Case 30
De Quervain’s Disease
Kevin D. Plancher
History and Clinical Presentation
A 45-year-old right hand dominant woman presents with wrist pain that is preventing her from doing activities at home. She spends a significant amount of time in her garden, and she has noticed increased wrist pain, especially when she uses her thumb. She reports that these symptoms do not improve with rest. She denies any history of trauma to her wrist and has not been diagnosed with rheumatoid arthritis.
Physical Examination
Pain and swelling are localized over the region of the radial styloid (Fig. 30–1). The pain radiates down to the thumb and a thickened fibrous sheath is palpable over the radial styloid. Maximum tenderness is noted over the radial styloid, and tenderness is also noted along the long abductor tendon and muscle. Pain is increased with extension and abduction of the thumb against resistance. A Finkelstein test is positive and produces significant pain (Fig. 30–2).
PEARLS
- Initial management consists of a custom thumb spica splint and additional antiinflammatory medication and a possible corticosteroid injection
- Careful attention to technique during injecting (needle angle and placement)
- Longitudinal septum may divide the APL and the EPB in 20 to 30% of patients.
- Necessary to identify and release both the EPB and APL before closure during surgery
PITFALLS
- Unresponsiveness to corticosteroid injections and recurrent symptoms can occur because of the presence of the longitudinal septum
- Injection not placed correctly will lead to recurrence of symptoms
- Patient falling to follow conservative treatment regiment with hand therapy will in 5% of all patients necessitate surgical release
Diagnostic Studies
Radiographs consisting of a posteroanterior (PA) and lateral view of the wrist as well as the important hyperpronated view or Robert’s view were within normal limits. No carpometacarpal (CMC) arthritis was evident on the Robert’s view.
Differential Diagnosis
Scaphoid fracture
Arthritis
Flexor carpi radialis tendonitis
Thumb carpometacarpal arthritis
Intersection syndrome
Wartenberg’s syndrome

Figure 30–1. Physical exam will localize pain and swelling over the region of the radial styloid.

Figure 30–2. (A) Finkelstein test. (B) Physical exam on a patient.
Diagnosis
De Quervain’s Tenosynovitis of the Right Wrist
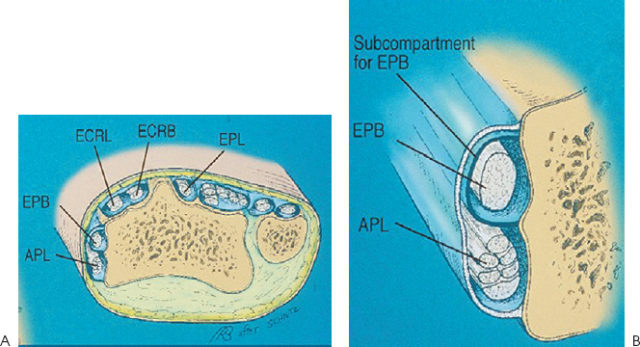
De Quervain’s disease may be caused by any condition that produces a swelling or a thickening of the tendons of the first dorsal compartment of the wrist (Fig. 30–3A). It is a stenosing tenosynovitis of the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons (Fig. 30–3B). This typically occurs in the third, fourth, and fifth decades of life and is 10 times more common in women. The cause is usually related to overuse and may be associated with rheumatoid arthritis. Overuse causes a chronic inflammation of the sheath that covers the long abductor and the short extensor tendons.
The tendons of the APL and the EPB pass through a fibro-osseous tunnel formed by a groove in the radial styloid and overlying extensor retinaculum (Fig. 30–4). The tendons deviate as they pass through the tunnel, and the angle increases with ulnar deviation of the wrist. Anatomic studies of the fibro-osseous canal have documented that in 94% of specimens the abductor pollicis tendon has two to four slips. Multiple EPB tendons are found in only 2%. Multiple subcompartments were recorded in 47% of patients and 75% of specimens. Multiple APL tendon slips and two subcompartments are the rule rather than the exception in normal anatomy.