15
Concepts of Joint Mobilization
Robert C. Manske and Justin Rohrberg
1. Discuss the general and applied concepts of peripheral joint mobilization.
2. Define terms and principles of peripheral joint mobilization.
3. Define and describe the convex–concave rule.
4. Define the five grades of mobilization.
5. Identify and describe terms of joint end-feel.
6. Define and describe capsular and noncapsular patterns.
7. Identify common indications and contraindications for mobilization.
8. Discuss the clinical basics and applications of peripheral joint mobilization.
9. Identify and discuss the role of the physical therapist assistant in assisting the physical therapist with the delivery of peripheral joint mobilization.
FUNDAMENTAL PRINCIPLES OF MOBILIZATION
A healthy joint is one that moves without limitation. In synovial joints, movement stimulates biological activity by moving synovial fluid to areas of avascular articular cartilage. Additionally, strength and resiliency of capsular tissue and periarticular tissue is maintained via joint movement. Immobilization causes a host of negative consequences such as fatty infiltration, articular adhesions, and physiologic changes to the strength and tolerance of ligaments, tendons, and capsular tissue. The term mobilization refers to an attempt to restore joint motion or mobility, or decrease pain associated with joint structures using manual, passive accessory-joint movement.4,21
Joint mobilizations are passive, skilled manual therapy techniques applied to joints and related soft tissues at varying speeds and amplitudes using physiologic or accessory motions for therapeutic purposes.1 Range of motion (ROM) involves physiologic movements which are active/passive motions at a given joint through one of the traditional cardinal planes of flexion, extension, abduction, adduction, or internal and external rotation. Physiologic movements are sometimes called osteokinematic, classical, or traditional movements because they are movements of the actual bones of a given joint system. These motions can be visualized by the naked eye and are commonly measured by goniometric assessment. Osteokinematic motions occur in the cardinal planes of movement such as frontal, sagittal, and transverse. Hip, knee, and shoulder flexion movements are examples of osteokinematic movements. These are all movements that can occur under volitional control. Arthrokinematic movements are those that occur at the bone ends, without regard to the movement. These movements are not under volitional control. These types of movements are known as accessory movements involving motions specific to articulating joint surfaces.4,21 These accessory joint motions are referred to as glide or slide, spin, and roll.4,14 Because these are passive movements at the actual joint level, they are sometimes referred to as arthrokinematic motions. Accessory and physiologic joint motions occur together during active ROM. If full accessory motion does not occur, there will be a limitation in normal physiological cardinal plane movements. However, accessory joint motion cannot be selectively recruited, meaning that a patient cannot selectively perform joint roll, glide, or spin independently on their own.4 The application of accessory joint motion is defined as “joint play” or “motion that occurs within the joint as a response to an outside force but not as a result of voluntary movement.”4
JOINT CONGRUENCY AND POSITION
The concept of joint congruency and the terms close-packed and loose-packed, referring to joint position, are pertinent to the discussion of various grades of mobilization. Congruence refers to articular position with regard to concave and convex joint surfaces. A joint is congruent when both articulating surfaces are in contact throughout the total surface area of the joint.4,14 However, the study of arthrokinematics (joint movement) states that joints are rarely in total congruence. As joints move, the accessory motions of glide or slide, spin, and roll alter total joint congruence.
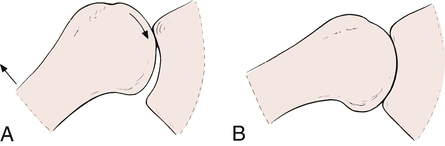
MacConaill and Basmajian14 have described close-packed positions as the most congruent positions of a joint,4,14 where the joint articular surfaces are aligned and the capsule and ligaments are taut and joint volume is minimal (Fig. 15-1). Generally, a close-packed position is used for testing the integrity and stability of ligaments and capsular structures. However, the close-packed position described by MacConaill and Basmajian14 is not used for mobilization techniques. The close-packed position is one of stability. When the elbow and knee are fully extended, the ligaments and joint capsule are taut, allowing no freedom of movement. Therefore the knee and elbow in extension serve as two excellent examples of joints in the close-packed position.
Any joint position other than the close-packed position is a loose-packed position. The position in which the joint capsule and ligaments are most relaxed, loose, and allow the maximum amount of joint play is referred to as the joint’s resting position.4 When the knee joint is flexed to 30°, the intracapsular space is increased and supporting ligaments become more relaxed. The loose-packed position is ideal for applying joint mobilization techniques, but painful, stiff, and dysfunctional joints are rarely in ideal resting positions for the application of joint mobilization. Table 15-1 lists resting and close-packed positions of major joints in the human body.16 If a joint has a limitation of arthrokinematic movement in which the close-packed position cannot be achieved, ground reaction forces and gravitational forces are not distributed through the joint in an optimal manner, thus additional stress and work has to be taken up by the periarticular muscles. If this dysfunctional movement pattern continues, a condition of muscle overuse can ensue.
