Diagnosis and Operative Treatment
David S. Ruch
Introduction
Wrist arthroscopy has become standard for the evaluation and treatment of many degenerative and traumatic conditions in the wrist. The technical ease and superior visualization of these conditions, combined with its relative safety, have made arthroscopic procedures in the wrist a standard method of treatment of a variety of conditions (1,2,3,4).
This chapter discusses standard arthroscopic evaluation of the wrist, as well as repair of peripheral lesions of the triangular fibrocartilage, débridement of degenerative conditions in the wrist.
Operative Indications
Arthroscopy remains the ideal imaging modality to diagnose and facilitate treatment of many conditions in the wrist. Specific indications include but are not limited to the following:
Confirmation and grading of intrinsic and extrinsic ligament injuries
Débridement and thermal shrinkage of these injuries
Repair of peripheral lesions of the triangular fibrocartilage complex (TFCC)
Débridement of the articular disc of the TFCC
Synovectomy for inflammatory conditions of the wrist
Débridement of the stalk of dorsal ganglion cysts
Removal of loose or foreign bodies
Confirmation or facilitation of the reduction of articular fractures of the wrist, specifically of the distal radius and scaphoid
Confirm the reduction of the carpus following complete ligament injuries seen in association with fractures.
No specific contraindications exist, except when open procedures would be more appropriate for either visualization or stabilization of the wrist.
 Figure 2-1 Illustrates the set-up for arthroscopy of the wrist using a portable distraction tower that permits 2.25 to 3.5 kg (5–7 lb) of traction, thereby facilitating visualization of the ligaments. |
Patient Position
Place the patient supine on the operating table with a regional block or general anesthesia in place. A Bier block may be used, but is not advisable for longer procedures.
Perform the procedure under tourniquet control.
Sterilely prepare the arm, and drape it on a hand table with the elbow flexed to 90 degrees.
Place the digits in finger traps, and suspend them from a portable tower (Fig. 2-1). Then apply traction of 2.25 to 3.15 kg (5–7 lb).
Operative Procedure
Insert a needle between the third and fourth dorsal compartments in line with the 12-degree palmar tilt at the radius.
Introduce a total of 7 to 10 mL of lactated Ringer’s into the wrist, taking care to visualize extravasation down the extensor carpi ulnaris sheath.
Make a skin incision at the 3-4 interval, and use a hemostat to gain entrance into the joint.
Place a blunt trochar on the 2.4-mm arthroscope and then introduce the arthroscope into the 3-4 portal.
Diagnostic arthroscopy is typically performed first through the 3-4 portal to identify any radioscaphoid, scapholunate, or triangular fibrocartilage lesions. It is performed sequentially from the dorsal intercarpal ligament insertion on the scaphoid to the radial styloid and the radial extrinsic ligaments (Fig. 2-2).
Notice the radioscapholunate ligament as a synovial infolding immediately ulnar to the long radiolunate ligament and trace it up to the scapholunate interosseous complex. The palmar portion of the complex is composed of fibrocartilage and mirrors the anatomy of distal radius. The palmar (difficult to appreciate arthroscopically) and the dorsal portions are composed of transversely oriented collagen fibers and represent the thickest and strongest portions of the complex (Fig. 2-3).
Pass the arthroscope slightly dorsal to the proximal lunate to avoid articular cartilage injury.
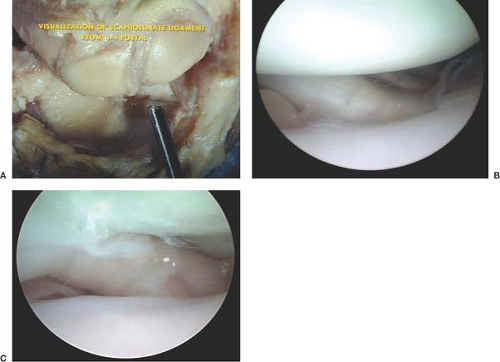
Figure 2-2 (A, B) Position of the arthroscope in 3-4 portal allows visualization of the radial extrinsic ligaments oriented obliquely across the radial styloid to the scaphoid and lunate as well as the radioscapholunate ligament of Testut (C). This ligament also serves as a marker for the scapholunate ligament distally.
Assess the ulnar extrinsic ligaments, including the ulnolunate and the ulnotriquetral ligaments. Trace these ligaments distally to their insertions on the palmar aspect of the lunate and the triquetrum, respectively. The interval between these two ligaments serves as a marker for the lunotriquetral interval. Visualization of the lunotriquetral ligament requires inspection through an ulnar-sided portal, typically at the 6U position (Fig. 2-4A, B).
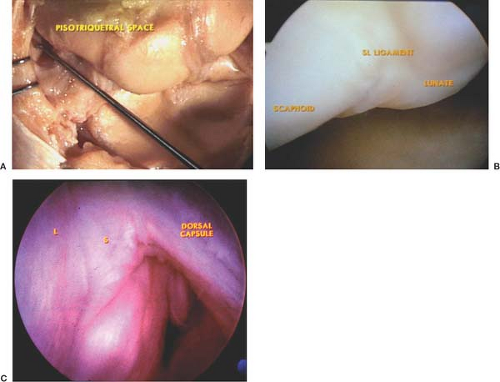
Figure 2-3 The arthroscopic anatomy of the scapholunate interosseous ligament demonstrating the gross and arthroscopic appearance of the central fibrocartilaginous portion and the dorsal collagenous portion. 2-3C shows the Dorsal Capsule and Dorsal extrinsic ligament attachment to the scapholunate interval. These attachments serve as secondary stabilizens of the SL interval and should be assessed at the time of diagnostic arthroscopy.
