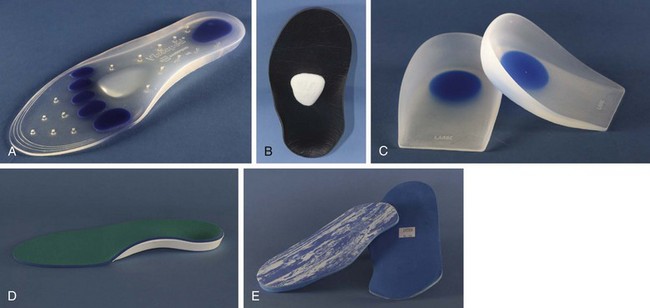
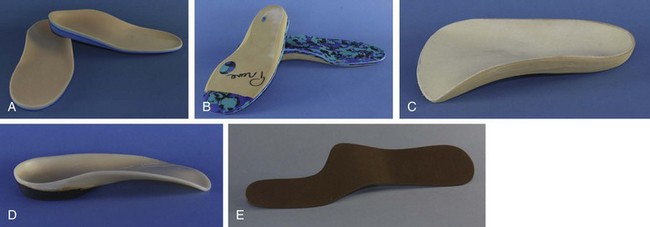
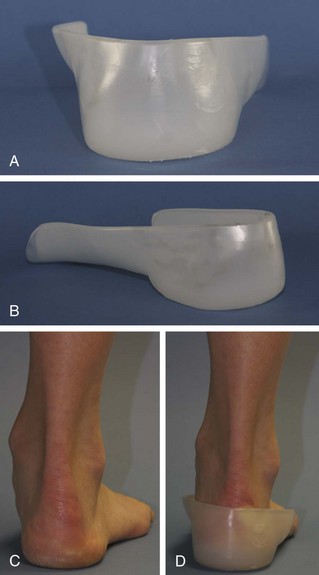
Chapter 4 Conservative treatment of foot and ankle disorders is important and often successful. Nonoperative regimens are relatively inexpensive and can be easily accomplished. The treating physician and surgeon should have thorough knowledge and understanding of the interaction of the foot and the shoe or device applied. Also, the biomechanics of normal foot function and the effect of the disease entity being treated should be analyzed. The anatomy of the normal shoe, the function of each component, and the effect of modifying each of these components must be appreciated.4,5,7,23,24 Furthermore, the practitioner should be familiar with over-the-counter devices as well as with prescribed inserts and orthoses. The desired results of these devices on the foot and ankle should be fully recognized.8,15 The foremost component of conservative treatment begins with patient education about the effects of ill-fitting shoes and high heels. Forefoot loading is increased by the foot sliding forward into the toe box.22 Female patients may not comply with this initial treatment because ill-fitting shoes continue to be inherent in high fashion. It is often necessary to remind patients that, for daily dress, there is no other part of the body they would consider putting in a container whose shape is so drastically different from that body part. A useful tool is comparing an outline of the patient’s foot to his or her current footwear; this is usually effective in conveying this point (Fig. 4-1). Unless the patient is willing to accept that a change in footwear is indicated, both conservative and operative intervention may be futile. Figure 4-1 Comparing the outline of a foot to a woman’s dress shoe demonstrates the disparity in shape. A proper-fitting shoe should accommodate the variations in the person’s foot.16 A set of consumer guidelines has been developed by the National Shoe Retailers Association, the Pedorthic Footwear Association, and the American Orthopaedic Foot and Ankle Society (Table 4-1). It is imperative to measure the shoe with the foot in a standing position because the width of the foot can increase up to two sizes and length by one-half size from the sitting to standing position. In addition, the foot should be measured late in the day because the foot expands in volume as much as 4% by the end of the day. Shoes should be fitted with the normally worn socks. There should be a full finger breadth between the tip of the shoe and the end of the longest toe, with the toes fully extended. Table 4-1 1. Sizes vary among shoe brands and styles. Do not select shoes by the size marked inside the shoe. Judge the shoe by how it fits on your foot. 2. Select a shoe that conforms as nearly as possible to the shape of your foot. 3. Have your feet measured regularly. The size of your feet changes as you grow older. 4. Have both feet measured. For most persons, one foot is larger than the other. Fit to the larger foot. 5. Fit at the end of the day when the feet are largest. 6. Stand during the fitting process and check that there is adequate space ( 7. Make sure the ball of your foot fits snugly into the widest part of the shoe. 8. Do not purchase shoes that feel too tight, expecting them to stretch. 9. Your heel should fit comfortably in the shoe with a minimum amount of slippage. It should be remembered that although orthoses may correct foot position and accommodate deformity, there is no evidence that an orthosis can correct or prevent the development of a hallux valgus or other structural deformities. Also, these devices may not prevent knee, hip, or back arthritis. The goals of foot orthoses include providing shock absorption, cushioning tender areas of the foot, relieving high plantar pressure areas by redistributing weight-bearing pressures covering the entire plantar surface, supporting and protecting healed fracture using the total-contact concept, controlling and supporting flexible deformities, limiting motion of joints, and accommodating fixed deformities with soft moldable materials.17 With the advances in materials used in shoe