Cross-Finger Flaps for Digital Soft Tissue Reconstruction
Bassem T. Elhassan
Alexander Y. Shin
Injuries of the fingertips are very common occurrences secondary to both domestic and industrial accidents and are among the most common hand injuries encountered in the emergency room and the hand practice. To function properly, the fingertip requires adequate padding with durable, sensate skin coverage. As such, any reconstructive procedure of the fingertip must include the provision of durable skin coverage, preservation of adequate sensation, maintenance of finger length, prevention of proximal joint stiffness, and restoration of cosmesis when possible.
Several techniques have been described to address tissue loss of the fingertips. These techniques include direct wound approximation, healing by secondary intention (i.e., allowing the wound to granulate), split and full thickness skin grafting, cross-finger and reverse cross (deepithelialized) finger flaps, adipofascial turnover flaps, revision amputation, volar V-Y advancement flap, Kutler’s bilateral V-Y advancement, vascularized island flaps (homodigital flaps), and partial toe transfers (1,2,3,4,5,6). Each technique has its own indications and contraindications depending on the size of soft tissue loss and the concomitant injuries (exposed bone, tendon, nerve, or vessels).
Cross-finger flaps are local flaps that can reliably provide padding and durable cover for fingertip injuries and have been in use for over 50 years (7,8). The anatomy, indications and contraindications, technique, and results of treatment of the cross-finger flap and the reverse (deepithelized) cross-finger flap for coverage of fingertip injuries will be described.
Anatomy
Cross-Finger Flap
The cross-finger flap is a random local (regional) flap that is usually raised from the dorsum of the donor finger at the level of the proximal or middle phalanx. The blood supply of this flap is from the many small vessels of the subdermal and subcutaneous plexus. These plexi are fed by two major blood supplies. The first is the dorsal digital arteries that originate from the dorsal metacarpal arteries, which in turn originate from the dorsal carpal arterial arch. These branches mostly feed the plexus covering the skin and subcutaneous tissues of the dorsum of the proximal phalanx. The second blood supply is the proper digital arteries, which feed the plexus of vessels covering the skin and subcutaneous of the dorsum of the middle and distal phalanges.
When used as an innervated flap, the cross-finger flap derives its innervation from the sensory innervation of the dorsum of the hand (9,10). The superficial branch of the radial nerve and the dorsal sensory branch of the ulnar nerve innervate the dorsum of the hand up to the level of the proximal one-third of the dorsal skin of the proximal phalanx. Distal to this point, most of the innervation comes from the proper digital nerves through dorsal and distal branches (Figs. 20-1 and 20-2).
Reverse Cross-Finger Flap
The flap used for reverse cross-finger flap consists of the same tissues used for the standard cross-finger flap but without the covering skin, and thus has also been called a deepithelialized cross-finger
flap. The subdermal plexus becomes the main blood supply to this flap, fed by branches of the dorsal digital arteries and the proper digital arteries as previously described.
flap. The subdermal plexus becomes the main blood supply to this flap, fed by branches of the dorsal digital arteries and the proper digital arteries as previously described.
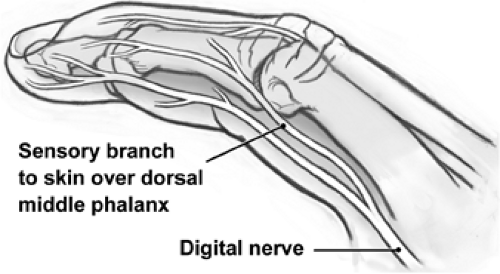 FIGURE 20-1 Innervation to the dorsum of the middle and distal phalanges from the proper digital nerves through dorsal and distal branches. (Reproduced with permission of the Mayo Foundation, 2005.) |
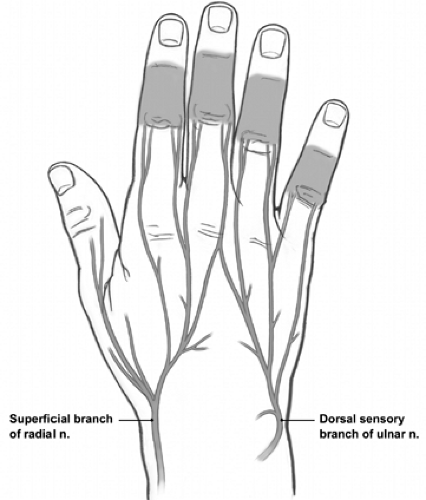 FIGURE 20-2 Innervation to the dorsum of the hand and dorsum of the proximal fingers from branches of the radial and ulnar nerves. (Reproduced with permission of the Mayo Foundation, 2005.) |
Indications/Contraindications
Cross-Finger Flap
A cross-finger flap can be used any age group. In the pediatric patient, its use is reported to be successful as early as the first year of life (11). Some authors have recommended alternative tissue coverage in patients older than 50 years because of the risk of development of persistent postoperative stiffness at the proximal interphalangeal (IP) joint (12,13).
The main indication for this flap coverage is a volar fingertip wound with a major loss of skin and subcutaneous tissue with exposed bones and/or tendons. It can also be used for volar defects of the middle phalanx.
As a random flap, the base is longer than the limbs of the flap. Thus, the entire dorsal skin of the finger can be raised and used. However, if the flap includes skin from the dorsal creases of the IP joints, the resultant dorsal scar may lead to stiffness and possible flexion contracture. It is recommended that the flap be raised between the IP creases. The flap’s size therefore varies from patient to patient and depends on the size of the finger.
Multiple injuries to the hand involving the potential donor finger
Vasospastic conditions such as Raynaud disease and Berger disease
Preexisting disabling problem such as Dupuytren contracture
Advanced age, diabetes mellitus, and rheumatoid arthritis are considered relative contraindications.
Reverse Cross-Finger Flap
A reverse cross-finger flap is indicated in adults with defects on the dorsum of the finger with major loss of skin and subcutaneous tissue and exposed bones and tendons or a nail bed defect that cannot be covered by other techniques (17).
The best donor site is the dorsum of the middle and proximal phalanges. The skin over the distal interphalangeal (DIP) and proximal interphalangeal (PIP) joints should be avoided because the subcutaneous tissue over these areas is thin and there is higher risk of developing contractures.
The size and contraindications of this flap are similar to those of the cross-finger flap.
Surgery
Cross-Finger Flap
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