After performing inspection of the ulnar side of the wrist through the ulnar portal (either 6U or 6R), remove the arthroscope from the ulnar side of the wrist, and place it back in the 3-4 portal. Insert a full radius synovial resector in the 6R portal, using it to perform a limited or more extensive synovectomy. This may allow visualization of occult tears of the TFCC. Occult tears may be covered with granulation tissue, which, when débrided, reveals a peripheral avulsion tear (Fig. 2-5A, B).
Insert a probe to assess the integrity of the deep fibers of the distal radioulnar joint and the interosseus ligaments (4).
Perform midcarpal joint arthroscopy by first placing a needle 1 cm distal to the 3-4 portal. The needle will enter the scaphocapitate articulation (Fig. 2-6).
Create a skin incision, and use a blunt trochar to pass the sheath into the radial midcarpal portal. This allows distal visualization of the scaphocapitate joint. The arthroscope may then be directed ulnarly and dorsal to the capitate to visualize the lunate and assess lunotriquetral joint congruity. In addition, the lunate facet of the hamate may be appreciated through this portal.
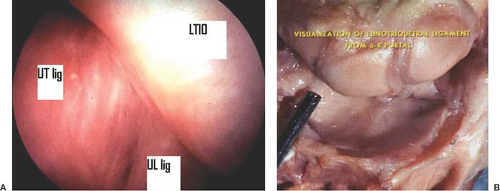
Figure 2-4 A: Demonstrates the anatomy of the lunotriquetral ligament with the arthroscope in the 6R portal. B: A view of the normal ulnocarpal ligaments. Note: The ulnolunate and ulnotriquetral ligaments may be identified palmarly, and the interval between the two serves as a marker for the lunotriquetral interosseous (LTIO) ligament.

Figure 2-5 A: Demonstrates the characteristic synovitis seen through the 3-4 portal at the peripheral attachment of the triangular fibrocartilage complex (TFCC). B: The same tear after débridement.
At this point, insert a needle 1 cm distal to the radiocarpal joint in the interval between the fourth and fifth dorsal compartments of the wrist. Under direct visualization, a needle can be seen to enter the ulnar midcarpal portal at the intersection of the capitohamate and lunotriquetral joints.
To introduce the shaver for a working portal, use a skin incision followed by blunt trochar placement. With any suspicion of interosseus ligament injury with incongruity or collapse pattern, the midcarpal portals can be useful in assessing congruity of this articulation (5). As with all small joint arthroscopy, it is easiest to appreciate incongruity by having the visualization portal further away from the articular surfaces in order to gain perspective. Therefore, it is most useful to assess the lunotriquetral joint from the radial midcarpal portal and the scapholunate articular congruity from the ulnar midcarpal portal. The ulnar midcarpal portal is also useful in assessing congruity of reduction of the scaphoid in arthroscopically assisted reductions (Fig. 2-7).
 Figure 2-6 A: The anatomy of the midcarpal joint is dictated by the proximal pole of the capitate; it is located 1 cm distal to the radiocarpal joint. B: The anatomy with the arthroscope in the radial midcarpal joint. The radial midcarpal portal permits visualization of both the lunotriquetral (LT) interval (B) the lunate facet of the hamate (6) and the distal pole of the scaphoid in the scaphoid-trapezium-trapezoid (STT) joint. |
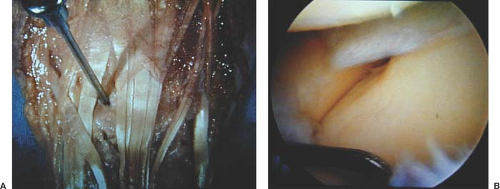 Figure 2-7 The ulnar midcarpal (UMC) portal permits visualization of the congruity of the scapholunate articulation. |
Interosseus Ligament Injuries
Arthroscopy can be of significant benefit in the evaluation and treatment of certain interosseus ligament injuries. Interosseus ligament injuries can be graded on the basis of their arthroscopic appearance (6,7). Geissler et al. (6) graded these injuries in association with distal radius fractures, and this grading system has been used and applied to isolated intrinsic ligament injuries (Fig. 2-8
 Arthroscopic-Assisted Limited Open Reduction
Arthroscopic-Assisted Limited Open Reduction
 Distal Radius Osteotomy
Distal Radius Osteotomy
 Scapholunate Advanced Collapse (SLAC) Reconstruction: Four-Corner Arthrodesis with Headless Screws
Scapholunate Advanced Collapse (SLAC) Reconstruction: Four-Corner Arthrodesis with Headless Screws
 Partial Excision of the Triangular Fibrocartilage Complex
Partial Excision of the Triangular Fibrocartilage Complex
 Arthrodesis of the Rheumatoid Wrist
Arthrodesis of the Rheumatoid Wrist
 Release of the First Dorsal Compartment
Release of the First Dorsal Compartment




Related posts:
Arthroscopic-Assisted Limited Open Reduction
Distal Radius Osteotomy
Scapholunate Advanced Collapse (SLAC) Reconstruction: Four-Corner Arthrodesis with Headless Screws
Partial Excision of the Triangular Fibrocartilage Complex
Arthrodesis of the Rheumatoid Wrist
Release of the First Dorsal Compartment
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