manufacturing, it is often possible to accomplish many of the goals of orthosis without the expense of custom-molded inlays. Several companies offer padded insoles for shock absorption and heel cushioning (Fig. 4-2). Spenco, Viscopeds, Dr. Scholl’s, and other companies provide padded insoles and inlays that can provide relief for metatarsalgia and fat-pad atrophy. The addition of metatarsal supports, such as the Hapad longitudinal metatarsal pad on a cushioned inlay or in a shoe with a soft sole, can effectively relieve metatarsalgia or neuroma symptoms. Various heel inserts, such as Visco heels or Tuli heel cups, are often helpful in treating plantar heel pain. These devices are readily available through medical supply catalogs and are often found in pharmacies and athletic shoe stores. Patients should be educated on their proper placement and use. If the patient has a deformity or disorder that is not amenable to treatment with an over-the-counter device, a custom orthoses may be appropriate. There are three general types of custom inserts: soft, semirigid, and rigid (Fig. 4-3). Custom orthoses are generally made from a foam impression of the feet of patients, in which the foot is pressed into the foam box evenly. The use of plantar pressure data obtained from new technology with the EMED-D pressure platform (Novel, Munich, Germany) with four sensors/cm2 yields superior off-loading capacity of insoles.20 Another type of foot orthosis is the UCBL insert, which controls flexible postural deformities by controlling the hindfoot.15 The orthosis should be molded with the heel in neutral position. To work successfully, the orthosis must be able to grasp the heel and prevent it from moving into valgus. By keeping the calcaneus in neutral position, the orthosis stiffens the transverse tarsal joints, and pronation and forefoot abduction can be diminished. It may be necessary to add medial posting to the heel and forefoot to keep the heel out of valgus. As medial posting is added, it may be necessary to lower the medial trim line to avoid impingement on the medial malleolus. With fxed deformities, such as arthritis of the midfoot, a UCBL insert can decrease motion and reduce pain. The foot is molded in situ, and the polypropylene should have a relief over the area of bony prominence. The orthosis can be lined with a material for pressure absorption, such as polyurethane foam (PPT) in the relief, and then the entire orthosis can be covered with a material such as polyethylene foam (Plastazote) for comfort (Fig. 4-4). AFOs can be made from double uprights attached to the shoe or molded polypropylene, either as a posterior shell or incorporated into a leather lacer (Arizona brace) (Fig. 4-5). The molded AFO is more potent in most instances. The AFO can be made with a fixed or hinged ankle. The orthosis is manufactured from a positive cast of the lower limb. Modifications can be made through reliefs over bony prominences to accommodate fit, and these can be lined with material to provide comfort and protect the foot and deformity. These modifications of the orthosis allow better control of deformities and expand the use of these orthoses to rigid as well as flexible deformities. A toe crest can be effective in relieving pressure on the tips of the toes from hammer toe and mallet toe deformities. Corn and callus pads can also relieve pressure but are more effective if the overlying callus and corn tissue is removed and the shoe is stretched over the offending prominence or a wider toe box is used. Foam or gel (Silipos) sleeves can also effectively relieve pressure (Fig. 4-6). Toe separators can be used, but lamb’s wool can be equally effective between the toes and has the advantage of better absorption of moisture than the separators have.
Conservative Treatment of the Foot
General Considerations

 to
to  inch) for your longest toe at the end of each shoe.
inch) for your longest toe at the end of each shoe.
Foot Orthoses
Over-the-Counter Inserts
Custom Foot Orthoses
University of California Biomechanics Laboratory (UCBL) Foot Orthoses
Ankle–Foot Orthoses
Appliances
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Musculoskeletal Key
Fastest Musculoskeletal Insight Engine