the junction of its middle and distal thirds. Precise canal measurement can be difficult,278,306 and the consequences of a nail or pin that is too large are probably worse than those of a nail or pin that is too small.237,287 Modern digital radiography systems have made these measurements easier.244
Plate Fixation
Open reduction and internal fixation of pediatric forearm shaft fractures with plates and screws is a well-documented procedure in both pediatric series242,310,324,332 and adult series that include patients as young as 1358 and even 758 years of age. In one of the early series of pediatric forearm fractures fixed with plates,82 dynamic compression plates and one-third tubular plates applied with standard atlas orthogonal technique (six cortices above and below the fracture site) obtained good results.230 Four-cortex fixation on either side of the fracture site has been shown to be equally effective in pediatric forearm fractures.357
Plate fixation uses the standard adult approach and technique except that smaller plates (2.7-mm compression and stacked one-third tubular), fewer screws, and single-bone fixation often are acceptable.357 Plate fixation may allow more anatomic and stable correction of rotational and angular abnormalities and restoration of the radial bow than with noncontoured intramedullary rods; however, the larger incisions and extensive surgical exposures required for plate fixation have raised concerns regarding unsightly scars273,332,354 and muscle fibrosis with consequent motion loss.357 Although the aesthetic concerns seem valid, ultimate forearm motion is similar with the two techniques, with only minor losses reported in the literature after both plating and intramedullary nailing.73,170,297,331 Fernandez et al.97 recently documented these precise issues very nicely in that they found no significant differences in functional outcome in their plate fixation versus intramedullary nailing patients, but they noted the longer operating room time and inferior appearance of the plated patients’ scars.
Open reduction and internal fixation with plates and screws may be appropriate in the management of fractures with delayed presentation or fractures that angulate late in the course of cast care,135,357 when significant fracture callus makes closed reduction and percutaneous passage of intramedullary nails difficult or impossible.11 Other indications for plate fixation include shaft fractures with significant comminution106 and impending or established malunion329 or nonunion.136,193,237 Several authors have reported good results with plate fixation of the radius only47,105,242,265 or the ulna only (Fig. 12-21).25 Bhaskar and Roberts25 compared 20 children with both-bone plate fixation to 12 with ulna-only fixation and found significantly more complications in the dual plating group, although motion was equal at 1-year follow-up. Single-bone fixation requires satisfactory reduction of both bones. Flynn and Waters105 stated that they would preferentially plate the radius only when the fracture could not be reduced by closed means. Two patients in Bhaskar and Roberts’25 study required open reduction and internal fixation of the radius when it was not adequately reduced after plate fixation of the ulna.

FIGURE 12-21 Single bone plate fixation (radius only). A: A 12-year-old female with both bone forearm fracture (AP and lateral). B: Immediate postoperative images. C: Two-year follow-up images. (Courtesy of Tom Welle, DO.)
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