Table 15-1
Resting (Loose) and Closed-Packed Position of Joints
| Joint | Resting Position | Closed-Packed Position |
| Facet (spine) | Midway between flexion and extension | Extension |
| Temporomandibular | Mouth slightly open (freeway space) | Clenched teeth |
| Glenohumeral | 55° abduction, 30° horizontal adduction | Abduction and lateral rotation |
| Acromioclavicular | Arm resting by side in normal physiologic position | Arm abducted to 90° |
| Sternoclavicular | Arm resting by side in normal physiologic position | Maximum shoulder elevation |
| Ulnohumeral (elbow) | 70° flexion, 10° supination | Extension |
| Radiohumeral | Full extension, full supination | Elbow flexed 90°, forearm supinated 5° |
| Proximal radioulnar | 70° flexion, 35° supination | 5° supination |
| Distal radioulnar | 10° supination | 5° supination |
| Radiocarpal (wrist) | Neutral with slight ulnar deviation | Extension with radial deviation |
| Carpometacarpal | Midway between abduction-adduction and flexion-extension | |
| Metacarpophalangeal (all) | Slight flexion | |
| Metacarpophalangeal (fingers) | Full flexion | |
| Metacarpophalangeal (thumb) | Full opposition | |
| Interphalangeal | Slight flexion | Full extension |
| Hip | 30° flexion, 30° abduction, slight lateral rotation | Full extension, medial rotation |
| Knee | 25° flexion | Full extension, lateral rotation of tibia |
| Talocrural (ankle) | 10° plantarflexion, midway between maximum inversion and eversion | Maximum dorsiflexion |
| Subtalar | Midway between extremes of range of motion | Supination |
| Midtarsal | Midway between extremes of range of motion | Supination |
| Tarsometatarsal | Midway between extremes of range of motion | Supination |
| Metatarsophalangeal | Neutral | Full extension |
| Interphalangeal | Slight flexion | Full extension |
From Magee DJ: Orthopedic physical assessment, ed 5, St Louis, 2008, Saunders.
CONVEX–CONCAVE RULE
Anatomically, all articular surfaces are either convex or concave,4,21 although the surfaces of some joints are not overtly of either shape. In these cases, fibrocartilage enhances and modifies the contour of the joint surfaces. On the convex joint surface, more cartilage is found at the center of the surface; on a concave joint surface, more cartilage is found at the periphery.4
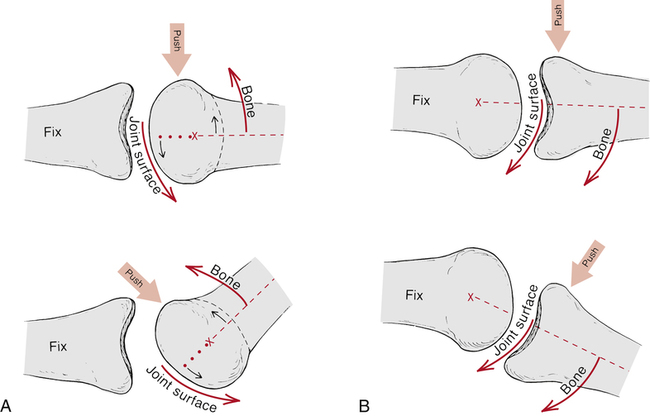
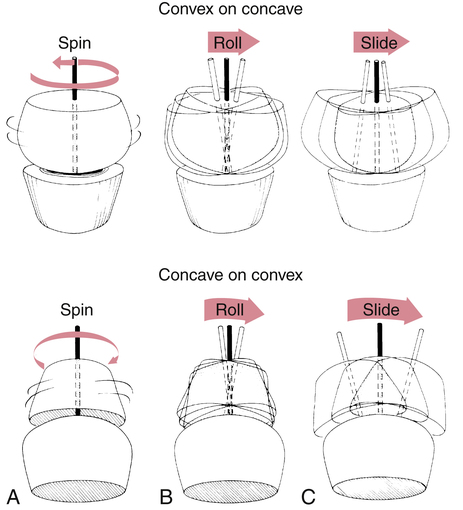
The convex–concave rule specifically states, “When the concave surface is stationary and the convex surface is moving, the gliding movement in the joint occurs in a direction opposite to the bone movement.”4 Conversely, if the convex surface is fixed while the concave surface is mobile, the gliding motion occurs in the same direction as the bone movement.4 This occurs because the convex bone surface always maintains an axis of rotation during joint motion (Fig. 15-2). The concept of accessory joint motions (glide or slide, spin, and roll), as they apply to joint congruency and the convex–concave rule, is clearly illustrated by MacConaill’s classification of accessory movements (Fig. 15-3).
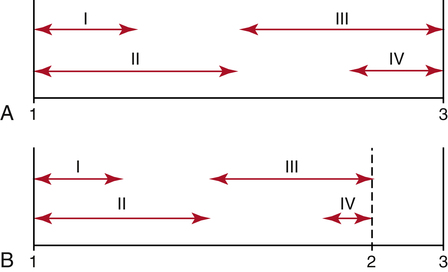
MOBILIZATION GRADES
Maitland17 describes five grades of physiologic and accessory joint motions used in mobilization (Fig. 15-4). The terms velocity, oscillation, and amplitude of movement describe the degree of force and rate of motion used during any of the grades of mobilization, as follows: